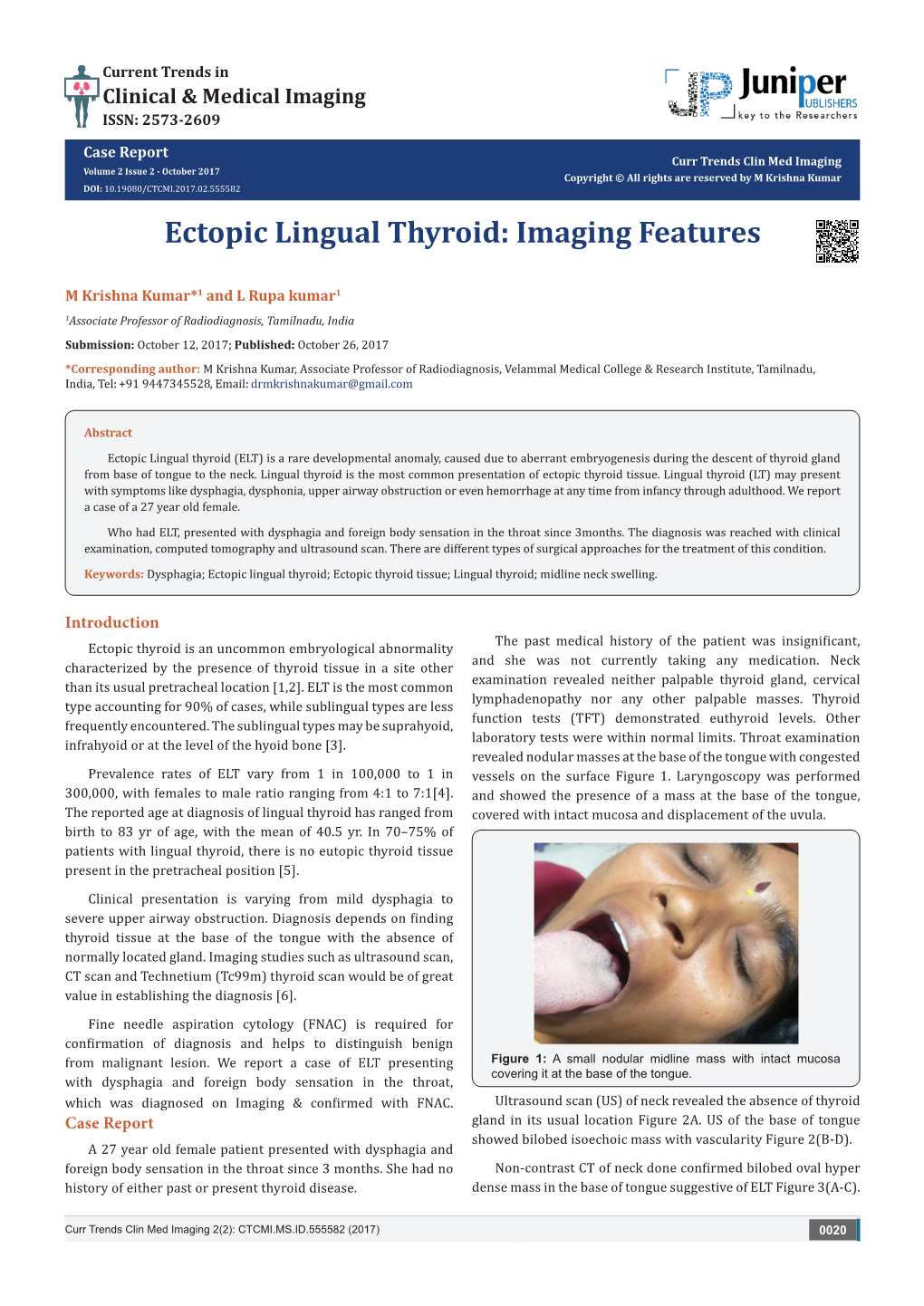
Ectopic Lingual Thyroid: Imaging Features
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ODONTOGENTIC INFECTIONS Infection Spread Determinants
ODONTOGENTIC INFECTIONS The Host The Organism The Environment In a state of homeostasis, there is Peter A. Vellis, D.D.S. a balance between the three. PROGRESSION OF ODONTOGENIC Infection Spread Determinants INFECTIONS • Location, location , location 1. Source 2. Bone density 3. Muscle attachment 4. Fascial planes “The Path of Least Resistance” Odontogentic Infections Progression of Odontogenic Infections • Common occurrences • Periapical due primarily to caries • Periodontal and periodontal • Soft tissue involvement disease. – Determined by perforation of the cortical bone in relation to the muscle attachments • Odontogentic infections • Cellulitis‐ acute, painful, diffuse borders can extend to potential • fascial spaces. Abscess‐ chronic, localized pain, fluctuant, well circumscribed. INFECTIONS Severity of the Infection Classic signs and symptoms: • Dolor- Pain Complete Tumor- Swelling History Calor- Warmth – Chief Complaint Rubor- Redness – Onset Loss of function – Duration Trismus – Symptoms Difficulty in breathing, swallowing, chewing Severity of the Infection Physical Examination • Vital Signs • How the patient – Temperature‐ feels‐ Malaise systemic involvement >101 F • Previous treatment – Blood Pressure‐ mild • Self treatment elevation • Past Medical – Pulse‐ >100 History – Increased Respiratory • Review of Systems Rate‐ normal 14‐16 – Lymphadenopathy Fascial Planes/Spaces Fascial Planes/Spaces • Potential spaces for • Primary spaces infectious spread – Canine between loose – Buccal connective tissue – Submandibular – Submental -

