Anatomical Variations of the Hand Extensors G.A
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

14-Anatomy of Forearm
FOREARM By : Prof.Saeed Abulmakarem. Dr. Sanaa Al-Sharawy OBJECTIVES §At the end of this lecture, the student should able to : §List the names of the Flexors Group of Forearm (superficial & deep muscles). §Identify the common flexor origin of flexor muscles and their innervation & movements. §Identify supination & poronation and list the muscles produced these 2 movements. §List the names of the Extensor Group of Forearm (superficial & deep muscles). §Identify the common extensor origin of extensor musles and their innervation & movements. n The forearm extends from elbow to wrist. n It posses two bones radius laterally & Ulna medially. n The two bones are connected together by the interosseous membrane. n This membrane allows movement of Pronation and Supination while the two bones are connected together. n Also it gives origin for the deep muscles. § The forearm is Fascial Compartments of the Forearm enclosed in a sheath of deep fascia, which is attached to the posterior border of the ulna . §This fascial sheath, together with the interosseous membrane & fibrous intermuscular septa, divides the forearm into compartments, each having its own muscles, nerves, and blood supply. These muscles: 8 FLEXOR GROUP § Act on the elbow & wrist joints and those of the fingers. § Form fleshy masses in the proximal part and become tendinous in the distal part of the forearm. •Arranged in three groups: I-Superficial: 4 Ø Pronator teres Ø Flexor carpi radialis Ø Palmaris longus III- Deep: 3 Ø Flexor carpi ulnaris Ø Flexor digitorum profundus II-Intermediate: 1 Ø Flexor pollicis longus Ø Ø Flexor digitorum superficialis Pronator quadratus n Superficial Flexors: n They arise - more or less- from the common flexor origin (front of medial epicondyle). -

Small Muscles of the Hand
By the name of Allah Small muscles of the hand Revision: The palmar aponeurosis is triangular in shape with apex and base. It is divided into 4 bands that radiate to the medial four fingers. Dupuytren’s Contracture: • A localized thickening and shortening of palmar aponeurosis that limits hand function (it is permanent) • Fibrosis pulls the ring finger then the little finger into partial flexion at the MCP joints, followed by flexion of their proximal interphalangeal joints • Usual treatment: Treated by surgical excision of fibrous bands followed by physiotherapy. Alternative treatment: Injection of the enzyme Collagenase into the contracted bands of the fibrous tissue. Keep in mind: • When the muscle Isn’t functioning: It is Relaxed. While it is in action: It is contracted. • Contraction DIFFERS from contracture. Contracture means permanent shortening. 18 th \Mar\2012 1 Small muscles of the hand: Arranged in five groups + 1 muscle, as the following: 1- Thenar muscles: (three in number) each moves the thumb according to its name: • Flexor pollicis brevis: assists the flexor pollicis longus in the flexion of MCP joint of the thumb. • Abductor pollicis brevis: abduction of the thumb. • Opponens pollicis: pulls the thumb medially and forward across the palm (as in counting fingers, shown in the figure below). All supplied by median nerve. 2- Hypothenar muscles: (three in number) each moves the little finger according to its name: • Flexor digiti minimi. • Abductor digit minimi. • Opponens digiti minimi. All supplied by deep branch of ulnar nerve. Only the thumb and little finger got opponens muscles, the Dr said it is because of the long distance between the two fingers ☺ 3- Adductor pollicis muscle: • It has got two heads: horizontal( transverse) and Oblique. -

