Quarterly Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bangladesh Jobs Diagnostic.” World Bank, Washington, DC
JOBS SERIES Public Disclosure Authorized Issue No. 9 Public Disclosure Authorized DIAGNOSTIC BANGLADESH Public Disclosure Authorized Main Report Public Disclosure Authorized JOBS DIAGNOSTIC BANGLADESH Thomas Farole, Yoonyoung Cho, Laurent Bossavie, and Reyes Aterido Main Report © 2017 International Bank for Reconstruction and Development / The World Bank. 1818 H Street NW, Washington, DC 20433, USA. Telephone: 202-473-1000; Internet: www.worldbank.org. Some rights reserved This work is a product of the staff of The World Bank with external contributions. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of The World Bank, its Board of Executive Directors, or the govern- ments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Nothing herein shall constitute or be considered to be a limitation upon or waiver of the privileges and immunities of The World Bank, all of which are specifically reserved. Rights and Permissions This work is available under the Creative Commons Attribution 3.0 IGO license (CC BY 3.0 IGO) http://creativecommons.org/licenses/by/3.0/igo. Under the Creative Commons Attribution license, you are free to copy, distribute, transmit, and adapt this work, including for commercial purposes, under the following conditions: Attribution—Please cite the work as follows: Thomas Farole, Yoonyoung Cho, Laurent Bossavie, and Reyes Aterido. -
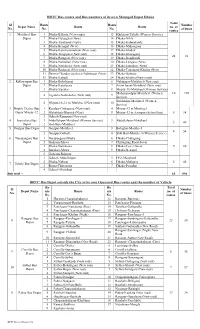
BRTC Bus Routes and Bus Numbers of Its Own Managed Depot Dhaka Total Sl Routs Routs Number Depot Name Routs Routs No
BRTC Bus routes and Bus numbers of its own Managed Depot Dhaka Total Sl Routs Routs Number Depot Name Routs Routs no. of No. No. No. of buses routes 1. Motijheel Bus 1 Dhaka-B.Baria (New routs) 13 Khilgoan-Taltola (Women Service) Depot 2 Dhaka-Haluaghat (New) 14 Dhaka-Nikli 3 Dhaka-Tarakandi (New) 15 Dhaka-Kalmakanda 4 Dhaka-Benapul (New) 16 Dhaka-Muhongonj 5 Dhaka-Kutichowmuhoni (New rout) 17 Dhaka-Modon 6 Dhaka-Tongipara (New rout) 18 Dhaka-Ishoregonj 24 82 7 Dhaka-Ramgonj (New rout) 19 Dhaka-Daudkandi 8 Dhaka-Nalitabari (New rout) 20 Dhaka-Lengura (New) 9 Dhaka-Netrakona (New rout) 21 Dhaka-Jamalpur (New) 10 Dhaka-Ramgonj (New rout) 22 Dhaka-Tongipara-Khulna (New) 11 Demra-Chandra via Savar Nabinagar (New) 23 Dhaka-Bajitpur 12 Dhaka-Katiadi 24 Dhaka-Khulna (New routs) 2. Kallayanpur Bus 1 Dhaka-Bokshigonj 6 Nabinagar-Motijheel (New rout) Depot 2 Dhaka-Kutalipara 7 Zirani bazar-Motijheel (New rout) 3 Dhaka-Sapahar 8 Mirpur-10-Motijheel (Women Service) Mohammadpur-Motijheel (Women 10 198 4 Zigatola-Notunbazar (New rout) 9 Service) Siriakhana-Motijheel (Women 5 Mirpur-10-2-1 to Motijheel (New rout) 10 Service) 3. Double Decker Bus 1 Kendua-Chittagong (New rout) 4 Mirpur-12 to Motijheel Depot Mirpur-12 2 Mohakhali-Bhairob (New) 5 Mirpur-12 to Azimpur (School bus) 5 38 3 Gabtoli-Rampura (New rout) 4. Joarsahara Bus 1 Abdullahpur-Motijheel (Women Service) 3 Abdullahpur-Motijheel 5 49 Depot 2 Shib Bari-Motijheel 5. Gazipur Bus Depot 1 Gazipur-Motijheel 3 Balughat-Motijheel 4 54 2 Gazipur-Gabtoli 4 Shib Bari-Motijheel (Women Service) 6. -

127 Branches
