Dissection Schedule
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Study on the Absence of Palmaris Longus in a Multi-Racial Population
108472 NV-OA7 pg26-28.qxd 11/05/2007 05:02 PM Page 26 (Black plate) Malaysian Orthopaedic Journal 2007 Vol 1 No 1 SA Roohi, etal A Study on the Absence of Palmaris Longus in a Multi- racial Population SA Roohi, MS (Ortho) (UKM), L Choon-Sian, MD (UKM), A Shalimar, MS (Ortho) (UKM), GH Tan, MS (Ortho) (UKM), AS Naicker, M Med Rehab (UM) Hospital Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia ABSTRACT Most standard textbooks of hand surgery quote the prevalence of absence of palmaris longus at around 15%3-5. Palmaris longus is a dispensable muscle with a long tendon However, this figure varies considerably in different ethnic which is very useful in reconstructive surgery. It is absent groups. A study by Thompson et al6 on 300 Caucasian 2.8 to 24% of the population depending on the race/ethnicity subjects found that palmaris longus was absent unilaterally in studied. Four hundred and fifty healthy subjects (equally 16%, and bilaterally in 9% of the study sample for an overall distributed among Malaysia’s 3 major ethnic groups) were prevalence of absence of 24%. Similarly, George7 noted on clinically examined for the presence or absence of palmaris 276 cadavers of European descent that its absence was 13% longus. This tendon was found to be absent unilaterally in unilaterally, 8.7% bilaterally for an overall absence of 15.2%. 6.4% of study subjects, and bilaterally in 2.9% of study Another cadaveric study by Vanderhooft8 in Seattle, USA participants. Malays have a high prevalence of palmaris reported its overall absence to be 12%. -

14-Anatomy of Forearm
FOREARM By : Prof.Saeed Abulmakarem. Dr. Sanaa Al-Sharawy OBJECTIVES §At the end of this lecture, the student should able to : §List the names of the Flexors Group of Forearm (superficial & deep muscles). §Identify the common flexor origin of flexor muscles and their innervation & movements. §Identify supination & poronation and list the muscles produced these 2 movements. §List the names of the Extensor Group of Forearm (superficial & deep muscles). §Identify the common extensor origin of extensor musles and their innervation & movements. n The forearm extends from elbow to wrist. n It posses two bones radius laterally & Ulna medially. n The two bones are connected together by the interosseous membrane. n This membrane allows movement of Pronation and Supination while the two bones are connected together. n Also it gives origin for the deep muscles. § The forearm is Fascial Compartments of the Forearm enclosed in a sheath of deep fascia, which is attached to the posterior border of the ulna . §This fascial sheath, together with the interosseous membrane & fibrous intermuscular septa, divides the forearm into compartments, each having its own muscles, nerves, and blood supply. These muscles: 8 FLEXOR GROUP § Act on the elbow & wrist joints and those of the fingers. § Form fleshy masses in the proximal part and become tendinous in the distal part of the forearm. •Arranged in three groups: I-Superficial: 4 Ø Pronator teres Ø Flexor carpi radialis Ø Palmaris longus III- Deep: 3 Ø Flexor carpi ulnaris Ø Flexor digitorum profundus II-Intermediate: 1 Ø Flexor pollicis longus Ø Ø Flexor digitorum superficialis Pronator quadratus n Superficial Flexors: n They arise - more or less- from the common flexor origin (front of medial epicondyle). -

Ultrasonograpic Assessment of Relationship Between the Palmaris Longus Tendon and the Flexor Retinacular Ligament and the Palmar Aponeurosis of the Hand
Original Article Ultrasonograpic Assessment of Relationship Between the Palmaris Longus Tendon and the Flexor Retinacular Ligament and the Palmar Aponeurosis of the Hand Kadir Ertem1, Ahmet Sığırcı2, Salih Karaca1, Aykut Sığırcı3, Yunus Karakoç4, Saim Yoloğlu5 İnonu University, Faculty of Medicine, ABSTRACT Departments of Orthopedics and Trauma- tology1, Radioloy2, Physiology4 and Biosta- Aim: This study aimed to evaluate the presence of the Palmaris Longus tistics5, Malatya, Turkey Tendon (PLT) and the relationship between the Flexor Retinacular Ligament (FRL) and the Palmar Aponeurosis (PA) of the hand. 319 Mayıs University, Faculty of Medicine, Departments of Orthopaedics and Trauma- Method: 62 voluntary subjects (31 female, 31 male students and per- tology, Samsun, Turkey sonnel from the Inonu University, at the average age 28.38 ± 6.86 years ranging from 19 to 48 years) took part in this study using ultrasound. Eur J Gen Med 2010;7(2):161-166 Received: 16.05.2009 Result: Significant differences were found in the PA p-m-d diameters of subjects between with and without PLT bilaterally, on the right Accepted: 06.07.2009 and the left hand (p<0.05), whereas there was no meaningful differ- ence considering FRL diameters (p>0.05). Furthermore, this ultraso- nographic assessment revealed the continuity of collagen bunches of the PL tendon up to FRL, but not PA. Conclusion: Although not demonstrated by ultrasonography here, the increased thickness of the PA in subjects with a PLT supports the find- ings in the literature in which the structural -