Extensor Pollicis Longus Superficialis and Extensor Indicis Superficialis, Can They Be Considered As a New Anatomical Variation in the Long Extensors of Fingers?
Int. J. Curr. Res. Med. Sci. (2016). 2(12): 27-32 International Journal of Current Research in Medical Sciences ISSN: 2454-5716 www.ijcrims.com Volume 2, Issue 12 -2016 Case study DOI: http://dx.doi.org/10.22192/ijcrms.2016.02.12.005 Extensor pollicis longus superficialis and extensor indicis superficialis, can they be considered as a new anatomical variation in the long extensors of fingers? Ahmed Farid Al-Neklawy, M.D. Anatomy and Embryology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt E-mail: [email protected], Tel: 00201001850336 Running title: Two extra muscles for thumb and index fingers Abstract Background: Variations of anomalies of hand extensors have been described by many authors. These anomalies are often discovered during routine surgical procedures and cadaveric dissections. Being aware of such anomalies is important to the physician in order to avoid unintentional damage to healthy tendons during surgical procedures. In addition, accessory tendons have the potential to be used in the surgical repair or replacement of damaged tendons. We reported a cadaveric case with bilateral two additional superficial extensors to the thumb and index fingers with unique features. The names of extensor pollicis longus superficialis (EPL-S) and extensor indicis superficialis(EI-S) were proposed. Methods: A female cadaver was used in this study. Bilateral dissection of the forearm and wrist was done. Results: Two extra muscles were observed in the superficial group of the extensors of the forearm. They were situated between extensor carpi radialis brevis and extensor digitorum muscles. Both muscles originated from the common extensor origin. -

Section 1 Upper Limb Anatomy 1) with Regard to the Pectoral Girdle
Section 1 Upper Limb Anatomy 1) With regard to the pectoral girdle: a) contains three joints, the sternoclavicular, the acromioclavicular and the glenohumeral b) serratus anterior, the rhomboids and subclavius attach the scapula to the axial skeleton c) pectoralis major and deltoid are the only muscular attachments between the clavicle and the upper limb d) teres major provides attachment between the axial skeleton and the girdle 2) Choose the odd muscle out as regards insertion/origin: a) supraspinatus b) subscapularis c) biceps d) teres minor e) deltoid 3) Which muscle does not insert in or next to the intertubecular groove of the upper humerus? a) pectoralis major b) pectoralis minor c) latissimus dorsi d) teres major 4) Identify the incorrect pairing for testing muscles: a) latissimus dorsi – abduct to 60° and adduct against resistance b) trapezius – shrug shoulders against resistance c) rhomboids – place hands on hips and draw elbows back and scapulae together d) serratus anterior – push with arms outstretched against a wall 5) Identify the incorrect innervation: a) subclavius – own nerve from the brachial plexus b) serratus anterior – long thoracic nerve c) clavicular head of pectoralis major – medial pectoral nerve d) latissimus dorsi – dorsal scapular nerve e) trapezius – accessory nerve 6) Which muscle does not extend from the posterior surface of the scapula to the greater tubercle of the humerus? a) teres major b) infraspinatus c) supraspinatus d) teres minor 7) With regard to action, which muscle is the odd one out? a) teres -
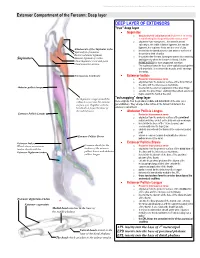
Extensor Compartment of the Forearm: Deep Layer
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. Extensor Compartment of the Forearm: Deep layer DEEP LAYER OF EXTENSORS "true" deep layer Supinator o deep branch of radial nerve which pierces it on its way to transforming into the posterior interosseous nerve o originates from everywhere... the lateral humeral epicondyle, the radial collateral ligament, the annular ligament, the supinator fossa and the crest of ulna Attachments of the Supinator to the o inserts into the lateral posterior and anterior surfaces of Epicondyle of humerus the proximal third of radius Radial collateral ligament o it supinates the forearm, turning the arm to face anteriorly Annular ligament of radius Supinator and superiorly when the forearm is flexed. It is the Ulnar Supinator crest and fossa PRIME MOVER for slow unopposed suination Ulnar posterior surface o The supinator forms the floor of the cubital fossa together with brachialis. It is a sheet-like muscle, and it envelops the radius. Interosseous membrane Extensor Indicis o Posterior interosseous nerve o originates from the posterior surface of the distal third of the ulna, and the interosseous membrane Abductor pollicis longus o inserts into the extensor expansion of the index finger o extends the index finger, enabling independent extension o helps extend the hand at the wrist "outcropping" deep layer the Supinator wraps around the radius to insert into the anterior these originate from the proximal, middle and distal thirds of the ulna (as a surface of it. -