মেটলাইফ পলললির প্রিপ্রিয়াি ও অꇍযাꇍয মপমেন্ট বযা廬ক এপ্রিয়ার িকল শাখায় ꇍগদে প্রদান কমর তাৎক্ষপ্রিকভাদব বমু ে লনন ররপ্রভপ্রꇍউ স্ট্যাম্প ও সীলসহ রিটলাইদের প্ররপ্রসট এই িলু বধা পাওয়ার জনয গ্রাহকমক মকান অলিলরক্ত লফ অথবা স্ট্যাম্প চাজ জ প্রদান করমি হমব না Sl. No. Division District Name of Branches Address of Branch 1 Barisal Barisal Barishal Branch Fakir Complex 112 Birshrashtra Captain Mohiuddin Jahangir Sarak 2 Barisal Bhola Bhola Branch Nabaroon Center(1st Floor), Sadar Road, Bhola 3 Chittagong Chittagong Agrabad Branch 69, Agrabad C/ A, Chittagong 4 Chittagong Chittagong Anderkilla Branch 184, J.M Sen Avenue Anderkilla 5 Chittagong Chittagong Bahadderhat Branch Mamtaz Tower 4540, Bahadderhat 6 Chittagong Chittagong Bank Asia Bhaban Branch 39 Agrabad C/A Manoda Mansion (2nd Floor), Holding No.319, Ward No.3, College 7 Chittagong Comilla Barura Branch Road, Barura Bazar, Upazilla: Barura, District: Comilla. 8 Chittagong Chittagong Bhatiary Branch Bhatiary, Shitakunda 9 Chittagong Brahmanbaria Brahmanbaria Branch "Muktijoddha Complex Bhaban" 1061, Sadar Hospital Road 10 Chittagong Chittagong C.D.A. Avenue Branch 665 CDA Avenue, East Nasirabad 1676/G/1 River City Market (1st Floor), Shah Amant Bridge 11 Chittagong Chaktai Chaktai Branch connecting road 12 Chittagong Chandpur Chandpur Branch Appollo Pal Bazar Shopping, Mizanur Rahman Road 13 Chittagong Lakshmipur Chandragonj Branch 39 Sharif Plaza, Maddho Bazar, Chandragonj, Lakshimpur 14 Chittagong Noakhali Chatkhil Branch Holding No. 3147 Khilpara Road Chatkhil Bazar Chatkhil 15 Chittagong Comilla Comilla Branch Chowdhury Plaza 2, House- 465/401, Race Course 16 Chittagong Comilla Companigonj Branch Hazi Shamsul Hoque Market, Companygonj, Muradnagar J.N. -

Traditional Institutions As Tools of Political Islam in Bangladesh
01_riaz_055072 (jk-t) 15/6/05 11:43 am Page 171 Traditional Institutions as Tools of Political Islam in Bangladesh Ali Riaz Illinois State University, USA ABSTRACT Since 1991, salish (village arbitration) and fatwa (religious edict) have become common features of Bangladesh society, especially in rural areas. Women and non-governmental development organizations (NGOs) have been subjected to fatwas delivered through a traditional social institution called salish. This article examines this phenomenon and its relationship to the rise of Islam as political ideology and increasing strengths of Islamist parties in Bangladesh. This article challenges existing interpretations that persecution of women through salish and fatwa is a reaction of the rural community against the modernization process; that fatwas represent an important tool in the backlash of traditional elites against the impoverished rural women; and that the actions of the rural mullahs do not have any political links. The article shows, with several case studies, that use of salish and fatwa as tools of subjection of women and development organizations reflect an effort to utilize traditional local institutions to further particular interpretations of behavior and of the rights of indi- viduals under Islam, and that this interpretation is intrinsically linked to the Islamists’ agenda. Keywords: Bangladesh; fatwa; political Islam Introduction Although the alarming rise of the militant Islamists in Bangladesh and their menacing acts in the rural areas have received international media attention in recent days (e.g. Griswold, 2005), the process began more than a decade ago. The policies of the authoritarian military regimes that ruled Bangladesh between 1975 and 1990, and the politics of expediency of the two major politi- cal parties – the Awami League (AL) and the Bangladesh Nationalist Party (BNP) – enabled the Islamists to emerge from the political wilderness to a legit- imate political force in the national arena (Riaz, 2003). -

Water Pricing for Slum Dwellers in Dhaka Metropolitan Area: Is It Affordable?
