DRC), AFRICA | Ebola Virus Disease Outbreak
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

COD OP Roadcorridor Easter
N ! ! " 0 ! ' ! ! 5 ! 1 2 29°6'0"E 31°9'0"E n Mityana Wakiso ° o 27°55'0"E 28°20'0"E 28°45'0"E 29°10'0"E 29°35'0"E 30°0'0"E 30°25'0"E 30°50'0"E Kiaka 31°15'0"E 31°40'0"E 32°5'0"E 32°30'0"E 0 Biaboye 2 ! Beni! ! Ru! wenzori Hima o ! ! ! ! (!H Kololo 0 N!zenga i ! ! g Ntoyo 2 ! o t N Maboya Mutwanga Busega !\" ! ! 0 4 n ' a ! ! Bapere Vurondo 5 i ! n Kampala 1 l Ombole ! ! ! !Mpigi ° u Barumbi-Opienge ! 0 ZS Biena !Vuhombwe Kasese J u ZS Manguredjipa Kamwenge Kasugho !Kasese ! o ! o 1 p Butembo !Tabili V!uhovi ! ZS Mutwanga 0 !\ ! o C Kakinga ! !Mpondwe ! ! Bashu Entebbe p ! ! TERRITOIRE TERRITOIRE ! ! " ZS Opienge TERRITOIRE ! (!o " 0 Baswaga DE BUTEMBO 0 a ' DE OICHA Kikorongo ' u ! 0 Entebbe 0 l DE LUBERO ° TERRITOIRE ! ° 0 0 DE BAFWASENDE ! ! O U G A N D A ZS Musienene ! e d ! ! Mb! ua ZS Kyondo d !Lukaya Bakumu d'Angumu ! ! !Ibanda ! ! Lubero n e Boli !\ Kiruhura Lugazi ! ! ! o ! Parc National ! i ! u ! de la Maiko K!asugho t ZS Masereka !! Kisaka Amamula ! a ! q ZS Alimbongo !Oninga Masaka ! ! u ! ! i ! ! Lac Edward c S Bamate S " " 0 0 t Bamate ' ! ' a 5 ! Batangi ! 5 2 ZS Lubero 2 ! ° ° v 0 0 a é ! ' Kaseghe r Mbarara Kalisizo Kirumba !Ish!aka ! d ZS Pinga ! K!ikuv!o ! Bushenyi o c ! Bamate ! !Mbarara ! ! !Kayna Kabwohe s ZS Kayna ! o e Kafun!zo t Kanyabayo!nga P R O V I N C E D U ! i ! TERRITOIRE ! Ishasha m ! s Kihihi DE LUBUTU ! ! N O R D - K I V U ! ! ZS Kibirizi !Ishasha Kilambo ! ! s S S é " Bitule ZS Binza " 0 0 ' ' e Rwindi Rukungiri 0 ! 0 l 5 5 ° Isingiro ° d Ntungamo ! 0 ! ! 0 ! ! s Mutukula Wanianga !Kayonza r Kisharo -

Meas, Conservation and Conflict: a Case Study of Virunga National Park
© 2008 International Institute for Sustainable Development (IISD) Published by the International Institute for Sustainable Development MEAs, Conservation and Conflict The International Institute for Sustainable Development contributes to sustainable development by advancing policy recommendations on international trade and investment, economic policy, climate change, A case study of Virunga Nationalmeasurement Park, and DRCassessmen t, and natural resources management. Through the Internet, we report on international negotiations and share knowledge gained through collaborative projects with global partners, resulting in more rigorous research, capacity building in developing countries and better dialogue between North and South. IISD’s vision is better living for all— sustainably; its mission is to champion innovation, enabling societies to live sustainably. IISD is registered as a charitable Alec Crawford organization in Canada and has 501(c)(3) status in the United States. IISD receives core Johannah Bernstein operating support from the Government of Canada, provided through the Canadian International Development Agency (CIDA), the International Development Research Centre October 2008 (IDRC) and Environment Canada; and from the Province of Manitoba. The institute receives project funding from numerous governments inside and outside Canada, United Nations agencies, foundations and the priate sector. International Institute for Sustainable Development 161 Portage Avenue East, 6th Floor Winnipeg, Manitoba Canada R3B 0Y4 Tel: +1 (204) 958–7700 Fax: +1 (204) 958–7710 © 2008 International Institute for Sustainable Development (IISD) Published by the International Institute for MEAs, Conservation Sustainable Development and Conflict The International Institute for Sustainable Development contributes to sustainable A case study of Virunga development by advancing policy recommendations on international trade and investment, economic National Park, DRC policy, climate change, measurement and assessment, and natural resources management. -

