Flexor and Extensor Forearm
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

14-Anatomy of Forearm
FOREARM By : Prof.Saeed Abulmakarem. Dr. Sanaa Al-Sharawy OBJECTIVES §At the end of this lecture, the student should able to : §List the names of the Flexors Group of Forearm (superficial & deep muscles). §Identify the common flexor origin of flexor muscles and their innervation & movements. §Identify supination & poronation and list the muscles produced these 2 movements. §List the names of the Extensor Group of Forearm (superficial & deep muscles). §Identify the common extensor origin of extensor musles and their innervation & movements. n The forearm extends from elbow to wrist. n It posses two bones radius laterally & Ulna medially. n The two bones are connected together by the interosseous membrane. n This membrane allows movement of Pronation and Supination while the two bones are connected together. n Also it gives origin for the deep muscles. § The forearm is Fascial Compartments of the Forearm enclosed in a sheath of deep fascia, which is attached to the posterior border of the ulna . §This fascial sheath, together with the interosseous membrane & fibrous intermuscular septa, divides the forearm into compartments, each having its own muscles, nerves, and blood supply. These muscles: 8 FLEXOR GROUP § Act on the elbow & wrist joints and those of the fingers. § Form fleshy masses in the proximal part and become tendinous in the distal part of the forearm. •Arranged in three groups: I-Superficial: 4 Ø Pronator teres Ø Flexor carpi radialis Ø Palmaris longus III- Deep: 3 Ø Flexor carpi ulnaris Ø Flexor digitorum profundus II-Intermediate: 1 Ø Flexor pollicis longus Ø Ø Flexor digitorum superficialis Pronator quadratus n Superficial Flexors: n They arise - more or less- from the common flexor origin (front of medial epicondyle). -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Parts of the Body 1) Head – Caput, Capitus 2) Skull- Cranium Cephalic- Toward the Skull Caudal- Toward the Tail Rostral- Toward the Nose 3) Collum (Pl
BIO 3330 Advanced Human Cadaver Anatomy Instructor: Dr. Jeff Simpson Department of Biology Metropolitan State College of Denver 1 PARTS OF THE BODY 1) HEAD – CAPUT, CAPITUS 2) SKULL- CRANIUM CEPHALIC- TOWARD THE SKULL CAUDAL- TOWARD THE TAIL ROSTRAL- TOWARD THE NOSE 3) COLLUM (PL. COLLI), CERVIX 4) TRUNK- THORAX, CHEST 5) ABDOMEN- AREA BETWEEN THE DIAPHRAGM AND THE HIP BONES 6) PELVIS- AREA BETWEEN OS COXAS EXTREMITIES -UPPER 1) SHOULDER GIRDLE - SCAPULA, CLAVICLE 2) BRACHIUM - ARM 3) ANTEBRACHIUM -FOREARM 4) CUBITAL FOSSA 6) METACARPALS 7) PHALANGES 2 Lower Extremities Pelvis Os Coxae (2) Inominant Bones Sacrum Coccyx Terms of Position and Direction Anatomical Position Body Erect, head, eyes and toes facing forward. Limbs at side, palms facing forward Anterior-ventral Posterior-dorsal Superficial Deep Internal/external Vertical & horizontal- refer to the body in the standing position Lateral/ medial Superior/inferior Ipsilateral Contralateral Planes of the Body Median-cuts the body into left and right halves Sagittal- parallel to median Frontal (Coronal)- divides the body into front and back halves 3 Horizontal(transverse)- cuts the body into upper and lower portions Positions of the Body Proximal Distal Limbs Radial Ulnar Tibial Fibular Foot Dorsum Plantar Hallicus HAND Dorsum- back of hand Palmar (volar)- palm side Pollicus Index finger Middle finger Ring finger Pinky finger TERMS OF MOVEMENT 1) FLEXION: DECREASE ANGLE BETWEEN TWO BONES OF A JOINT 2) EXTENSION: INCREASE ANGLE BETWEEN TWO BONES OF A JOINT 3) ADDUCTION: TOWARDS MIDLINE -

Small Muscles of the Hand