WATER PRICING FOR SLUM DWELLERS IN DHAKA METROPOLITAN AREA: IS IT AFFORDABLE? Muhammad Mizanur Rahaman*, Tahmid Saif Ahmed & Abdullah Al-Hadi Department of Civil Engineering, University of Asia Pacific, House 8, Road 7, Dhanmondi, Dhaka -1205, Bangladesh Fax: +88029664950 Email: [email protected]; [email protected] Email: [email protected] *Corresponding author Abstract Bangladesh is facing serious water management challenge to ensure affordable water supply for all, especially in urban areas. Both the availability and the quality of water are decreasing in the poor urban areas. Besides, the population situation of the country is getting worst in Dhaka, the capital of Bangladesh, which became one of the megacities in the world in terms of population and urbanization. The aim of this research is to address the following question: “Are slum dwellers in Dhaka Metropolitan Area capable for paying for Dhaka Water Supply and Sewerage Authority’s (DWASA) services?”. This study focused on three slums in Dhaka Metropolitan Area namely Korail slum, Godown slum and Tejgaon slum to determine the current water price in these slums and to compare it with water price of other cities of the world. A field study has been conducted during July and August 2014. It involves semi structured questionnaire survey and focus group discussions with slum dwellers and various stakeholders. For secondary data source, a wide range of books, peer-reviewed articles, researcher documents, related websites and databases have been reviewed. Result shows that for domestic water use slum dwellers are paying about 7 to 14 times higher than legal connection holders covered by DWASA. -

Division Zila Upazila Name of Upazila/Thana 10 10 04 10 04
Geo Code list (upto upazila) of Bangladesh As On March, 2013 Division Zila Upazila Name of Upazila/Thana 10 BARISAL DIVISION 10 04 BARGUNA 10 04 09 AMTALI 10 04 19 BAMNA 10 04 28 BARGUNA SADAR 10 04 47 BETAGI 10 04 85 PATHARGHATA 10 04 92 TALTALI 10 06 BARISAL 10 06 02 AGAILJHARA 10 06 03 BABUGANJ 10 06 07 BAKERGANJ 10 06 10 BANARI PARA 10 06 32 GAURNADI 10 06 36 HIZLA 10 06 51 BARISAL SADAR (KOTWALI) 10 06 62 MHENDIGANJ 10 06 69 MULADI 10 06 94 WAZIRPUR 10 09 BHOLA 10 09 18 BHOLA SADAR 10 09 21 BURHANUDDIN 10 09 25 CHAR FASSON 10 09 29 DAULAT KHAN 10 09 54 LALMOHAN 10 09 65 MANPURA 10 09 91 TAZUMUDDIN 10 42 JHALOKATI 10 42 40 JHALOKATI SADAR 10 42 43 KANTHALIA 10 42 73 NALCHITY 10 42 84 RAJAPUR 10 78 PATUAKHALI 10 78 38 BAUPHAL 10 78 52 DASHMINA 10 78 55 DUMKI 10 78 57 GALACHIPA 10 78 66 KALAPARA 10 78 76 MIRZAGANJ 10 78 95 PATUAKHALI SADAR 10 78 97 RANGABALI Geo Code list (upto upazila) of Bangladesh As On March, 2013 Division Zila Upazila Name of Upazila/Thana 10 79 PIROJPUR 10 79 14 BHANDARIA 10 79 47 KAWKHALI 10 79 58 MATHBARIA 10 79 76 NAZIRPUR 10 79 80 PIROJPUR SADAR 10 79 87 NESARABAD (SWARUPKATI) 10 79 90 ZIANAGAR 20 CHITTAGONG DIVISION 20 03 BANDARBAN 20 03 04 ALIKADAM 20 03 14 BANDARBAN SADAR 20 03 51 LAMA 20 03 73 NAIKHONGCHHARI 20 03 89 ROWANGCHHARI 20 03 91 RUMA 20 03 95 THANCHI 20 12 BRAHMANBARIA 20 12 02 AKHAURA 20 12 04 BANCHHARAMPUR 20 12 07 BIJOYNAGAR 20 12 13 BRAHMANBARIA SADAR 20 12 33 ASHUGANJ 20 12 63 KASBA 20 12 85 NABINAGAR 20 12 90 NASIRNAGAR 20 12 94 SARAIL 20 13 CHANDPUR 20 13 22 CHANDPUR SADAR 20 13 45 FARIDGANJ -

Under Threat: the Challenges Facing Religious Minorities in Bangladesh Hindu Women Line up to Vote in Elections in Dhaka, Bangladesh