TAR and Non-Benefit List: Codes 40000 Thru 49999 Page Updated: January 2021
tar and non cd4 1 TAR and Non-Benefit List: Codes 40000 thru 49999 Page updated: January 2021 Surgery Digestive System Note: Refer to the TAR and Non-Benefit: Introduction to List in this manual for more information about the categories of benefit restrictions. Lips Excision Code Description Benefit Restrictions 40490 Biopsy of lip Assistant Surgeon services not payable Other Procedures Code Description Benefit Restrictions 40799 Unlisted procedure, lips Requires TAR, Primary Surgeon/ Provider Vestibule of Mouth Incision Code Description Benefit Restrictions 40800 Drainage of abscess/cyst, mouth, simple Assistant Surgeon services not payable 40801 Drainage of abscess/cyst, mouth, complicated Assistant Surgeon services not payable 40804 Removal of embedded foreign body, mouth, simple Assistant Surgeon services not payable 40805 Removal of embedded foreign body, mouth, Assistant Surgeon complicated services not payable 40806 Incision labial frenum Non-Benefit Excision Code Description Benefit Restrictions 40808 Biopsy, vestibule of mouth Assistant Surgeon services not payable 40810 Excision of lesion mucosa/submucosa, mouth, without Non-Benefit repair Part 2 – TAR and Non-Benefit List: Codes 40000 thru 49999 tar and non cd4 2 Page updated: January 2021 Excision (continued) Code Description Benefit Restrictions 40812 Excision of lesion mucosa/submucosa, mouth, simple Assistant Surgeon repair services not payable 40816 Excision of lesion, mouth, mucosa/submucosa, Assistant Surgeon complex services not payable 40819 Excision of frenum, labial -

Deep Neck Space Infection
European Journal of Molecular & Clinical Medicine ISSN 2515-8260 Volume 07, Issue 03, 2020 DEEP NECK SPACE INFECTION- A CLINICAL INSIGHT Correspondance to:Dr.Vijay Ebenezer 1, Professor Head of the department of oral and maxillofacial surgery, Sree balaji dental college and hospital, pallikaranai, chennai-100. Email id: [email protected], Contact no: 9840136328 Names of the author(s): 1)Dr. Vijay Ebenezer1 ,Professor and Head of the department of oral and maxillofacial surgery, Sree Balaji dental college and hospital , BIHER, Chennai-600100, Tamilnadu , India. 2)Dr. Balakrishnan Ramalingam2, professor in the department of oral and maxillofacial surgery, Sree balaji dental college and hospital, pallikaranai, chennai-100. INTRODUCTION Deep neck infections are a life threatening condition but can be treated, the infections affects the deep cervical space and is characterized by rapid progression. These infections remains as a serious health problem with significant morbidity and potential mortality. These infections most frequently has its origin from the local extension of infections from tonsils, parotid glands, cervical lymph nodes, and odontogenic structures. Classically it presents with symptoms related to local pressure effects on the respiratory, nervous, or gastrointestinal (GI) tract (particularly neck mass/swelling/induration, dysphagia, dysphonia, and trismus). The specific presenting symptoms will be related to the deep neck space involved (parapharyngeal, retropharyngeal, prevertebral, submental, masticator, etc).1,2,3,4,5 ETIOLOGY Deep neck space infections are polymicrobial, with their source of origin from the normal flora of the oral cavity and upper respiratory tract. The most common deep neck infections among adults arise from dental and periodontal structures, with the second most common source being from the tonsils. -