By the name of Allah Small muscles of the hand Revision: The palmar aponeurosis is triangular in shape with apex and base. It is divided into 4 bands that radiate to the medial four fingers. Dupuytren’s Contracture: • A localized thickening and shortening of palmar aponeurosis that limits hand function (it is permanent) • Fibrosis pulls the ring finger then the little finger into partial flexion at the MCP joints, followed by flexion of their proximal interphalangeal joints • Usual treatment: Treated by surgical excision of fibrous bands followed by physiotherapy. Alternative treatment: Injection of the enzyme Collagenase into the contracted bands of the fibrous tissue. Keep in mind: • When the muscle Isn’t functioning: It is Relaxed. While it is in action: It is contracted. • Contraction DIFFERS from contracture. Contracture means permanent shortening. 18 th \Mar\2012 1 Small muscles of the hand: Arranged in five groups + 1 muscle, as the following: 1- Thenar muscles: (three in number) each moves the thumb according to its name: • Flexor pollicis brevis: assists the flexor pollicis longus in the flexion of MCP joint of the thumb. • Abductor pollicis brevis: abduction of the thumb. • Opponens pollicis: pulls the thumb medially and forward across the palm (as in counting fingers, shown in the figure below). All supplied by median nerve. 2- Hypothenar muscles: (three in number) each moves the little finger according to its name: • Flexor digiti minimi. • Abductor digit minimi. • Opponens digiti minimi. All supplied by deep branch of ulnar nerve. Only the thumb and little finger got opponens muscles, the Dr said it is because of the long distance between the two fingers ☺ 3- Adductor pollicis muscle: • It has got two heads: horizontal( transverse) and Oblique. -

Extensor Pollicis Longus Superficialis and Extensor Indicis Superficialis, Can They Be Considered As a New Anatomical Variation in the Long Extensors of Fingers?
Int. J. Curr. Res. Med. Sci. (2016). 2(12): 27-32 International Journal of Current Research in Medical Sciences ISSN: 2454-5716 www.ijcrims.com Volume 2, Issue 12 -2016 Case study DOI: http://dx.doi.org/10.22192/ijcrms.2016.02.12.005 Extensor pollicis longus superficialis and extensor indicis superficialis, can they be considered as a new anatomical variation in the long extensors of fingers? Ahmed Farid Al-Neklawy, M.D. Anatomy and Embryology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt E-mail: [email protected], Tel: 00201001850336 Running title: Two extra muscles for thumb and index fingers Abstract Background: Variations of anomalies of hand extensors have been described by many authors. These anomalies are often discovered during routine surgical procedures and cadaveric dissections. Being aware of such anomalies is important to the physician in order to avoid unintentional damage to healthy tendons during surgical procedures. In addition, accessory tendons have the potential to be used in the surgical repair or replacement of damaged tendons. We reported a cadaveric case with bilateral two additional superficial extensors to the thumb and index fingers with unique features. The names of extensor pollicis longus superficialis (EPL-S) and extensor indicis superficialis(EI-S) were proposed. Methods: A female cadaver was used in this study. Bilateral dissection of the forearm and wrist was done. Results: Two extra muscles were observed in the superficial group of the extensors of the forearm. They were situated between extensor carpi radialis brevis and extensor digitorum muscles. Both muscles originated from the common extensor origin. -

Section 1 Upper Limb Anatomy 1) with Regard to the Pectoral Girdle