report Under threat: The challenges facing religious minorities in Bangladesh Hindu women line up to vote in elections in Dhaka, Bangladesh. REUTERS/Mohammad Shahisullah Acknowledgements Minority Rights Group International This report has been produced with the assistance of the Minority Rights Group International (MRG) is a Swedish International Development Cooperation Agency. non-governmental organization (NGO) working to secure The contents of this report are the sole responsibility of the rights of ethnic, religious and linguistic minorities and Minority Rights Group International, and can in no way be indigenous peoples worldwide, and to promote cooperation taken to reflect the views of the Swedish International and understanding between communities. Our activities are Development Cooperation Agency. focused on international advocacy, training, publishing and outreach. We are guided by the needs expressed by our worldwide partner network of organizations, which represent minority and indigenous peoples. MRG works with over 150 organizations in nearly 50 countries. Our governing Council, which meets twice a year, has members from 10 different countries. MRG has consultative status with the United Nations Economic and Minority Rights Group International would like to thank Social Council (ECOSOC), and observer status with the Human Rights Alliance Bangladesh for their general support African Commission on Human and Peoples’ Rights in producing this report. Thank you also to Bangladesh (ACHPR). MRG is registered as a charity and a company Centre for Human Rights and Development, Bangladesh limited by guarantee under English law: registered charity Minority Watch, and the Kapaeeng Foundation for supporting no. 282305, limited company no. 1544957. the documentation of violations against minorities. -

Bangladesh Country Report 2018
. Photo: Children near an unsecured former smelting site in the Ashulia area outside of Dhaka Toxic Sites Identification Program in Bangladesh Award: DCI-ENV/2015/371157 Prepared by: Andrew McCartor Prepared for: UNIDO Date: November 2018 Pure Earth 475 Riverside Drive, Suite 860 New York, NY, USA +1 212 647 8330 www.pureearth.org List of Acronyms ...................................................................................................................... 1 List of Annexes ......................................................................................................................... 1 Acknowledgements ................................................................................................................. 2 Introduction............................................................................................................................... 2 Background............................................................................................................................... 2 Toxic Sites Identification Program (TSIP) ............................................................................. 3 TSIP Training ...................................................................................................................................... 3 Implementation Strategy and Coordination with Government .......................................... 4 Program Implementation Activities ..................................................................................................... 4 Analysis of Environmental -

Impacts of Climate Variability on Major Food Crops in Selected Agro-Ecosystems of Bangladesh M
