Situation Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Democratic Republic of Congo Constitution
THE CONSTITUTION OF THE DEMOCRATIC REPUBLIC OF THE CONGO, 2005 [1] Table of Contents PREAMBLE TITLE I GENERAL PROVISIONS Chapter 1 The State and Sovereignty Chapter 2 Nationality TITLE II HUMAN RIGHTS, FUNDAMENTAL LIBERTIES AND THE DUTIES OF THE CITIZEN AND THE STATE Chapter 1 Civil and Political Rights Chapter 2 Economic, Social and Cultural Rights Chapter 3 Collective Rights Chapter 4 The Duties of the Citizen TITLE III THE ORGANIZATION AND THE EXERCISE OF POWER Chapter 1 The Institutions of the Republic TITLE IV THE PROVINCES Chapter 1 The Provincial Institutions Chapter 2 The Distribution of Competences Between the Central Authority and the Provinces Chapter 3 Customary Authority TITLE V THE ECONOMIC AND SOCIAL COUNCIL TITLE VI DEMOCRACY-SUPPORTING INSTITUTIONS Chapter 1 The Independent National Electoral Commission Chapter 2 The High Council for Audiovisual Media and Communication TITLE VII INTERNATIONAL TREATIES AND AGREEMENTS TITLE VIII THE REVISION OF THE CONSTITUTION TITLE IX TRANSITORY AND FINAL PROVISIONS PREAMBLE We, the Congolese People, United by destiny and history around the noble ideas of liberty, fraternity, solidarity, justice, peace and work; Driven by our common will to build in the heart of Africa a State under the rule of law and a powerful and prosperous Nation based on a real political, economic, social and cultural democracy; Considering that injustice and its corollaries, impunity, nepotism, regionalism, tribalism, clan rule and patronage are, due to their manifold vices, at the origin of the general decline -

WEEKLY BULLETIN on OUTBREAKS and OTHER EMERGENCIES Week 28: 6 - 12 July 2020 Data As Reported By: 17:00; 12 July 2020
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 28: 6 - 12 July 2020 Data as reported by: 17:00; 12 July 2020 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 110 100 10 New event Ongoing events Outbreaks Humanitarian crises 19 195 1 011 Algeria 64 3 1 0 657 0 5 275 147 Gambia 7 0 880 75 1 099 68 Mauritania 50 0 2 411 121 Senegal 304 1 232 0Eritrea 8 135 148 Niger 8 397 39 Mali 1 698 19 Burkina Faso 82 1 0 10 7 0 Cabo Verdé Guinea 1 033 53 53 0 Chad 7 766 128 5 644 14 4 1 32 558 740 29 0 Nigeria 6 141 37Côte d’Ivoire South Sudan 1 873 895 15 4 288 53 337 2 32 0 Guinea-Bissau Ghana 1 054 232 15 173 359 11 427 176 720 15 1 150 0 2 0 19 0 Central African 27 0 Liberia 12 766 84 22 0 2 148 41 Benin Cameroon Republic 916 2 Ethiopia 1 842 63 24 518 139 420 14 Sierra léone Togo 21 219 83 1 175 11 Uganda 980 45 Democratic Republic 40 18 694 3 1 378 26 421 2 10 105 185 17 0 of Congo 1 635 62 1 1 Congo 1 025 0 Gabon 682 6 Kenya 49 20 685 13 Legend 1 010 51 9 0 202 10 37 0 5 942 46 65 004 919 Rwanda Measles Humanitarian crisis 1 337 4 2 103 47 11 773 169 Burundi 729 12 100 0 Hepatitis E Monkeypox 258 1 8 033 188 Seychelles Sao Tome 126 0 Yellow fever Tanzania 857 0 70 0 Lassa fever and Principe 509 21 34 7 Dengue fever Cholera 1 702 47 1 043 12 Angola Ebola virus disease Comoros cVDPV2 Equatorial 2 364 38 317 7 132 0 2 0 Chikungunya Guinea 696 0 COVID-19 Malawi 506 26 Zambia Mozambique Guinea Worm 1 895 42 Anthrax Leishmaniasis Zimbabwe 2 625 21 Madagascar Malaria Namibia Floods Plague 319 1 Botswana 985 18 342 10 Cases Crimean-Congo -
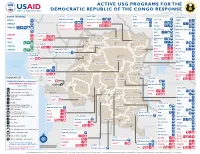
ACTIVE USG PROGRAMS for the DEMOCRATIC REPUBLIC of the CONGO RESPONSE Last Updated 07/27/20