M1 – Muscled Arm
M1 – Muscled Arm See diagram on next page 1. tendinous junction 38. brachial artery 2. dorsal interosseous muscles of hand 39. humerus 3. radial nerve 40. lateral epicondyle of humerus 4. radial artery 41. tendon of flexor carpi radialis muscle 5. extensor retinaculum 42. median nerve 6. abductor pollicis brevis muscle 43. flexor retinaculum 7. extensor carpi radialis brevis muscle 44. tendon of palmaris longus muscle 8. extensor carpi radialis longus muscle 45. common palmar digital nerves of 9. brachioradialis muscle median nerve 10. brachialis muscle 46. flexor pollicis brevis muscle 11. deltoid muscle 47. adductor pollicis muscle 12. supraspinatus muscle 48. lumbrical muscles of hand 13. scapular spine 49. tendon of flexor digitorium 14. trapezius muscle superficialis muscle 15. infraspinatus muscle 50. superficial transverse metacarpal 16. latissimus dorsi muscle ligament 17. teres major muscle 51. common palmar digital arteries 18. teres minor muscle 52. digital synovial sheath 19. triangular space 53. tendon of flexor digitorum profundus 20. long head of triceps brachii muscle muscle 21. lateral head of triceps brachii muscle 54. annular part of fibrous tendon 22. tendon of triceps brachii muscle sheaths 23. ulnar nerve 55. proper palmar digital nerves of ulnar 24. anconeus muscle nerve 25. medial epicondyle of humerus 56. cruciform part of fibrous tendon 26. olecranon process of ulna sheaths 27. flexor carpi ulnaris muscle 57. superficial palmar arch 28. extensor digitorum muscle of hand 58. abductor digiti minimi muscle of hand 29. extensor carpi ulnaris muscle 59. opponens digiti minimi muscle of 30. tendon of extensor digitorium muscle hand of hand 60. superficial branch of ulnar nerve 31. -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Anatomy, Shoulder and Upper Limb, Arm Quadrangular Space
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Anatomy, Shoulder and Upper Limb, Arm Quadrangular Space Authors Irfan A. Khan1; Matthew Varacallo2. Affiliations 1 Florida International University 2 Department of Orthopaedic Surgery, University of Kentucky School of Medicine Last Update: December 21, 2018. Introduction The quadrangular (or quadrilateral) space (QS) is named based on the shape of its anatomic boundaries. Located along the posterolateral shoulder, the QS serves as a passageway for the axillary nerve and posterior humeral circumflex artery (PHCA). Quadrangular (or quadrilateral) space syndrome (QSS) can occur secondary to various compressive pathologies. Although the incidence of such pathologies is rare, QSS has a known predilection for subgroups of athletic populations and can often suffer misdiagnosis or are clinically under-appreciated. Thus, clinicians should maintain a heightened clinical suspicion for QSS in patients aged 20-40 years of age presenting with a history of current contact or overhead athletic performance (e.g., baseball pitchers, swimmers, etc.), [1][2] or overhead laborers secondary to repetitive stress mechanics on the shoulder.[3] Structure and Function The QS has four anatomic borders; the teres minor superiorly, the inferior border is the teres major muscle, the medial boundary is the long head of the triceps brachii muscle, and the humeral surgical neck forms the lateral bound. The QS functions as a passageway for the axillary nerve, and the posterior humeral circumflex artery (PHCA).[3] The latter provides the primary (two-thirds) of the blood supply to the humeral head.[4] Blood Supply and Lymphatics The posterior humeral circumflex artery (PHCA) within the quadrangular space originates from the axillary artery, and within the QS, the PHCA divides into anterior and posterior branches. -