Deep Neck Space Infectionsdeep Neck Space Infections
Deep Neck Space InfectionsDeep Neck Space Infections Disclaimer: The pictures used in this presentation and its content has been obtained from a number of sources. Their use is purely for academic and teaching purposes. The contents of this presentation do not have any intended commercial use. In case the owner of any of the pictures has any objection and seeks their removal please contact at [email protected] . These pictures will be removed immediately. The fibrous connective tissue that constitutes the cervical fascia varies from loose areolar tissue to dense fibrous bands. This fascia serves to envelope the muscles, nerves, vessels and viscera of the neck, thereby forming planes and potential spaces that serve to divide the neck into functional units. It functions to both direct and limit the spread of disease processes in the neck. The cervical fascia can be divided into a simpler superficial layer and a more complex deep layer that is further subdivided into superficial, middle and deep layers. The superficial layer of cervical fascia ensheaths the platysma in the neck and extends superiorly in the face to cover the mimetic muscles. It is the equivalent of subcutaneous tissue elsewhere in the body and forms a continuous sheet from the head and neck to the chest, shoulders and axilla. The superficial layer of the deep cervical fascia is also known as the investing layer. It follows the “rule of twos”—it envelops two muscles, two glands and forms two spaces. It originates from the spinous processes of the vertebral column and spreads circumferentially around the neck. -

Suprahyoid and Infrahyoid Neck Overview
Suprahyoid and Infrahyoid Neck Overview Imaging Approaches & Indications by space, the skull base interactions above and IHN extension below are apparent. Neither CT nor MR is a perfect modality for imaging the • PPS has bland triangular skull base abutment without extracranial H&N. MR is most useful in the suprahyoid neck critical foramen involved; it empties inferiorly into (SHN) because it is less affected by oral cavity dental amalgam submandibular space (SMS) artifact. The SHN tissue is less affected by motion compared • PMS touches posterior basisphenoid and anterior with the infrahyoid neck (IHN); therefore, the MR image basiocciput, including foramen lacerum; PMS includes quality is not degraded by movement seen in the IHN. Axial nasopharyngeal, oropharyngeal, and hypopharyngeal and coronal T1 fat-saturated enhanced MR is superior to CECT mucosal surfaces in defining soft tissue extent of tumor, perineural tumor • MS superior skull base interaction includes zygomatic spread, and dural/intracranial spread. When MR is combined with CT of the facial bones and skull base, a clinician can obtain arch, condylar fossa, skull base, including foramen ovale (CNV3), and foramen spinosum (middle meningeal precise mapping of SHN lesions. Suprahyoid and Infrahyoid Neck artery); MS ends at inferior surface of body of mandible CECT is the modality of choice when IHN and mediastinum are • PS abuts floor of external auditory canal, mastoid tip, imaged. Swallowing, coughing, and breathing makes this area including stylomastoid foramen (CNVII); parotid tail a "moving target" for the imager. MR image quality is often extends inferiorly into posterior SMS degraded as a result. Multislice CT with multiplanar • CS meets jugular foramen (CNIX-XI) floor, hypoglossal reformations now permits exquisite images of the IHN canal (CNXII), and petrous internal carotid artery canal; unaffected by movement. -