Section 1 Upper Limb Anatomy 1) With regard to the pectoral girdle: a) contains three joints, the sternoclavicular, the acromioclavicular and the glenohumeral b) serratus anterior, the rhomboids and subclavius attach the scapula to the axial skeleton c) pectoralis major and deltoid are the only muscular attachments between the clavicle and the upper limb d) teres major provides attachment between the axial skeleton and the girdle 2) Choose the odd muscle out as regards insertion/origin: a) supraspinatus b) subscapularis c) biceps d) teres minor e) deltoid 3) Which muscle does not insert in or next to the intertubecular groove of the upper humerus? a) pectoralis major b) pectoralis minor c) latissimus dorsi d) teres major 4) Identify the incorrect pairing for testing muscles: a) latissimus dorsi – abduct to 60° and adduct against resistance b) trapezius – shrug shoulders against resistance c) rhomboids – place hands on hips and draw elbows back and scapulae together d) serratus anterior – push with arms outstretched against a wall 5) Identify the incorrect innervation: a) subclavius – own nerve from the brachial plexus b) serratus anterior – long thoracic nerve c) clavicular head of pectoralis major – medial pectoral nerve d) latissimus dorsi – dorsal scapular nerve e) trapezius – accessory nerve 6) Which muscle does not extend from the posterior surface of the scapula to the greater tubercle of the humerus? a) teres major b) infraspinatus c) supraspinatus d) teres minor 7) With regard to action, which muscle is the odd one out? a) teres -
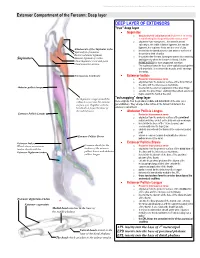
Extensor Compartment of the Forearm: Deep Layer
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. Extensor Compartment of the Forearm: Deep layer DEEP LAYER OF EXTENSORS "true" deep layer Supinator o deep branch of radial nerve which pierces it on its way to transforming into the posterior interosseous nerve o originates from everywhere... the lateral humeral epicondyle, the radial collateral ligament, the annular ligament, the supinator fossa and the crest of ulna Attachments of the Supinator to the o inserts into the lateral posterior and anterior surfaces of Epicondyle of humerus the proximal third of radius Radial collateral ligament o it supinates the forearm, turning the arm to face anteriorly Annular ligament of radius Supinator and superiorly when the forearm is flexed. It is the Ulnar Supinator crest and fossa PRIME MOVER for slow unopposed suination Ulnar posterior surface o The supinator forms the floor of the cubital fossa together with brachialis. It is a sheet-like muscle, and it envelops the radius. Interosseous membrane Extensor Indicis o Posterior interosseous nerve o originates from the posterior surface of the distal third of the ulna, and the interosseous membrane Abductor pollicis longus o inserts into the extensor expansion of the index finger o extends the index finger, enabling independent extension o helps extend the hand at the wrist "outcropping" deep layer the Supinator wraps around the radius to insert into the anterior these originate from the proximal, middle and distal thirds of the ulna (as a surface of it. -

Skeletal System -Appendicular System
Skeletal System -Appendicular System Chapter 8 Part B Skeleton - Divisions Total number of bones: 206 Divided into two major subdivisions: Axial system….blue Appendicular system….tan Axial system: Composed of bones that form the axis of the body. 80 bones. Appendicular system: Composed of bones that form The limbs. The bones that attach the limbs to the axial. 126 bones. Practice…Practice…Practice…Practice…Practice!! Appendicular Skeleton Appendicular system: Pectoral girdle 4 bones Upper extremity 60 bones Pelvic girdle 2 bones Lower extremity 60 bones 126 bones Appendicular Skeleton Appendicular system: Pectoral girdle 4 bones Upper extremity 60 bones Pelvic girdle 2 bones Lower extremity 60 bones 126 bones Upper Extremity/Limb Upper limbs/extremities are composed of 60 bones…30 bones in each limb: Upperarm – Humerus Forearm – Radius and Ulna Wrist – Carpals Hand – Metacarpals in palm – Phalanges in fingers and thumb Upper Extremity/Limb - Humerus Body/Shaft Humerus: long bone. Has 3 regions: Proximal end articulates with glenoid cavity of