The Eastern Border of DR Congo
Geothermal Exploration in D.R. Congo Vikandy S. Mambo Université Officielle de Ruwenzori,,, Butembo, North-Kivu, Eastern Congo 1 Geochemical Study of Thermal Springs in Eastern D. R. Congo • Mambo Vikandy S., (UOR, Butembo) • Kasereka Mahinda, Yalire Mapendano and Wafula Mifundu, (OVG, Goma) 2 Introduction • D.R. Congo is known to be endowed with natural resources: • Minerals • Fresh water • Timber • Electric power is therefore mainly Hydropower Which enormous untapped resources. • In spi te o f l arge resources, on ly 10% o f population use electricity 3 Index map of the western and eastern rifts in Africa 4 Major ‘Great Lakes’ of the East Africa rifts valleys 5 MjMajor volcanoes and dis tr ibu tion of major 20th Century lava flows 6 The most recent eruption • Mt.Nyiragongo eruption – Date : January 17, 2002 – Dea th to ll: 100 peop le (60 dea ths by explosion of petrol stations) – Damages: 30 % of Goma town destroyed or covered with thick lava 7 Vol cani c Disast er in 2002 Lava flow pushes the Lake 100 m as the Lava enters 70 m deep A house couvered with lava (6 personnes died inside)8 Destruction of Goma town, mostly the business area 9 The most recent major earthquakes • Kalehe earthquake occured on October 24, 2002 with 12 deaths •Buk av u ear th quak e on F ebr uar y 3, 2 008 with 44 deaths 10 Damages caused by earthquake in Kalehe (70 km south of Goma) on 24 Oct 2002 11 Earthquake parameters and disaster in Bukavu ● Time ; S und ay F eb . -

Of the United Nations Mission in the DRC / MONUC – MONUSCO
Assessing the of the United Nations Mission in the DRC / MONUC – MONUSCO REPORT 3/2019 Publisher: Norwegian Institute of International Affairs Copyright: © Norwegian Institute of International Affairs 2019 ISBN: 978-82-7002-346-2 Any views expressed in this publication are those of the author. Tey should not be interpreted as reflecting the views of the Norwegian Institute of International Affairs. Te text may not be re-published in part or in full without the permission of NUPI and the authors. Visiting address: C.J. Hambros plass 2d Address: P.O. Box 8159 Dep. NO-0033 Oslo, Norway Internet: effectivepeaceops.net | www.nupi.no E-mail: [email protected] Fax: [+ 47] 22 99 40 50 Tel: [+ 47] 22 99 40 00 Assessing the Efectiveness of the UN Missions in the DRC (MONUC-MONUSCO) Lead Author Dr Alexandra Novosseloff, International Peace Institute (IPI), New York and Norwegian Institute of International Affairs (NUPI), Oslo Co-authors Dr Adriana Erthal Abdenur, Igarapé Institute, Rio de Janeiro, Brazil Prof. Tomas Mandrup, Stellenbosch University, South Africa, and Royal Danish Defence College, Copenhagen Aaron Pangburn, Social Science Research Council (SSRC), New York Data Contributors Ryan Rappa and Paul von Chamier, Center on International Cooperation (CIC), New York University, New York EPON Series Editor Dr Cedric de Coning, NUPI External Reference Group Dr Tatiana Carayannis, SSRC, New York Lisa Sharland, Australian Strategic Policy Institute, Canberra Dr Charles Hunt, Royal Melbourne Institute of Technology (RMIT) University, Australia Adam Day, Centre for Policy Research, UN University, New York Cover photo: UN Photo/Sylvain Liechti UN Photo/ Abel Kavanagh Contents Acknowledgements 5 Acronyms 7 Executive Summary 13 Te effectiveness of the UN Missions in the DRC across eight critical dimensions 14 Strategic and Operational Impact of the UN Missions in the DRC 18 Constraints and Challenges of the UN Missions in the DRC 18 Current Dilemmas 19 Introduction 21 Section 1. -

Download File