Upper Limb : Muscles "Revision" Anatomy Team 434
Upper Limb : Muscles "Revision" Anatomy Team 434 Color Index: If you have any complaint or ▪ Important Points suggestion please don’t ▪ Helping notes hesitate to contact us on: [email protected] ▪ Explanation Muscles of shoulder region Muscle ORIGIN INSERTION ACTION NERVE Lateral 1/3 of clavicle + Deltoid tuberosity of Deltoid acromion and spine of Major abductor of the arm humerus scapula Axillary nerve Greater tuberosity of Teres minor Laterally rotates the arm humerus Lateral border of scapula Adducts at the shoulder and Teres major Bicipital groove of humerus Lower subscapular nerve medially rotates the arm Abducts the arm 0-15o, and Supraspinatus Supraspinous fossa Greater tuberosity of assists deltoid for 15-90o Suprascapular nerve humerus Infraspinatus Infraspinous fossa Laterally rotates the arm Lesser tuberosity of Upper and lower Subscapularis Subscapular fossa Medially rotates the arm humerus subscapular nerves All the pictures are taken from [ http://teachmeanatomy.info/ ] .. Muscles of pectoral region Muscle ORIGIN INSERTION ACTION NERVE -Sternum, -Adduct and medially rotate the Medial and Pectoralis -Upper 6 costal cartilages humerus Lateral lip of bicipital groove lateral pectoral major -Aponeurosis of external -The clavicular head also nerves oblique muscle performs flexion -Depression of shoulder Pectoralis 3rd, 4th, & 5th ribs close Medial pectoral Coracoid process -Draw the ribs upward & minor to their costal cartilages nerve outwards during deep inspiration Steadies or fixes the clavicle 1st rib at its costal Subclavian groove at the inferior Nerve to Subclavius during movement of the shoulder cartilage surface of middle 1/3 of clavicle subclavius joint -Draws the scapula forward -Rotates scapula outwards in Serratus Ventral aspect of the medial border Long thoracic Upper eight ribs raising the arm above 90 degree. -

* the Function of Extensor Digitorum
Forearm Arteries and nerves Revision: ☻The function of extensor digitorum : It extends the medial 4 fingers and the wrist. ☻The 4 tendons of the extensor digitorum flatten over the proximal phalanges of the medial 4 fingers to form extensor expansion (extensor hood) in some books. ☻The extensor expansion divides into 3 divisions: •One is central •Two are laterals. ☻Extensor expansion receives: • interosseous muscle on each side(palmar interossei and dorsal interossei) • Lumbrical(worm-like) muscle on the lateral side. ☻The function of extensor expansion when these small muscles attached to it : 1- flexion of matacarpophalangeal (MCP) joints. 2- extension of interphalangeal joints Main function : writing position Arteries: Brachial artery divides at opposite neck of radius into two branches: 1-ulnar artery (larger) 2- radial artery (smaller) ulnar ☻They both reach the wrist. artery Ulnar artery (larger): ☻It passes above flexor retinaculum and divides into 2 branches: 1-superfecial branch (larger) Radial 2- deep branch (smaller) artery ☻Both of them will go to the hand. From medial to lateral pisiform (insertion of flexor carpi ulnaris) >>> ulnar nerve>>> ulnar artery Radial artery (smaller): ☻It is located on the floor of snuffbox. ☻In the snuffbox it divides into : 1-small superficial branch. 2- large deep branch. Palmar arches: Palm is supplied by a connection between vessels called ( anastomosis ) 1- superficial palmar arch. 2- deep palmer arch. Superficial palmer arch: ☻It is contributed from: 1-(mainly) superficial branch of ulnar artery (direct continuation of it). 2- smaller superficial branch of radial artery. ☻It is located at the distal level of the hyper extended thumb. -