Anatomy and Physiology II
Anatomy and Physiology II Review Bones of the Upper Extremities Muscles of the Upper Extremities Anatomy and Physiology II Review Bones of the Upper Extremities Questions From Shoulder Girdle Lecture • Can you name the following structures? A – F • Acromion F – B B • Spine of the Scapula G – C • Medial (Vertebral) Border H – E C • Lateral (Axillary) Border – A • Superior Angle E I – D • Inferior Angle – G • Head of the Humerus D – H • Greater Tubercle of Humerus – I • Deltoid Tuberosity Questions From Shoulder Girdle Lecture • Would you be able to find the many of the same landmarks on this view (angles, borders, etc)? A • Can you name the following? – D • Coracoid process of scapula C – C D B • Lesser Tubercle – A • Greater Tubercle – B • Bicipital Groove (Intertubercular groove) Questions From Upper Extremities Lecture • Can you name the following structures? – B • Lateral epicondyle – A • Medial epicondyle A B Questions From Upper Extremities Lecture • Can you name the following landmarks? – C • Olecranon process – A • Head of the radius – B D • Medial epicondyle B A – D C • Lateral epicondyle Questions From Upper Extremities Lecture • Can you name the following bones and landmarks? – Which bone is A pointing to? • Ulna – Which bone is B pointing A to? • Radius E – C B • Styloid process of the ulna – D • Styloid process of the radius C – E D • Interosseous membrane of forearm Questions From Upper Extremities Lecture • Can you name the following bony landmarks? – Which landmark is A pointing to? • Lateral epicondyle of humerus – Which -

Small Muscles of the Hand
By the name of Allah Small muscles of the hand Revision: The palmar aponeurosis is triangular in shape with apex and base. It is divided into 4 bands that radiate to the medial four fingers. Dupuytren’s Contracture: • A localized thickening and shortening of palmar aponeurosis that limits hand function (it is permanent) • Fibrosis pulls the ring finger then the little finger into partial flexion at the MCP joints, followed by flexion of their proximal interphalangeal joints • Usual treatment: Treated by surgical excision of fibrous bands followed by physiotherapy. Alternative treatment: Injection of the enzyme Collagenase into the contracted bands of the fibrous tissue. Keep in mind: • When the muscle Isn’t functioning: It is Relaxed. While it is in action: It is contracted. • Contraction DIFFERS from contracture. Contracture means permanent shortening. 18 th \Mar\2012 1 Small muscles of the hand: Arranged in five groups + 1 muscle, as the following: 1- Thenar muscles: (three in number) each moves the thumb according to its name: • Flexor pollicis brevis: assists the flexor pollicis longus in the flexion of MCP joint of the thumb. • Abductor pollicis brevis: abduction of the thumb. • Opponens pollicis: pulls the thumb medially and forward across the palm (as in counting fingers, shown in the figure below). All supplied by median nerve. 2- Hypothenar muscles: (three in number) each moves the little finger according to its name: • Flexor digiti minimi. • Abductor digit minimi. • Opponens digiti minimi. All supplied by deep branch of ulnar nerve. Only the thumb and little finger got opponens muscles, the Dr said it is because of the long distance between the two fingers ☺ 3- Adductor pollicis muscle: • It has got two heads: horizontal( transverse) and Oblique. -

Extensor Pollicis Longus Superficialis and Extensor Indicis Superficialis, Can They Be Considered As a New Anatomical Variation in the Long Extensors of Fingers?
Int. J. Curr. Res. Med. Sci. (2016). 2(12): 27-32 International Journal of Current Research in Medical Sciences ISSN: 2454-5716 www.ijcrims.com Volume 2, Issue 12 -2016 Case study DOI: http://dx.doi.org/10.22192/ijcrms.2016.02.12.005 Extensor pollicis longus superficialis and extensor indicis superficialis, can they be considered as a new anatomical variation in the long extensors of fingers? Ahmed Farid Al-Neklawy, M.D. Anatomy and Embryology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt E-mail: [email protected], Tel: 00201001850336 Running title: Two extra muscles for thumb and index fingers Abstract Background: Variations of anomalies of hand extensors have been described by many authors. These anomalies are often discovered during routine surgical procedures and cadaveric dissections. Being aware of such anomalies is important to the physician in order to avoid unintentional damage to healthy tendons during surgical procedures. In addition, accessory tendons have the potential to be used in the surgical repair or replacement of damaged tendons. We reported a cadaveric case with bilateral two additional superficial extensors to the thumb and index fingers with unique features. The names of extensor pollicis longus superficialis (EPL-S) and extensor indicis superficialis(EI-S) were proposed. Methods: A female cadaver was used in this study. Bilateral dissection of the forearm and wrist was done. Results: Two extra muscles were observed in the superficial group of the extensors of the forearm. They were situated between extensor carpi radialis brevis and extensor digitorum muscles. Both muscles originated from the common extensor origin. -