Complex Odontogenic Infections
Complex Odontogenic Infections Larry ). Peterson CHAPTEROUTLINE FASCIAL SPACE INFECTIONS Maxillary Spaces MANDIBULAR SPACES Secondary Fascial Spaces Cervical Fascial Spaces Management of Fascial Space Infections dontogenic infections are usually mild and easily and causes infection in the adjacent tissue. Whether or treated by antibiotic administration and local sur- not this becomes a vestibular or fascial space abscess is 0 gical treatment. Abscess formation in the bucco- determined primarily by the relationship of the muscle lingual vestibule is managed by simple intraoral incision attachment to the point at which the infection perfo- and drainage (I&D) procedures, occasionally including rates. Most odontogenic infections penetrate the bone dental extraction. (The principles of management of rou- in such a way that they become vestibular abscesses. tine odontogenic infections are discussed in Chapter 15.) On occasion they erode into fascial spaces directly, Some odontogenic infections are very serious and require which causes a fascial space infection (Fig. 16-1). Fascial management by clinicians who have extensive training spaces are fascia-lined areas that can be eroded or dis- and experience. Even after the advent of antibiotics and tended by purulent exudate. These areas are potential improved dental health, serious odontogenic infections spaces that do not exist in healthy people but become still sometimes result in death. These deaths occur when filled during infections. Some contain named neurovas- the infection reaches areas distant from the alveolar cular structures and are known as coinpnrtments; others, process. The purpose of this chapter is to present which are filled with loose areolar connective tissue, are overviews of fascial space infections of the head and neck known as clefts. -

Factors Affecting the Necessity of Tracheostomy in Patients with Deep Neck Infection
diagnostics Article Factors Affecting the Necessity of Tracheostomy in Patients with Deep Neck Infection Shih-Lung Chen 1,2 , Chi-Kuang Young 2,3, Tsung-You Tsai 1,2 , Huei-Tzu Chien 2,4 , Chung-Jan Kang 1,2 , Chun-Ta Liao 1,2 and Shiang-Fu Huang 1,5,* 1 Department of Otorhinolaryngology & Head and Neck Surgery, Chang Gung Memorial Hospital, Linkou 333, Taiwan; [email protected] (S.-L.C.); [email protected] (T.-Y.T.); [email protected] (C.-J.K.); [email protected] (C.-T.L.) 2 School of Medicine, Chang Gung University, Taoyuan 333, Taiwan; [email protected] (C.-K.Y.); [email protected] (H.-T.C.) 3 Department of Otorhinolaryngology, Chang Gung Memorial Hospital, Keelung 204, Taiwan 4 Department of Nutrition and Health Sciences, Chang Gung University of Science and Technology, Taoyuan 333, Taiwan 5 Graduate Institute of Clinical Medical Sciences, Chang Gung University, Taoyuan 333, Taiwan * Correspondence: [email protected]; Tel.: +886-3-3281200 (ext. 3972); Fax: +886-3-3979361 Abstract: Deep neck infection (DNI) is a serious disease that can lead to airway obstruction, and some patients require a tracheostomy to protect the airway instead of intubation. However, no previous study has explored risk factors associated with the need for a tracheostomy in patients with DNI. This article investigates the risk factors for the need for tracheostomy in patients with DNI. Between September 2016 and February 2020, 403 subjects with DNI were enrolled. Clinical findings and critical deep neck spaces associated with a need for tracheostomy in patients with DNI were assessed. -