ACTIVE USG PROGRAMS FOR THE DEMOCRATIC REPUBLIC OF THE CONGO RESPONSE Last Updated 07/27/20 BAS-UELE HAUT-UELE ITURI S O U T H S U D A N COUNTRYWIDE NORTH KIVU OCHA IMA World Health Samaritan’s Purse AIRD Internews CARE C.A.R. Samaritan’s Purse Samaritan’s Purse IMA World Health IOM UNHAS CAMEROON DCA ACTED WFP INSO Medair FHI 360 UNICEF Samaritan’s Purse Mercy Corps IMA World Health NRC NORD-UBANGI IMC UNICEF Gbadolite Oxfam ACTED INSO NORD-UBANGI Samaritan’s WFP WFP Gemena BAS-UELE Internews HAUT-UELE Purse ICRC Buta SCF IOM SUD-UBANGI SUD-UBANGI UNHAS MONGALA Isiro Tearfund IRC WFP Lisala ACF Medair UNHCR MONGALA ITURI U Bunia Mercy Corps Mercy Corps IMA World Health G A EQUATEUR Samaritan’s NRC EQUATEUR Kisangani N Purse WFP D WFPaa Oxfam Boende A REPUBLIC OF Mbandaka TSHOPO Samaritan’s ATLANTIC NORTH GABON THE CONGO TSHUAPA Purse TSHOPO KIVU Lake OCEAN Tearfund IMA World Health Goma Victoria Inongo WHH Samaritan’s Purse RWANDA Mercy Corps BURUNDI Samaritan’s Purse MAI-NDOMBE Kindu Bukavu Samaritan’s Purse PROGRAM KEY KINSHASA SOUTH MANIEMA SANKURU MANIEMA KIVU WFP USAID/BHA Non-Food Assistance* WFP ACTED USAID/BHA Food Assistance** SA ! A IMA World Health TA N Z A N I A Kinshasa SH State/PRM KIN KASAÏ Lusambo KWILU Oxfam Kenge TANGANYIKA Agriculture and Food Security KONGO CENTRAL Kananga ACTED CRS Cash Transfers For Food Matadi LOMAMI Kalemie KASAÏ- Kabinda WFP Concern Economic Recovery and Market Tshikapa ORIENTAL Systems KWANGO Mbuji T IMA World Health KWANGO Mayi TANGANYIKA a KASAÏ- n Food Vouchers g WFP a n IMC CENTRAL y i k -

UNJHRO) MONUSCO – OHCHR March 2021 REPORTED HUMAN RIGHTS VIOLATIONS in DEMOCRATIC REPUBLIC of the CONGO (DRC)
Protection of civilians: Human rights violations documented in provinces affected by conflict United Nations Joint Human Rights Office in the DRC (UNJHRO) MONUSCO – OHCHR March 2021 REPORTED HUMAN RIGHTS VIOLATIONS IN DEMOCRATIC REPUBLIC OF THE CONGO (DRC) Figure 1. Percentage of violations per territory Figure 2. Number of violations per province in DRC SOUTH CENTRAL AFRICAN REPUBLIC SUDAN North Kivu Tanganyika Bas-Uele Haut-Uele Masisi 79% 21 Kalemie 36% 65 North-Ubangi Beni 64 36 Manono0 100 2 UGANDA CAMEROON South-Ubangi Rutshuru 69 31 Moba0 100 Ituri Mongala Lubero 29 71 77 Nyiragongo 86 14 Maniema Tshopo Walikale 90 10 Kabambare 63% 395 CONGO Equateur North Butembo0 100 Kasongo0 100 Kivu Kibombo0 100 GABON Tshuapa 359 South Kivu RWANDA Kasai Shabunda 82% 18 Mai-Ndombe Kamonia (Kas.)0 100% Kinshasa Uvira 33 67 5 BURUNDI Llebo (Kas.)0 100 Sankuru 15 63 Fizi 33 67 Kasai South Tshikapa (Kas.)0 100 Maniema Kivu Kabare 100 0 Luebo (Kas.)0 100 Kwilu 23 TANZANIA Walungu 29 71 Kananga (Kas. C)0 100 Lomami Bukavu0 100 22 4 Demba (Kas. C)0 100 Kongo 46 Mwenga 67 33 Central Luiza (Kas. C)0 100 Kwango Tanganyika Kalehe0 100 Kasai Dimbelenge (Kas. C)0 100 Central Haut-Lomami Ituri Miabi (Kas. O)0 100 Kasai 0 100 ANGOLA Oriental Irumu 88% 12 Mbuji-Mayi (Kas. O) Haut- Djugu 64 36 Lualaba Bas-Uele Katanga Mambasa 30 70 Buta0 100% Mahagi 100 0 % by armed groups % by State agents The boundaries and names shown and designations ZAMBIA used on this map do not imply official endorsement or acceptance by the United Nations. -

Download File