scapula. Distal end articulates with radius and ulna. Body/Shaft: diaphysis between proximal and distal ends. Has rough surface – deltoid tuberosity…for deltoid muscle attachment. Upper Extremity/Limb - Humerus Body/Shaft Humerus - Proximal end: Head: rounded projection fits into glenoid cavity of scapula. Greater and lesser tubercles: projections next to the head for muscle attachment. Intertubercular sulcus: groove between the tubercles accommodates tendon of an arm muscle. Upper Extremity/Limb - Humerus Body/Shaft Humerus - Distal end: Anterior surface: Capitulum: small, rounded knob articulates with proximal end of radius of forearm. Trochlea: spool-shaped structure articulates with proximal end of ulna of forearm. -

Arm and Cubital Fossa
Two Minute History M1 - Anatomy Dissection: • 300 B.C Arm and Cubital Alexandrian Egypt: King Ptolemy I, its ok Fossa to dissect cadavers of executed, mummies etc… •Herophilus “Father of Anatomy” accused by a rival of DG Simpson, Ph.D. dissecting 600 criminals…..live criminals VCU Department of Anatomy •1300 AD Europe Pope Boniface VIII edict to stop dissection to reduce the flow of bodies “parted out and boiled” from the crusades. Unclear if this is broad ban or very narrow. 1 2 Dissection: Dissection: •1540 parliament passes “The United Company of Barbers and •1700’s with the expansion of medical Surgeons, dissect 4-6 executed schools cadavers are used as tuition criminals/yr (not enough even then) •Competition is very high and medical •1600’s Britain. The executed are schools actively advertise that training includes dissections etc.. dissected in public as punishment • 1628 William Harvey •1828 London had 10 full time (cardiovascular fame). Autopsy & 200 part time body snatchers (“seasonal work” at 312 bodies/yr) of live and dead…. Medicine expands and shortages develop •Inventions to foil grave robbers Harvey dissects father and sister •1828 Robert Knox….and the rest • 1740’s Lots of private medical is amazing history. schools competing for students, William Hogarth The Reward of Cruelty 3 4 market forces develop 1750-1751 Dissection: •Burke was hanged: 25,000 watched. Hare was granted immunity as crowd called “Burke Hare” •1828, knock on the •Burke dissected: 30,000 came to see the open lab door, Knox’s assistant purchases a cadaver -
Bones of Upper Limb
BONES OF THE UPPER LIMB Dr. Jamila El-Medany OBJECTIVES At the end of the lecture, students should be able to: List the different bones of the UL. List the characteristic features of each bone. Differentiate between the bones of the right and left sides. List the articulations between the different bones. The Bones of UL are: Pectoral Girdle. Arm : Humerus. Forearm : Radius & Ulna. Wrist : Carpal bones Hand: Metacarpals & Phalanges Pectoral Girdle Formed of Two Bones: Clavicle (anteriorly) and Scapula (posteriorly). It is very light and allows the upper limb to have exceptionally free movement. Clavicle It is a doubly curved long bone lying horizontally across the root of the neck It is subcutaneous throughout its length. Functions: 1. It serves as a rigid support from which the scapula and free upper limb are suspended & keep them away from the trunk so that the arm has maximum freedom of movement. 2. Transmits forces from the upper limb to the axial skeleton. 3. Provides attachment for muscles. 4. It forms a boundary of the Cervicoaxillary canal for protection of the neurovascular bundle of the UL. Clavicle It is a long bone with no medullary cavity. It has the appearance of an elongated letter Capital (S) lying on one side. It has Two Ends: Medial (Sternal) : enlarged & triangular. Lateral (Acromial) : flattened. Body (shaft): Its medial 2/3 is convex forward. Its lateral 1/3 is concave forward. Surfaces: Superior : smooth as it lies just deep to the skin. Inferior : rough because strong ligaments bind it to the 1st rib. Articulations of Clavicle Medially with the manubrium at the Sternoclavicular joint . -