Unusual Variation of the Extensor Indicis Muscle Tendon
eISSN 1308-4038 International Journal of Anatomical Variations (2009) 2: 17–19 Case Report Unusual variation of the extensor indicis muscle tendon Published online January 31st, 2009 © http://www.ijav.org Satya Prasad VENUGOPAL ABSTRACT Sree Bhanu MALLULA There are numerous reports regarding the variations of the extensor muscles. The present report is on the unusual variation of the extensor indicis muscle. The extensor indicis presented two tendons, one of which is inserted into the ulnar aspect of the dorsal digital expansion of the index finger. While the other tendon –especially in Department of Anatomy, M.N.R. Medical College, Sangareddy, Medak District, Andhra the left upper limb– was inserted into the dorsal part of the capsule of the metacarpophalangeal joint of the Pradesh, INDIA. middle finger and also few tendinous fibers were merging with the dorsal expansion of the middle finger. The same variation was found in the right upper limb, but the insertion was to the dorsal digital expansion of the index and middle fingers and no attachment to the capsule was noticed. © IJAV. 2009; 2: 17–19. Dr. Satya Prasad VENUGOPAL Department Of Anatomy M.N.R. Medical College Sangareddy, Medak District Andhra Pradesh, INDIA. +91 8455 277055 +91 8455 277688 [email protected] Received October 30th, 2008; accepted January 19th, 2009 Key words [extensor indicis tendon] [middle finger] [capsule of metacarpophalangeal joint] [extensor expansion] Introduction The extensor indicis (EI) muscle is one of the known extensor for its variations. It normally arises from the EI posterior surface of the ulna and the adjoining interosseous membrane, and is inserted into the ulnar aspect of the extensor expansion of the index finger. -

Practical Muscles and Vessels of Upper Limb
Practical Muscles and vessels of upper limb OBJECTIVES - Identify the different group of muscles of upper limb, (pectoral, scapular, flexors and extensors of arm and forearm, muscles of the hand). - List the name of each muscle group. - Briefly mention the attachment (origin & insertion) of these muscular groups, the action and nerve supply of these groups of muscles. - Describe the course, and distribution of the nerves of upper limb (radial, ulnar, median, musculocutaneous and axillary nerves). - Describe the course and branches of the main arteries of the upper limb (axillary, brachial, radial and ulnar arteries). - Describe the course, and tributaries of the superficial and deep veins of the upper limb (cephalic, basilic, brachial and axillary vein). Muscles of pectoral region: - Pectoralis major - Pectoralis minor - Subclavius - Serratus anterior Muscles of scapular region: - Deltoid - Supraspinatus - Infraspinatus - Teres minor - Teres major - Subscapularis Muscles of arm: Anterior compartment (flexors): - Biceps brachii - Coracobrachialis - Brachialis Posterior compartment (extensors): - Triceps Muscles of forearm: Anterior compartment (flexors): - Pronator teres - Flexor carpi radialis - Palmaris longus - Flexor carpi ulnaris - Flexor digitorum superficialis - Flexor digitorum profundus - Flexor pollicis longus - Pronator quadratus Posterior compartment (extensors): - Brachioradialis - Extensor carpi radialis longus - Extensor carpi radialis brevis - Extensor digitorum - Extensor digiti minimi - Extensor carpi ulnaris - Anconeus -