UNICEF DRC | COVID-19 Situation Report COVID-19 Situation Report #9 29 May-10 June 2020 /Desjardins COVID-19 overview Highlights (as of 10 June 2020) 25702 • 4.4 million children have access to distance learning UNI3 confirmed thanks to partnerships with 268 radio stations and 20 TV 4,480 cases channels © UNICEF/ UNICEF’s response deaths • More than 19 million people reached with key messages 96 on how to prevent COVID-19 people 565 recovered • 29,870 calls managed by the COVID-19 Hotline • 4,338 people (including 811 children) affected by COVID-19 cases under 388 investigation and 837 frontline workers provided with psychosocial support • More than 200,000 community masks distributed 2.3% Fatality Rate 392 new samples tested UNICEF’s COVID-19 Response Kinshasa recorded 88.8% (3,980) of all confirmed cases. Other affected provinces including # of cases are: # of people reached on COVID-19 through North Kivu (35) South Kivu (89) messaging on prevention and access to 48% Ituri (2) Kongo Central (221) Haut RCCE* services Katanga (38) Kwilu (2) Kwango (1) # of people reached with critical WASH Haut Lomami (1) Tshopo (1) supplies (including hygiene items) and services 78% IPC** Equateur (1) # of children who are victims of violence, including GBV, abuse, neglect or living outside 88% DRC COVID-19 Response PSS*** of a family setting that are identified and… Funding Status # of children and women receiving essential healthcare services in UNICEF supported 34% Health facilities Funds # of caregivers of children (0-23 months) available* DRC COVID-19 reached with messages on breadstfeeding in 15% 30% Funding the context of COVID-19 requirements* : Nutrition $ 58,036,209 # of children supported with distance/home- 29% based learning Funding Education Gap 70% 0% 20% 40% 60% 80% 100% *Funds available include 9 million USD * Risk Communication and Community Engagement UNICEF regular ressources allocated by ** Infection Prevention and Control the office for first response needs. -

Province Du Maindombe
RÉPUBLIQUE DÉMOCRATIQUE DU CONGO - Province du Maindombe - Carte de Référence NIGE RIA Ubangui Lomela CENT RAL SO UTH S UDA N Lotumbe AF RICA N Territoire Elanga REP UB LIC CAM E ROON Nord -Uba ngi de Bomongo Ba s-Uele Haut- Uele Botende Su d-Ub ang i Lokolia ± Mon gala EQ UATORIA L Itur i Bolaka GUINE A Tshop o UGA NDA Eq uate ur Bokatola Boyera GA BO N CONGO Tshua pa Irebu Nord -Kivu RWA NDA Mai- Ndom be Territoire BURUNDI Sa nkur u Man iema Gombe Boloka Su d-Kivu Imbonga de Boende Kin shasa Kwilu Ka sai Ko ngo Centr al UNITE D REP UB LIC OF Lac Ntomb a Bikoro Kasa Ka sai Lom ami Orien tal Tang anyika TA NZ ANIA Kwa ngo Ka sai Bohoke Boende Centr al Lusako Haut- Lom am i Bowele Luala ba Territoire Itipo Losofi Bombesangi Djom bawuli Territoire Haut- Ka tan ga de Bikoro ANG OLA de Ingende Bongili Batua Pembe Watsi Bunga Boyolo ZA MB IA Bolieko Tweya Bopita Lomunu Salonga Gunda MOZ A MB IQ UE Lokakao Monio Penzele Bongili EQUATEUR Loponde Lukanga Botike Bokenge Djaledjom bo Bokenge Sungu Lis obe Lukolela Liese Djaleompendjele Ikongo-Moke Mompoto Ikongo Ebitale Yosenge Ikongo Batwa Mbuye Pum eniama Pendjwa Koko Bonkende Botuali Bakamba Bosano Longo Ebekoli Mbeye Bosobe Ikoyo Mongero Weti Penge Isake Yembe Bobala Besiro Ekuna Nkos o Bololo Itikala Nseti Wenga Boota Mbolo TSHUAPA Tito Mpese Bebongo Bulaki Lofoloko Mbuse Mputu Botola Nsalele Ilinga Ifumba CONGO Kangala Nkutu Momboyo Bekungu Mpasa Towe Bam bi-Gangi Ibeke-Bolia Busepoka Ew ungu Salonga Bobala Nsaw Bem bo Wafania Mbala Pangi Mbengolo National park Koli Ibeke-Bolia Ibeke Wese -

A Turning Point for Manual Drilling in the Democratic Republic of Congo