Ann.M. G. Bangladesh Miah, M. A. Agric. Rahman, (2016) M. 20(1 M. Rahman & 2) : 61-74 and S. R. Saha ISSN 1025-482X (Print)61 2521-5477 (Online) IMPACTS OF CLIMATE VARIABILITY ON MAJOR FOOD CROPS IN SELECTED AGRO-ECOSYSTEMS OF BANGLADESH M. G. Miah*1, M. A. Rahman1, M. M. Rahman1 and S. R. Saha1 Abstract The agriculture of Bangladesh has been recognized as one of the most vulnerable sectors to the impacts of climate change due to its juxtaposing geographical position. This study examined the nexus between long-term (1960–2014) climate variables with the yield and area of major food crops in selected agro-ecosystems (Gazipur, Comilla, Jessore, and Dinajpur) of Bangladesh. Secondary data from the Bangladesh Meteorological Department (BMD) were used in analyzing climate variability for all the studied locations. Data of crop yields were collected from the Department of Agricultural Extension (DAE) local offices and respective farmers. Fifty farmers from each site were selected randomly and interviewed to investigate the farmers’ perceptions regarding the climate change phenomenon and its impact on crop production. Results showed the increasing trend of temperatures with time, which became more pronounced in Jessore and Dinajpur. Annual rainfall also revealed an increasing trend in all locations except Comilla. The analyses of Lower Confidence Level (LCL) and Upper Confidence Level (UCL) clearly indicated that the climate in recent years (1990–2014) changed conspicuously compared to that in 30 years ago (1960– 1989). Results of Standardized Precipitation Index (SPI) indicated drought intensity, which was distinct in Dinajpur and Jessore. Although area under crop production had declined, yields showed an increasing trend in all locations because of technological advances. -
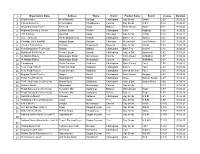
Organization Name Address Thana Distric Product Name Brand
1 Organization Name Address Thana Distric Product Name Brand License Duration 2 Shanti Bricks West Aburkhil Raozan Chattogram Clay Bricks Shanti C-03 30.06.22 3 Chiora Bricks Co Chiora Bazar Choddogram Cumilla Clay Bricks C B C C-12 30.06.21 4 Shahi Bakery & Confec. TA Road Sadar B-Baria White Bread Shahi C-17 30.06.21 5 Highway Sweets & Confec. Lalkhan Bazar Khulshi Chattogram Cake Highway C-20 30.06.22 6 A M S Bricks Moishadi Sadar Chandpur Clay Bricks A M S C-26 30.06.22 7 S.S. Tea House 99, Reazuddin road Kotwali Chattogram Black Tea Aurnov C-27 30.06.20 8 Chandan Oil & Atta Mill Hajiganj Bazar Hajiganj Chandpur Mustard Oil Jora Kobutar C-28 30.06.20 9 Amanat Bricks Manu Amnatpur Begumganj Noakhali Clay Bricks A B M C-40 30.06.20 10 New Bangladesh Tea House Bakalia Bakalia Chattogram Black Tea Nayem C-45 30.06.22 11 Bashkhali Salt Mills Ltd. Firingee Bazar Kotwali Chattogram Iodized Salt Bashkhali C-52 30.06.20 12 Al-Madina Bakery Muradnagar Bazar Muradnagar Cumilla White Bread Al-Madina C-57 30.06.22 13 Al-Madina Bakery Muradnagar Bazar Muradnagar Cumilla Biscuit Al-Madina C-58 30.06.22 14 Chadgaong South Burirchar Hathazari Chattogram White Bread Fulel C-60 30.06.22 15 Fulel Food Product South Burirchar Hathazari Chattogram Biscuit Fulel C-61 30.06.22 16 Fulel Food Product South Burichor Hathazari Chattogram Lachsa Shemai Fulel C-62 30.06.22 17 Bagdad Bread Factory Oxygen Baizid Chattogram White Bread Bagdad C-63 30.06.22 18 Tahar Food Products Nasirabad I/a Baizid Chattogram Ghee Danofa, Recipi C-67 30.06.21 19 Tarik Hasan Salt Crushing Ind. -

A Puzzle in the Hindu Population Growth in Bangladesh