UNICEF DRC | COVID-19 Situation Report COVID-19 Situation Report #9 29 May-10 June 2020 /Desjardins COVID-19 overview Highlights (as of 10 June 2020) 25702 • 4.4 million children have access to distance learning UNI3 confirmed thanks to partnerships with 268 radio stations and 20 TV 4,480 cases channels © UNICEF/ UNICEF’s response deaths • More than 19 million people reached with key messages 96 on how to prevent COVID-19 people 565 recovered • 29,870 calls managed by the COVID-19 Hotline • 4,338 people (including 811 children) affected by COVID-19 cases under 388 investigation and 837 frontline workers provided with psychosocial support • More than 200,000 community masks distributed 2.3% Fatality Rate 392 new samples tested UNICEF’s COVID-19 Response Kinshasa recorded 88.8% (3,980) of all confirmed cases. Other affected provinces including # of cases are: # of people reached on COVID-19 through North Kivu (35) South Kivu (89) messaging on prevention and access to 48% Ituri (2) Kongo Central (221) Haut RCCE* services Katanga (38) Kwilu (2) Kwango (1) # of people reached with critical WASH Haut Lomami (1) Tshopo (1) supplies (including hygiene items) and services 78% IPC** Equateur (1) # of children who are victims of violence, including GBV, abuse, neglect or living outside 88% DRC COVID-19 Response PSS*** of a family setting that are identified and… Funding Status # of children and women receiving essential healthcare services in UNICEF supported 34% Health facilities Funds # of caregivers of children (0-23 months) available* DRC COVID-19 reached with messages on breadstfeeding in 15% 30% Funding the context of COVID-19 requirements* : Nutrition $ 58,036,209 # of children supported with distance/home- 29% based learning Funding Education Gap 70% 0% 20% 40% 60% 80% 100% *Funds available include 9 million USD * Risk Communication and Community Engagement UNICEF regular ressources allocated by ** Infection Prevention and Control the office for first response needs. -

Democratic Republic of the Congo of the Congo Democratic Republic
Democratic Republic of the Congo of the Congo Democratic Republic Main objectives Impact • UNHCR provided international protection to some In 2005, UNHCR aimed to strengthen the protection 204,300 refugees in the DRC of whom some 15,200 framework through national capacity building, registra- received humanitarian assistance. tion, and the prevention of and response to sexual and • Some of the 22,400 refugees hosted by the DRC gender-based violence; facilitate the voluntary repatria- were repatriated to their home countries (Angola, tion of Angolan, Burundian, Rwandan, Ugandan and Rwanda and Burundi). Sudanese refugees; provide basic assistance to and • Some 38,900 DRC Congolese refugees returned to locally integrate refugee groups that opt to remain in the the DRC, including 14,500 under UNHCR auspices. Democratic Republic of the Congo (DRC); prepare and UNHCR monitored the situation of at least 32,000 of organize the return and reintegration of DRC Congolese these returnees. refugees into their areas of origin; and support initiatives • With the help of the local authorities, UNHCR con- for demobilization, disarmament, repatriation, reintegra- ducted verification exercises in several refugee tion and resettlement (DDRRR) and the Multi-Country locations, which allowed UNHCR to revise its esti- Demobilization and Reintegration Programme (MDRP) mates of the beneficiary population. in cooperation with the UN peacekeeping mission, • UNHCR continued to assist the National Commission UNDP and the World Bank. for Refugees (CNR) in maintaining its advocacy role, urging local authorities to respect refugee rights. UNHCR Global Report 2005 123 Working environment Recurrent security threats in some regions have put another strain on this situation. -