Rural Water Supply Network Publication 2020-2 C H Kane & Dr K Danert 2020 A Turning Point for Manual Drilling in the Democratic Republic of Congo Publication 2020-2 Dedication Summary The authors dedicate this publication to Gambo Nayou This publication provides a source of inspiration from a country that (1963 to 2016). tends to otherwise be associated with humanitarian crisis, persistent con- flicts, recurrent civil wars and a generally obsolete road infrastructure. It describes over a decade of pioneering efforts by UNICEF, the Gov- ernment of the Democratic Republic of Congo and partners to intro- duce and professionalise manual drilling. This professionalisation pro- gramme is very important as it is estimated that only 43% of the pop- ulation have access to a basic drinking water service (JMP, 2019). In addition, the majority of the DRC is favourable to manual drilling (42% classified with very high or high potential, and 24% as moderate). The most favourable area for manual drilling is in the western part of Gambo was a man of vision, a person who looked into the future and the country, which has a soft geological layer of considerable extent saw things that many could not even imagine. He passionately and thickness. shared what he knew with others. Over a ten-year period, manual drilling, using the rota-jetting tech- Following his experiences of manual drilling in Niger and Chad, nique, has gone from a little-known technology in the DRC to an ef- Gambo reached out to the Association of Manual Drillers from Chad fective technology that has enabled about 650,000 people to be pro- (Tchadienne pour la Promotion des Entreprises Spécialisées en For- vided with a water service. -

World Bank Document
.. HOLD FOR RELEASE • INTERNATIONAL DEVELOPMENT ASSOCIATION 1818 H STREET. ·N.W, WASHINGTON 25, D. C TE' EPHONE. EXECUTIVE 3-6360 Public Disclosure Authorized I:JA Press Release No. 69/19 Subject: IDA and UNDP financing for May 7, 1969 highway technical assistance in Congo (Kinshasa.) A credit of $6 million from the International Development Association (IDA) and a $1.5 million technical assistance grant from the United Nations Development Programme (UNDP) to the Democratic Republic of the Congo (Kinshasa) will enable th~ Government to take the first steps toward rehabilitating its highway network. Public Disclosure Authorized The Government is contributing the equivalent of $2 million toward the cost of the project. The Congo's major centers of population, production and trade are widely s~nttered and an efficient and extensive transport system is essential if the • c,.·,untry is to be integrated administratively, politically and economically. Tile once efficient rail, river and road transport system has deteriorated since 1.udependence and the difficulties which followed. The condition of the highways Public Disclosure Authorized is particularly acute because of a serious weakening of administration, and lack of maintenance and of equipment replacements. The measures now to be undertaken are of an emergency nature and only a small part of what has to be done to establish a viable highway system and administration. However, they will assure more efficient use of personnel and ·funds being used for highway maintenance and rehabilitation; halt the r~1r:i.d deterioration of some of the most important roads; achieve substantial Public Disclosure Authorized s;.:v-tngs in vehicle operating costs; and will encourage incn:?ased production ~-7 ?emoving potential bottlenecks to economic recovery • • /more \ IDA P.R. -