A puzzle in the Hindu population growth in Bangladesh Background: Bangladesh is a plural society with Muslims, Hindus, Christians, Buddhists, and tribal faiths [1]. In 2011, Muslims constituted 90.4%, Hindus 8.5%, Christians 0.3%, and Buddhists 0.6% (Table 1). Only 0.1% people are affiliated with other faiths most of which are probably from the tribal populations. There has not been much change in the proportion of Christian, Buddhist, and other religious group over the 60 year period 1951-2011, but the proportion of Hindu population declined dramatically from 22.0% in 1951 to 8.5% in 2011. The pace of decline seems to be higher in the period between 1951 and 1981 than between 1981 and 2011. The shrinking of the relative share of Non-Muslim population is striking. As expected, the absolute size of all the religious groups has increased. However, population growth rates were different for different religious groups, highest for the Muslims, followed by Christians, Buddhists, and Hindus. Markedly very low rate of growth is observed for the Hindus. Because of substantially higher growth rate of Muslims than Hindus, the relative proportion of Hindu population has declined. Migration was a key element of population change in the early days of East Pakistan, now Bangladesh. Approximately 4.7 million Hindus sought refuge in India from the then East Pakistan between 1947 and 1971 [2], and also lots of Muslims migrated to East Pakistan from India but that number was thought to be much lower than the Hindu migration. Table 1 Population distribution -

Outlet of Robi
Zone Distributor Name Contract Person Name Mobile number Address Barisal Ma Telecom MD Yesuf 8801611111013 Patuakhali, SADAR Barisal MS Smart Tel Md. Neaz Morshed 8801828113311 Talukdar Bhaban, 2nd Floor, Sadar Road , Bhola Barisal M/S Anamika Enterprise MD Kamal Hossain 8801859700700 Barisal Sadar Road Barisal Robi Axiata Ltd Holding: 1160, Ground Floor Karim Kutir, Mohona Manjil, Barisal Nobogram Road infront of Karim Kuthi Mashjide Barishal Phone: +8801833182369 Robi Axiata Ltd R D Tower Bogra Shaheed Abdul Jabbar Road, Kalibari, Joleshowritola , Bogra Phone: +8801833182439 SD Tower (3rd Floor), Jhaotola, Chokjaduroad, Sadar, Bogura R. K. Agro Rafid Hasan Khan 8801814999666 Bogura-5800 Robi Axiata Ltd 96, Chowdhury Plaza (3rd Floor) Chittagong Metro-01 Behind Of Chittagong Shopping Complex Nasirabad, Panchlish, Chittagong Phone: +8801833181761 Shomobay Market (1st floor), Moshjid Road, Sadar CTG Metero-3 Yes Enterprise Md. Mizanur Rahman 8801820700700 Khagrachari Puraton Bus stand , Reserve Bazar, Rangamati Sadar , CTG Metro 1 JB Enterprise Abser Uddin 8801864363636 Rangamati Shamim Corporation, 5063, CJKS Shopping Complex, 4th CTG Metro 1 Shamim Corporation Network Showkat Osman 8801614005050 floor, Nur Ahmed Road, Kotwali, Chattogram. CTG Metro 1 KS Enterprise Mithun Shaha 8801611376328 Collage Gate, Rangamati Sadar, Rangamati. CTG Metro-2 Scorp International Md Sazzad 8801839908890 Saleh Tower(3rd Floor), Freeport, Bandar, Ctg ANIS MANSION, CHUNKUTIA CHOWRASTHA KERANIGANJ ALIF CORPORATION MD. MOHIUDDIN SALMAN 8801620200000 SOUTH KERANIGONJ | DHAKA-1310 Alam shaheb's building 1st floor, Room no: A-4, infront of TMSS, shahajalal islami bank goli,Opposite of Shiuli Chittagong Metro-03 Petrol Pump, Alankar more, Chittagong. Phone: 8801833181144 Robi Axiata Ltd 111, No Fakirhat Road Hazi Khalilur Rahman Mistri Bari Chittagong Metro-02 Middle Gosaildanga, Bandar,Chittagong Phone:+8801833182765 Robi Axiata Ltd Gias & Johor Villa Cox's Bazar Holding No: 117, Word No: 10, North Baharchora New Circuit House Road, Cox's Bazar.