Dissection Schedule
DISSECTION SCHEDULE Session I - Pectoral Region Surface anatomy Self study ØØØ Clavicle and its ends ØØØ Sternal angle, xiphoid process, jugular ••• Location, extent, relations, notch blood supply, lymphatic ØØØ Ribs and cartilages drainage, applied anatomy of breast ØØØ Nipple and areola ØØØ Axilla and axillary folds ••• Axillary lymph nodes Dissection ••• ØØØ Cutaneous nerves & vessels Attachments (proximal & distal), nerve ØØØ Deep fascia, clavipectoral supply and actions of fascia pectoralis major ØØØ Breast (in female body) ØØØ Pectoralis major muscle ••• Clavicle - attachments, movements & special ØØØ Cephalic vein features Session II - Axilla (Vessels) Dissection Self study Muscles ••• Boundaries and contents of axilla ØØØ Pectoralis minor ØØØ Coracobrachialis, short head of biceps ••• Origin, course, termination & branches of Nerves axillary artery ØØØ Lateral and medial pectoral nerves ØØØ Median nerve ••• Attachments, nerve supply & actions of ØØØ ØØ Ulnar nerve pectoralis minor ØØØ Musculocutaneous nerve ØØØ Medial cutaneous nerve of arm and forearm; intercostobrachial nerve Vessels ØØØ Thoracoacromial artery ØØØ Axillary artery and vein Other structures ØØØ Axillary pad of fat ØØØ Axillary lymph nodes Session III - Axilla (Brachial Plexus) Dissection Self study Nerves ••• Formation, parts, distribution of brachial ØØØ Cords of brachial plexus plexus ØØØ Median nerve ØØØ Musculocutaneous nerve ••• ØØØ Ulnar nerve Sternoclavicular joint - Type, description, ØØØ Radial nerve movements ØØØ Axillary nerve ØØØ Upper and lower subscapular -
The Upper Limb Lecture 1.Pdf
The upper limb Muscles That Move the Pectoral Girdle Originate on the axial skeleton and insert on the clavicle and scapula. Stabilize the scapula and move it to increase the arm’s angle of movements. Some of the superficial muscles of the thorax are grouped together according to the scapular movement they direct. elevation, depression, protraction, or retraction The muscles of back Superficial group Trapezius Latissimus dorsi Levator scapulae Rhomboideus Deep group Erector spinae Splenius Thoracolumbar fascia The muscles of thorax Extrinsic muscles Pectoralis major Pectoralis minor Serratus anterior Intrinsic muscles Intercostales externi Intercostales interni Intercostales intimi The Muscles of Upper Limb Muscles of shoulder Deltoid supraspinatus Infraspinatus Teres minor Teres major subscapularis Major muscles of upper limb Deltoid Origin: lateral third of clavicle, acromion, and spine of scapula Insertion: deltoid tuberosity of humerus Action: abducts,flexes and medically rotates, extends, and laterally rotates arm Teres major Origin: dorsal surface of inferior angle of scapula Insertion: crest of lesser tubercle of humerus Action: medially rotates and adducts arm Foramen axillare laterale et mediale Arm Muscles That Move the Shoulder/Elbow Joint (Flexor) compartment Posterior (extensor) compartment Anterior compartment primarily contains shoulder/elbow flexors Posterior compartment contains elbow extensors the principal flexors biceps brachii, brachialis, and brachioradialis muscles that extend -

Upper Extremity Muscle Table
Robert Frysztak, PhD. Structure of the Human Body Loyola University Chicago Stritch School of Medicine UPPER EXTREMITY MUSCLE TABLE PROXIMAL ATTACHMENT DISTAL ATTACHMENT MUSCLE INNERVATION MAIN ACTIONS BLOOD SUPPLY MUSCLE GROUP (ORIGIN) (INSERTION) Flexor carpi radialis Medial epicondyle of humerus Base of 2nd metacarpal Median nerve Flexes and abducts hand at wrist Radial artery Anterior forearm Humeral head: medial epicondyle of Pisiform bone, hook of hamate, base Flexor carpi ulnaris humerus Ulnar head: olecranon and Ulnar nerve Flexes and adducts hand at wrist Posterior ulnar recurrent artery Anterior forearm of 5th metacarpal posterior border of ulna Medial and anterior surface of Flexes distal phalanges of medial four Palmar base of distal phalanges of Medial part: ulnar nerve Lateral Anterior interosseous artery, Flexor digitorum profundus proximal 3/4 of ulna and digits, assists with flexion of hand at Anterior forearm medial four digits part: median nerve muscular branches of ulnar artery interosseous membrane wrist Humero‐ulnar head: medial epicondyle of humerus and coronoid Flexes middle and proximal Bodies of middle phalanges of medial Flexor digitorum superficialis process of ulna Median nerve phalanges of medial four digits, flexes Ulnar and radial arteries Anterior forearm four digits Radial head: superior half of anterior hand at wrist radius Anterior surface of radius and Palmar base of distal phalanx of Flexor pollicis longus Median nerve (anterior interosseous) Flexes phalanges of thumb Anterior interosseous artery