Democratic Republic of the Congo – Ebola Outbreaks SEPTEMBER 30, 2020
Fact Sheet #10 Fiscal Year (FY) 2020 Democratic Republic of the Congo – Ebola Outbreaks SEPTEMBER 30, 2020 SITUATION AT A GLANCE 128 53 13 3,470 2,287 Total Confirmed and Total EVD-Related Total EVD-Affected Total Confirmed and Total EVD-Related Probable EVD Cases in Deaths in Équateur Health Zones in Probable EVD Cases in Deaths in Eastern DRC Équateur Équateur Eastern DRC at End of at End of Outbreak Outbreak MoH – September 30, 2020 MoH – September 30, 2020 MoH – September 30, 2020 MoH – June 25, 2020 MoH – June 25, 2020 Health actors remain concerned about surveillance gaps in northwestern DRC’s Équateur Province. In recent weeks, several contacts of EVD patients have travelled undetected to neighboring RoC and the DRC’s Mai- Ndombe Province, heightening the risk of regional EVD spread. Logistics coordination in Equateur has significantly improved in recent weeks, with response actors establishing a Logistics Cluster in September. The 90-day enhanced surveillance period in eastern DRC ended on September 25. TOTAL USAID HUMANITARIAN FUNDING USAID/BHA1,2 $152,614,242 For the DRC Ebola Outbreaks Response in FY 2020 USAID/GH in $2,500,000 Neighboring Countries3 For complete funding breakdown with partners, see funding chart on page 6 Total $155,114,2424 1USAID’s Bureau for Humanitarian Assistance (USAID/BHA) 2 Total USAID/BHA funding includes non-food humanitarian assistance from the former Office of U.S. Foreign Disaster Assistance. 3 USAID’s Bureau for Global Health (USAID/GH) 4 Some of the USAID funding intended for Ebola virus disease (EVD)-related programs in eastern Democratic Republic of the Congo (DRC) is now supporting EVD response activities in Équateur. -
Understanding People's Resistance to Ebola Responses in The
FROM BIOLEGITIMACY TO ANTIHUMANITARIANISM | MAY 2021 Photo by: Ernest Katembo Ngetha. From Biolegitimacy to Antihumanitarianism: Understanding People’s Resistance to Ebola Responses in the Democratic Republic of the Congo Aymar Nyenyezi Bisoka, Koen Vlassenroot, and Lucien Ramazani 8 Congo Research Briefs | Issue 8 FROM BIOLEGITIMACY TO ANTIHUMANITARIANISM: UNDERSTANDING PEOPLE’S RESISTANCE TO EBOLA RESPONSES IN THE DEMOCRATIC REPUBLIC OF THE CONGO Aymar Nyenyezi Bisoka, Koen Vlassenroot, and Lucien Ramazani1 INTRODUCTION authorities and their ineffectiveness in providing security and creating The tenth outbreak of Ebola hemorrhagic fever in the Democratic lasting peace in areas hit by conflict. In such areas, people prioritize Republic of the Congo (DRC) officially started in August 2018 security above health provisions and feel abandoned by those they in the eastern province of North Kivu, leading the World Health expect to care about them. As one respondent told us, “we die more Organization (WHO), on July 17, 2019, to recognize it as a “public from war than from Ebola and no one cares about it.”4 The local health emergency of international concern.”2 At its formal conclusion population experienced the Ebola health crisis as an opportunity not on June 26, 2020, the pandemic had resulted in 3,470 reported to aim for better health care but to demand protection and peace. cases, including 2,287 deaths.3 Despite its devastating impact, local These observations tell us that, rather than accepting the health- populations seemed to be skeptical about the existence of the new care priorities of humanitarian interventions, people living in North pandemic. Consequently, the outbreak saw substantial and often Kivu saw the pandemic as a moment of struggle and resistance fierce local resistance to the medical response, including armed and mobilized to express their demands to a wide range of public attacks on Ebola treatment centers (ETCs) and violence toward authorities. -