Assessing the Effectiveness of the United Nations Mission
Assessing the of the United Nations Mission in the DRC / MONUC – MONUSCO Publisher: Norwegian Institute of International Affairs Copyright: © Norwegian Institute of International Affairs 2019 ISBN: 978-82-7002-346-2 Any views expressed in this publication are those of the author. They should not be interpreted as reflecting the views of the Norwegian Institute of International Affairs. The text may not be re-published in part or in full without the permission of NUPI and the authors. Visiting address: C.J. Hambros plass 2d Address: P.O. Box 8159 Dep. NO-0033 Oslo, Norway Internet: effectivepeaceops.net | www.nupi.no E-mail: [email protected] Fax: [+ 47] 22 99 40 50 Tel: [+ 47] 22 99 40 00 Assessing the Effectiveness of the UN Missions in the DRC (MONUC-MONUSCO) Lead Author Dr Alexandra Novosseloff, International Peace Institute (IPI), New York and Norwegian Institute of International Affairs (NUPI), Oslo Co-authors Dr Adriana Erthal Abdenur, Igarapé Institute, Rio de Janeiro, Brazil Prof. Thomas Mandrup, Stellenbosch University, South Africa, and Royal Danish Defence College, Copenhagen Aaron Pangburn, Social Science Research Council (SSRC), New York Data Contributors Paul von Chamier, Center on International Cooperation (CIC), New York University, New York EPON Series Editor Dr Cedric de Coning, NUPI External Reference Group Dr Tatiana Carayannis, SSRC, New York Lisa Sharland, Australian Strategic Policy Institute, Canberra Dr Charles Hunt, Royal Melbourne Institute of Technology (RMIT) University, Australia Adam Day, Centre for Policy Research, UN University, New York Cover photo: UN Photo/Sylvain Liechti UN Photo/ Abel Kavanagh Contents Acknowledgements 5 Acronyms 7 Executive Summary 13 The effectiveness of the UN Missions in the DRC across eight critical dimensions 14 Strategic and Operational Impact of the UN Missions in the DRC 18 Constraints and Challenges of the UN Missions in the DRC 18 Current Dilemmas 19 Introduction 21 Section 1. -
Annex A: Democratic Republic of Congo
Annex A. Summary of the Early Grade Reading Materials Survey in the Democratic Republic of the Congo Geography and Demographics 2,344,858 square Size: kilometers (km2) Population: 79 million (2015) Capital: Kinshasa Urban: 43% (2015) Administrative Divisions: 26 provinces Religion: 70% Christian 10% Kimbanguist 10% Muslim 10% Other Source: Central Intelligence Agency (2015). Note: Population and percentages are rounded. Literacy Projected 2013 Primary School 2015 Age Population (aged 11 million Literacy a a 6–11 years): Rates: Overall Male Female Adult (aged 2013 Primary School 77% 89% 66% 113%, up from 53% in 1999 >15 years) GER:a Youth (aged 2013 Pre-primary 86% 92% 80% 4%, up from 1% in 1999 15–24 years) School GER:a Mean: 17.5 (boy)/23.5 (girl) Language: French correct words per minute When: 2014 Oral Reading Standard deviation: Fluency: 2.4 (boy)/2.0 (girl) Sample (formerc) Equateur Where: EGRA Province Results:b 30% zero scores Fewer than 5% reading with ≥80% Reading comprehension Who: 208 students in P4 Comprehension: 69% zero scores Note: EGRA = Early Grade Reading Assessment; GER = Gross Enrollment Rate; P4 = Primary Grade 4. Percentages are rounded. a Source: UNESCO (2015). b Source: RTI International (2015). c In June–July 2015, the country’s 10 provinces were subdivided into 26 provinces. This was the name of the province at the time of data collection. Language Number of Living Languages:a 210 Major Languagesb Estimated Populationc Government Recognized Statusd French 6,080,000 (L2) (2007)e “Official” language 60 DERP in Africa—Reading -