Immediate Or Delayed Retrieval of the Displaced Third Molar: a Review
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Archivio della ricerca- Università di Roma La Sapienza J Clin Exp Dent. 2019;11(1):e55-61. Immediate/delayed third molar retrieval Journal section: Oral Surgery doi:10.4317/jced.55379 Publication Types: Review http://dx.doi.org/10.4317/jced.55379 Immediate or delayed retrieval of the displaced third molar: A review Dario Di Nardo 1, Giulia Mazzucchi 2, Marco Lollobrigida 2, Claudio Passariello 3, Renzo Guarnieri 2, Massimo Galli 2, Alberto De Biase 2, Luca Testarelli 1 1 DDS, Ph.D. Department of Oral and Maxillo Facial Sciences, “Sapienza” University of Rome, Italy 2 DDS. Department of Oral and Maxillo Facial Sciences, “Sapienza” University of Rome, Italy 3 DDS. Department of Public Health and Infectious Diseases, “Sapienza” University of Rome, Italy Correspondence: Department of Oral and Maxillo Facial Sciences “Sapienza” University of Rome, Italy Via Caserta, 6 - 00161 Rome, ITALY [email protected] Di Nardo D, Mazzucchi G, Lollobrigida M, Passariello C, Guarnieri R, Galli M, De Biase A, Testarelli L. Immediate or delayed retrieval of the dis- placed third molar: A review. J Clin Exp Dent. 2019;11(1):e55-61. http://www.medicinaoral.com/odo/volumenes/v11i1/jcedv11i1p55.pdf Received: 23/10/2018 Accepted: 10/12/2018 Article Number: 55379 http://www.medicinaoral.com/odo/indice.htm © Medicina Oral S. L. C.I.F. B 96689336 - eISSN: 1989-5488 eMail: [email protected] Indexed in: Pubmed Pubmed Central® (PMC) Scopus DOI® System Abstract Background: The displacement of a third molar is a rare occurrence, but it could lead to serious and/or life threate- ning complication. -

Plunging Ranulas Revisited: a CT Study with Emphasis on a Defect Of
Original Article | Neuroimaging and Head & Neck http://dx.doi.org/10.3348/kjr.2016.17.2.264 pISSN 1229-6929 · eISSN 2005-8330 Korean J Radiol 2016;17(2):264-270 Plunging Ranulas Revisited: A CT Study with Emphasis on a Defect of the Mylohyoid Muscle as the Primary Route of Lesion Propagation Ji Young Lee, MD1, 2, Hee Young Lee, MD1, Hyung-Jin Kim, MD1, Han Sin Jeong, MD3, Yi-Kyung Kim, MD1, Jihoon Cha, MD1, Sung Tae Kim, MD1 Departments of 1Radiology and 3Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea; 2Department of Radiology, Hanyang University Hospital, Hanyang University College of Medicine, Seoul 04763, Korea Objective: The purpose of this study was to clarify the pathogenesis of plunging ranulas in regard of the pathway of lesion propagation using CT scans. Materials and Methods: We retrospectively reviewed CT scans of 41 patients with plunging ranula. We divided plunging ranulas into two types: type 1 was defined as those directly passing through a defect of the mylohyoid muscle with the presence (type 1A) or absence (type 1B) of the tail sign and type 2 as those through the traditional posterior route along the free edge of the mylohyoid muscle. Images were also analyzed for the extent of the lesion in respect to the spaces involved. As for type 1 lesions, we recorded the location of the defect of the mylohyoid muscle and the position of the sublingual gland in relation to the defect. Results: CT scans demonstrated type 1 lesion in 36 (88%), including type 1A in 14 and type 1B in 22, and type 2 lesion in 5 (12%). -

Submandibular Abscess Caused by Salmonella Spp. in a Diabetic Patient: a Case Report Abdul-Aziz Alaqeeli, Belal Alani, Moustafa Al Khalil
Case report 129 Submandibular abscess caused by Salmonella spp. in a diabetic patient: a case report Abdul-Aziz Alaqeeli, Belal Alani, Moustafa Al Khalil Department of Craniomaxillofacial Surgery, Head and neck infections normally arise from Streptococcus, Staphylococcus,or Hamad Medical Corporation, Doha, Qatar other anaerobic species, and infection by Salmonella spp. is rare. Patients with Correspondence to Abdul-Aziz Alaqeeli, significant underlying conditions are at increased risk for the development of focal Hamad Medical Corporation, Arab Board of infection. This has been observed in patients with HIV, diabetes, and malignancy. Oral and Maxillofacial Surgery, PO box 3050, Alrayyan Street, Doha, Qatar. Tel: +974 3358 8748; fax: 44397363; Keywords: e-mail: [email protected] Salmonella spp. in the neck Received 3 July 2017 Egypt J Otolaryngol 35:129–132 © Accepted 3 July 2017 2019 The Egyptian Journal of Otolaryngology 1012-5574 The Egyptian Journal of Otolaryngology 2019, 35:129–132 complaining of a progressively enlarging swelling of Introduction the right upper side of the neck with pain, fever, and Head and neck infections normally arise from reduced oral intake since 7 days. Streptococcus, Staphylococcus, or other anaerobic species, and infection by Salmonella spp. is rare. On examination, the patient was conscious, alert, and Nontyphoidal salmonellosis, which is increasing oriented, and not in distress; vitals were within the nowadays in the developed countries, is manifested normal range and had raised body temperature to 38°, as enteritis in most cases, but it also encompasses with no history of recent trauma, dental pain or bacteremia, intra-abdominal infections, and bone, treatment, any abdominal pain, or abnormal bowel joint, and soft tissue infections. -