Section 1 Upper Limb Anatomy 1) with Regard to the Pectoral Girdle
Section 1 Upper Limb Anatomy 1) With regard to the pectoral girdle: a) contains three joints, the sternoclavicular, the acromioclavicular and the glenohumeral b) serratus anterior, the rhomboids and subclavius attach the scapula to the axial skeleton c) pectoralis major and deltoid are the only muscular attachments between the clavicle and the upper limb d) teres major provides attachment between the axial skeleton and the girdle 2) Choose the odd muscle out as regards insertion/origin: a) supraspinatus b) subscapularis c) biceps d) teres minor e) deltoid 3) Which muscle does not insert in or next to the intertubecular groove of the upper humerus? a) pectoralis major b) pectoralis minor c) latissimus dorsi d) teres major 4) Identify the incorrect pairing for testing muscles: a) latissimus dorsi – abduct to 60° and adduct against resistance b) trapezius – shrug shoulders against resistance c) rhomboids – place hands on hips and draw elbows back and scapulae together d) serratus anterior – push with arms outstretched against a wall 5) Identify the incorrect innervation: a) subclavius – own nerve from the brachial plexus b) serratus anterior – long thoracic nerve c) clavicular head of pectoralis major – medial pectoral nerve d) latissimus dorsi – dorsal scapular nerve e) trapezius – accessory nerve 6) Which muscle does not extend from the posterior surface of the scapula to the greater tubercle of the humerus? a) teres major b) infraspinatus c) supraspinatus d) teres minor 7) With regard to action, which muscle is the odd one out? a) teres -
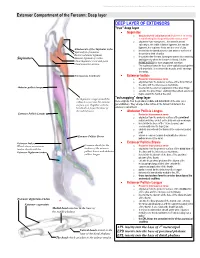
Extensor Compartment of the Forearm: Deep Layer
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. Extensor Compartment of the Forearm: Deep layer DEEP LAYER OF EXTENSORS "true" deep layer Supinator o deep branch of radial nerve which pierces it on its way to transforming into the posterior interosseous nerve o originates from everywhere... the lateral humeral epicondyle, the radial collateral ligament, the annular ligament, the supinator fossa and the crest of ulna Attachments of the Supinator to the o inserts into the lateral posterior and anterior surfaces of Epicondyle of humerus the proximal third of radius Radial collateral ligament o it supinates the forearm, turning the arm to face anteriorly Annular ligament of radius Supinator and superiorly when the forearm is flexed. It is the Ulnar Supinator crest and fossa PRIME MOVER for slow unopposed suination Ulnar posterior surface o The supinator forms the floor of the cubital fossa together with brachialis. It is a sheet-like muscle, and it envelops the radius. Interosseous membrane Extensor Indicis o Posterior interosseous nerve o originates from the posterior surface of the distal third of the ulna, and the interosseous membrane Abductor pollicis longus o inserts into the extensor expansion of the index finger o extends the index finger, enabling independent extension o helps extend the hand at the wrist "outcropping" deep layer the Supinator wraps around the radius to insert into the anterior these originate from the proximal, middle and distal thirds of the ulna (as a surface of it. -

Quadrilateral Space Syndrome
FUNCTIONAL REHABILITATION R. Barry Dale, PhD, PT, ATC, CSCS, Report Editor Quadrilateral Space Syndrome Robert C. Manske, PT, DPT, MEd, SCS, ATC, CSCS, Afton Sumler, ATC, and Jodi Runge, ATC • Wichita State University QUADRILATERAL space syndrome (QSS) is a History uncommon condition that has been reported to affect athletes who perform overhead QSS has been reported to have a spontaneous movement patterns, such as baseball play- onset during sport participation or as a result 1,2,7-15 ers,1-4 tennis players,5 and volleyball players.6 of acute trauma. Misdiagnosis may Cahill and Palmer7 described it as a rare be responsible for an underestimate of the 16 7 condition that involves compression of the prevalence of QSS. Cahill described four posterior humeral cir- cardinal features of QSS: (a) poorly localized cumflex artery (PHCA) shoulder pain, (b) nondermatomal distribu- Key PointsPoints and the axillary nerve tion of paresthesia, (c) discrete point ten- within the quadrilat- derness in the quadrilateral space, and (d) a Qaudrilateral space syndrome is an uncom- eral space, which pro- positive arteriogram finding with the affected mon condition. duces pain over the shoulder in a position of abduction and exter- posterior aspect of nal rotation. A high index of suspicion should Symptoms are caused by entrapment of the shoulder that may be maintained for this unusual diagnosis the axillary nerve within the quadrilateral in the overhead athlete who presents with space. radiate into the arm and forearm with a recalcitrant posterior shoulder pain. Conservative treatment should be non-dermatomal dis- attempted prior to surgical intervention. tribution.