MONUSCO, 20 Years in Democratic Republic of Congo. What
MONUSCO, 20 Years in Democratic Republic of Congo. What Are the Priorities For Its New Mandate? Analysis December 2019 / N° 746a Cover picture: The gates to the MONUSCO headquarters in Kinshasa, Democratic Republic of Congo (DRC), 19 February 2015. © Michael Kappeler / DPA/DPA Picture Alliance TABLE OF CONTENTS ACRONYMS 5 MAP OF MONUSCO’S PRESENCE IN DRC 6 EXECUTIVE SUMMARY 7 METHODOLOGY 9 INTRODUCTION 10 I. OVERVIEW OF THE POLITICAL, SECURITY AND HUMAN RIGHTS CONTEXT IN DRC 12 A. An uncertain context of emergence from political crisis and lifting of restrictions on democratic space 12 B. A worrying security context, marked by continuing violations of human rights and inter-communal tensions and conflicts throughout the country 14 II. OVERVIEW OF THE CONTEXT OF RENEWAL OF MONUSCO’S MANDATE 18 A. A nine-month interim mandate 18 B. Towards MONUSCO’s reconfiguration 19 III. PRIORITIES FOR THE NEW MONUSCO MANDATE ACCORDING TO FIDH AND ITS MEMBER ORGANISATIONS IN DRC 21 A. On democratic space and governance 21 1. Consolidate efforts already undertaken to open up democratic space 21 2. Encourage institutional reforms 22 B. On security and civilian protection 24 1. Prioritise a non-military community-based and local approach to civilian protection 24 2. Strengthen civil and military coordination 25 3. Provide a rapid response to protection needs 26 4. Adopt a regional approach to civilian protection 26 5. Pursue efforts to reform the UN peacekeeping system 26 C. On justice and the fight against impunity 27 1. Fight impunity for the most serious crimes 27 2. Build the capacities of the judicial system to increase its efficiency and independence 29 3. -

Report on Violations of Human Rights and International Humanitarian Law by the Allied Democratic Forces Armed
UNITED NATIONS JOINT HUMAN RIGHTS OFFICE OHCHR-MONUSCO Report on violations of human rights and international humanitarian law by the Allied Democratic Forces armed group and by members of the defense and security forces in Beni territory, North Kivu province and Irumu and Mambasa territories, Ituri province, between 1 January 2019 and 31 January 2020 July 2020 Table of contents Summary ......................................................................................................................................................................... 4 I. Methodology and challenges encountered ............................................................................................ 7 II. Overview of the armed group Allied Democratic Forces (ADF) ................................................. 8 III. Context of the attacks in Beni territory ................................................................................................. 8 A. Evolution of the attacks from January 2015 to December 2018 .................................................. 8 B. Context of the attacks from 1 January 2019 and 31 January 2020 ............................................ 9 IV. Modus operandi............................................................................................................................................. 11 V. Human rights violations and abuses and violations of international humanitarian law . 11 A. By ADF combattants .................................................................................................................................. -
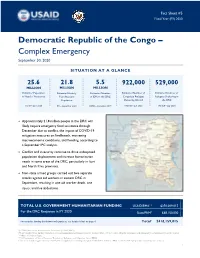
DRC Complex Emergency Fact Sheet #5 09.30.2020