BO6 106 Rzepkowki
106: Shoulder & Elbow Joint Replacements – New Advancements in Rehab Terry Rzepkowski, DPT, MS, BS To comply with professional boards/associations standards: • I declare that I (or my family) do not have a financial relationship in any amount, occurring in the last 12 months with a commercial interest whose products or services are discussed in my presentation. Additionally, all planners involved do not have any financial relationship. •Requirements for successful completion are attendance for the full session along with a completed session evaluation. •PESI and all current accreditation statuses does not imply endorsement of any commercial products displayed in conjunction with this activity. 106: Shoulder & Elbow Joint Replacements – New Advancements in Rehab Terry Rzepkowski, DPT, MS, BS Financial: Terry Rzepkowski is an Assistant Professor for Nova Southeastern University Tampa; and an Assistant Professor for South University Tampa. He receives a speaking honorarium from PESI, Inc. Non‐financial: Terry Rzepkowski is a member of the American Physical Therapy Association (APTA). UE joint replacements and post‐op management Dr. Terry Rzepkowski, DPT Associate Professor [email protected] 1 About the instructor Dr. Terry L Rzepkowski, DPT, MS, BS Dr. Terry L Rzepkowski, DPT, MS, BS, is a Doctor of Physical Therapy with specialization in Orthopedic Physical Therapy. Throughout his 38‐year career, he has specialized in Orthopedics, specifically: Musculoskeletal out‐patient rehab as an independent private practitioner, Total Joint Replacement Surgery, Sports Medicine, and Orthopedic Homecare. This extensive background allows him to relate his knowledge of the complex rehab patient from prevention strategies including rehabilitative exercises, lifestyle and activity modifications through all phases of post‐op rehabilitation. -

Upper Limb : Muscles "Revision" Anatomy Team 434
Upper Limb : Muscles "Revision" Anatomy Team 434 Color Index: If you have any complaint or ▪ Important Points suggestion please don’t ▪ Helping notes hesitate to contact us on: [email protected] ▪ Explanation Muscles of shoulder region Muscle ORIGIN INSERTION ACTION NERVE Lateral 1/3 of clavicle + Deltoid tuberosity of Deltoid acromion and spine of Major abductor of the arm humerus scapula Axillary nerve Greater tuberosity of Teres minor Laterally rotates the arm humerus Lateral border of scapula Adducts at the shoulder and Teres major Bicipital groove of humerus Lower subscapular nerve medially rotates the arm Abducts the arm 0-15o, and Supraspinatus Supraspinous fossa Greater tuberosity of assists deltoid for 15-90o Suprascapular nerve humerus Infraspinatus Infraspinous fossa Laterally rotates the arm Lesser tuberosity of Upper and lower Subscapularis Subscapular fossa Medially rotates the arm humerus subscapular nerves All the pictures are taken from [ http://teachmeanatomy.info/ ] .. Muscles of pectoral region Muscle ORIGIN INSERTION ACTION NERVE -Sternum, -Adduct and medially rotate the Medial and Pectoralis -Upper 6 costal cartilages humerus Lateral lip of bicipital groove lateral pectoral major -Aponeurosis of external -The clavicular head also nerves oblique muscle performs flexion -Depression of shoulder Pectoralis 3rd, 4th, & 5th ribs close Medial pectoral Coracoid process -Draw the ribs upward & minor to their costal cartilages nerve outwards during deep inspiration Steadies or fixes the clavicle 1st rib at its costal Subclavian groove at the inferior Nerve to Subclavius during movement of the shoulder cartilage surface of middle 1/3 of clavicle subclavius joint -Draws the scapula forward -Rotates scapula outwards in Serratus Ventral aspect of the medial border Long thoracic Upper eight ribs raising the arm above 90 degree.