Situation Report
BABAY ZIKA VIRUS SITUATION REPORT YELLOW FEVER 15 JULY 2016 SUMMARY . In Angola, as of 8 July 2016 a total of 3625 suspected cases have been reported, of which 876 are confirmed. The total number of reported deaths is 357, of which 117 were reported among confirmed cases. Suspected cases have been reported in all 18 provinces and confirmed cases have been reported in 16 of 18 provinces and 80 of 125 reporting districts. Mass reactive vaccination campaigns first began in Luanda and have now expanded to cover most of the other affected parts of Angola. Recently, the campaigns have focused on border areas. Despite extensive vaccination efforts circulation of the virus persists. Eleven reactive and pre-emptive mass vaccination campaigns are ongoing in several districts in Benguela, Huambo, Huila, Kwanza Norte, Kwanza Sul, Lunda Norte and Uige provinces. Six other mass vaccination campaigns are nearing completion. Mop-up campaigns are being implemented in parts of the provinces of Cunene, Lunda Norte, Uige and Zaire. Other than an increase in the number of suspected cases recently reported, there are no updates regarding the epidemiological situation in the Democratic Republic of The Congo (DRC). For the last three weeks the national laboratory in DRC has been unable to confirm or discard any suspected cases of yellow fever due to technical issues. According to the latest available information (as of 11 July), the total number of notified suspected cases is 1798, with 68 confirmed cases (as of 24 June) and 85 reported deaths. Cases have been reported in 22 health zones in five of 26 provinces. -

DEMOCRATIC REPUBLIC of the CONGO ! ! ! on Behalf of OCHA ! ! ! !
! ! ! 5-YEAR EVALUATION OF THE CENTRAL EMERGENCY RESPONSE FUND COUNTRY STUDY: DEMOCRATIC REPUBLIC OF THE CONGO ! ! ! On Behalf of OCHA ! ! ! ! ! ! 11 August 2011 Authors: Marie Spaak Augustin Ngendakuriyo ! ! CERF 5-Year Evaluation DRC Country Report ! ! ! This%document%has%been%prepared%by%Channel%Research%as%part%of%the%58Year%Evaluation%of%the% CERF,%commissioned%by%OCHA.%% % This%document%is%public%and%can%be%disseminated.% % Please%address%all%correspondence%to:% % Cecile%Collin,% E8mail:%[email protected]% Tel:%+32%2%633%6529% Fax:%+32%2%633%3092% ! ! ! ! UN!General!Assembly!Resolution!60/124!sets!the!objective!of!the!upgraded!CERF “to ensure a more predictable and timely response to humanitarian emergencies, with the objectives of promoting early action and response to reduce loss of life, enhancing response to time-critical requirements and strengthening core elements of humanitarian response in underfunded crises, based on demonstrable needs and on priorities identified in consultation with the affected State as appropriate” ! Route!des!Marnières!45B,!1380!Ohain,!!Belgium! Tel!+32!2!633!65!29!Fax!+32!2!633!30!92! [email protected]! VAT!No!864!560!703! 2 CERF 5-Year Evaluation DRC Country Report TABLE OF CONTENTS ! TABLE OF CONTENTS ............................................................................................................ 3! ACRONYMS ............................................................................................................................. 4! MAP - DEMOCRATIC