Imaging of the Sublingual and Submandibular Spaces
Insights into Imaging (2018) 9:391–401 https://doi.org/10.1007/s13244-018-0615-4 REVIEW Imaging of the sublingual and submandibular spaces Swapnil Patel1 & Alok A. Bhatt1 Received: 16 October 2017 /Revised: 19 February 2018 /Accepted: 1 March 2018 /Published online: 19 April 2018 # The Author(s) 2018 Abstract Divided by the mylohyoid muscle, the sublingual and submandibular spaces represent a relatively small part of the oral cavity, but account for a disproportionate amount of pathological processes. These entities are traditionally separated into congenital, infectious/inflammatory, vascular and neoplastic aetiologies. This article reviews the relevant anatomy, clinical highlights and distinguishing imaging features necessary for accurate characterisation. Teaching Points • The mylohyoid sling is a key anatomical landmark useful in surgical planning. • Congenital lesions and infectious/inflammatory processes constitute the majority of pathology. • Depth of invasion is key when staging tumours in the oral cavity. Keywords Head and neck . Salivary glands . Education . CT . MR Introduction Embryology/anatomy The suprahyoid neck is frequently the site of many com- Within the suprahyoid neck, the sublingual and submandibu- mon conditions. Although accessible to clinical exam, lar spaces are the site of a large variety of pathology, given some components are better evaluated with imaging; le- their embryological origin and contents [1]. sions occupying the sublingual space and submandibular The sublingual space is bounded anteriorly by the mandi- space are invisible to the referring clinician. A broad array ble, medially by the midline genioglossus/geniohyoid muscle of pathological processes can occur in these spaces and complex, inferolaterally by the mylohyoid muscle, and pinpointing the origin can narrow the differential and in superomedially by the mucosa of the floor of the mouth and certain cases determine the diagnosis. -

Submandibular Space Infection: a Potentially Lethal Infection
International Journal of Infectious Diseases (2009) 13, 327—333 http://intl.elsevierhealth.com/journals/ijid Submandibular space infection: a potentially lethal infection Paolo Boscolo-Rizzo *, Maria Cristina Da Mosto Department of Medical and Surgical Specialities, Otolaryngology Clinic — Regional Center for Head and Neck Cancer, University of Padua, School of Medicine, Treviso Regional Hospital, Treviso, Italy Received 4 March 2008; received in revised form 19 June 2008; accepted 14 July 2008 Corresponding Editor: William Cameron, Ottawa, Canada KEYWORDS Summary Deep neck infections; Objectives: The aims of this study were to review the clinical characteristics and management of Submandibular infection; submandibular space infections and to identify the predisposing factors of life-threatening Airway control; complications. Treatment; Design and methods: This was a retrospective study at a tertiary academic center. We retrieved Ludwig’s angina; and evaluated the records of all patients admitted to the University of Padua Otolaryngology Clinic Complications at Treviso Regional Hospital with the diagnosis of submandibular space infection for the period 1998—2006. The following variables were reviewed: demographic data, pathogenesis, clinical presentation, associated systemic diseases, bacteriology, imaging studies, medical and surgical treatment, and complications. A multivariate logistic regression analysis was undertaken using a forward stepwise technique. Results: Multivariate analysis identified four risk factors for complications. Anterior visceral space involvement (odds ratio (OR) 54.44; 95% confidence interval (CI) 5.80—511.22) and diabetes mellitus (OR 17.46; 95% CI 2.10—145.29) were the most important predictive factors in the model. Logistic regression analysis also confirmed other comorbidities (OR 11.66; 95% CI 1.35—100.10) and bilateral submandibular swelling (OR 10.67; 95% CI 2.73—41.75) as independent predictors for life- threatening complications.