Fact Sheet #5 Fiscal Year (FY) 2020 Democratic Republic of the Congo – Complex Emergency September 30, 2020 SITUATION AT A GLANCE 25.6 21.8 5.5 922,000 529,000 MILLION MILLION MILLION Estimated Population Estimated Acutely Estimated Number Estimated Number of Estimated Number of in Need of Assistance Congolese Refugees Refugees Sheltering in Food Insecure of IDPs in the DRC Population Sheltering Abroad the DRC OCHA – June 2020 UNHCR – July 2020 UNHCR – July 2020 IPC – September 2020 OCHA – December 2019 Approximately 21.8 million people in the DRC will likely require emergency food assistance through December due to conflict, the impact of COVID-19 mitigation measures on livelihoods, worsening macroeconomic conditions, and flooding, according to a September IPC analysis. Conflict and insecurity continue to drive widespread population displacement and increase humanitarian needs in some areas of the DRC, particularly in Ituri and North Kivu provinces. Non-state armed groups carried out two separate attacks against aid workers in eastern DRC in September, resulting in one aid worker death, one injury, and five abductions. TOTAL U.S. GOVERNMENT HUMANITARIAN FUNDING USAID/BHA1,2 $350,009,015 For the DRC Response in FY 2020 State/PRM3 $68,150,000 For complete funding breakdown with partners, see detailed chart on page 6 Total4 $418,159,015 1USAID’s Bureau for Humanitarian Assistance (USAID/BHA) 2 Total USAID/BHA funding includes non-food humanitarian assistance from the former Office of U.S. Foreign Disaster Assistance and emergency food assistance from the former Office of Food for Peace. 3 U.S. Department of State’s Bureau of Population, Refugees, and Migration (State/PRM) 4 This total includes approximately $23,833,699 in supplemental funding through USAID/BHA and State/PRM for COVID-19 preparedness and response activities. -

Bureau De La Division Epst Nord Kivu Ii a Butembo
COMPTE RENDU DE LA REUNION DU SOUS CLUSTER EDUCATION DU 26 FEVRIER 2020 LIEU : BUREAU DE LA DIVISION EPST NORD KIVU II A BUTEMBO Modération : NRC Secrétariat : EADEV AGENDA DE LA REUNION 1. Suivi des recommandations de la dernière réunion: 5 min. 2. Contexte sécuritaire et Alertes en éducation : 15 min 3. Positionnement des acteurs en éducation pour la réponse sur l’axe Mangina : 25 min 4. Plan d’action 2020 du sous cluster éducation au GNK : 30min 5. Activités réalisées par les acteurs et gaps en éducation : 10 min 6. Divers : 5min Participants/Organisation ou institution : UNICEF, L2RCONGO, Days for Girls, ADELUC, CREVF, CEFIDI, UEJEP RDC, NRC, EPST, EADEV, APETAMACO, AHADI RDC, MAAMS, ASOPROSAFD, OCHA, AVSI, ULCDDI, APDS Timing : de 10h40 à 12h30 SUJET DE POINTS DE DISCUSSION RECOMMANDATIONS L’AGENDA (par qui et quand) 1. Présentation des La réunion a été introduite par un mot de bienvenu prononcé par le PROVEDA participants EPST NK II à l’endroit de tous les acteurs présents. Il a aussi exprimé ses attentes vis-à-vis des défis auxquels est confronté le secteur de l’éducation dans le contexte de l’insécurité, la MVE mais aussi au contexte de la gratuité de l’enseignement de base. Une présentation nominative a, par la suite, été faite et c’était le début de l’effectivité de la réunion. SUJET DE RECOMMANDATION (S) RESPONSABLE (S) DE SUIVI ET NIVEAU DE REALISATION L’AGENDA REALISATION 2. Suivi des Du partage d’un rapport de Le rapport est déjà disponible et partagé AVSI et AHADI RD Congo recommandations l’évaluation multisectorielle des de la réunion du besoins en zone d’OICHA mois de janvier Du partage de l’outil 4W aux Le partage n’a pas été fait à cause du NRC 2020 membres du Sous Cluster Education programme du cluster national qui envisage renforcer les capacités des membres du sous cluster éducation sur les outils de collecte des données, y compris le 3 /4W.