A Patient's G a Patient's Guide to Scaphoid Fracture of the Wrist
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fractures Long Bones, Upper Limb (Includes Hand)
Ministry of Defence Synopsis of Causation Fractures Long Bones, Upper Limb (includes hand) Author: Mr John A Dent, Ninewells Hospital and Medical School, Dundee Validator: Mr Sheo Tibrewal, Queen Elizabeth Hospital, London September 2008 Disclaimer This synopsis has been completed by medical practitioners. It is based on a literature search at the standard of a textbook of medicine and generalist review articles. It is not intended to be a meta-analysis of the literature on the condition specified. Every effort has been taken to ensure that the information contained in the synopsis is accurate and consistent with current knowledge and practice and to do this the synopsis has been subject to an external validation process by consultants in a relevant specialty nominated by the Royal Society of Medicine. The Ministry of Defence accepts full responsibility for the contents of this synopsis, and for any claims for loss, damage or injury arising from the use of this synopsis by the Ministry of Defence. 2 1. Definition 1.1. A bone breaks as a result of a variety of injuring forces. The fracture produced in a long bone may be of its shaft or diaphysis; towards one of its ends where the bone widens (metaphysis); or of the end of the bone, where it forms a joint with the next bone (Figure 1). Fractures near a joint may involve the joint surface causing intra-articular fractures. 1.2. It must always be remembered that the soft tissues surrounding the bone will also be damaged to a varying extent by the injuring force. -
What Is a Scaphoid Fracture?
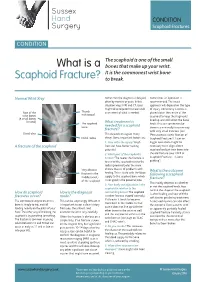
Sussex Hand CONDITION Surgery Scaphoid Fractures CONDITION The scaphoid is one of the small What is a bones that make up your wrist. It is the commonest wrist bone Scaphoid Fracture? to break. Normal Wrist Xray Sometimes the diagnosis is delayed, Sometimes an operation is often by months or years. In this recommended. The exact situation xrays, MRI and CT scans approach will depend on the type might all be required to make a full of injury. Commonly a screw is Rest of the Thumb assessment of what is needed. placed down the centre of the metacarpal wrist bones scaphoid to keep the fragments (8 small bones lined up and still whilst the bone in total) The scaphoid What treatment is heals. This can sometimes be bone needed for a scaphoid done in a minimally invasive way fracture? with very small incisions (see Distal ulna This depends on a great many ‘Percutaneous screw fixation of Distal radius things. Some important factors are: Scaphoid Fractures’). Later on 1. How old is the injury? Fresh bigger operations might be A fracture of the scaphoid fractures have better healing necessary to re-align a bent potential scaphoid and put new bone into 2. Which part of the scaphoid is the old fracture (see ‘ORIF of broken? The nearer the fracture is Scaphoid Fractures +/-bone to end of the scaphoid next to the grafting’). radius (proximal pole) the more Very obvious chance there is of problems with What is the outcome fracture in the healing. This is to do with the blood following a scaphoid middle (waist) supply to the scaphoid bone which fracture? of the scaphoid is not good in the proximal pole. -

EM Cases Digest Vol. 1 MSK & Trauma
THE MAGAZINE SERIES FOR ENHANCED EM LEARNING Vol. 1: MSK & Trauma Copyright © 2015 by Medicine Cases Emergency Medicine Cases by Medicine Cases is copyrighted as “All Rights Reserved”. This eBook is Creative Commons Attribution-NonCommercial- NoDerivatives 3.0 Unsupported License. Upon written request, however, we may be able to share our content with you for free in exchange for analytic data. For permission requests, write to the publisher, addressed “Attention: Permissions Coordinator,” at the address below. Medicine Cases 216 Balmoral Ave Toronto, ON, M4V 1J9 www.emergencymedicinecases.com This book has been authored with care to reflect generally accepted practices. As medicine is a rapidly changing field, new diagnostic and treatment modalities are likely to arise. It is the responsibility of the treating physician, relying on his/her experience and the knowledge of the patient, to determine the best management plan for each patient. The author(s) and publisher of this book are not responsible for errors or omissions or for any consequences from the application of the information in this book and disclaim any liability in connection with the use of this information. This book makes no guarantee with respect to the completeness or accuracy of the contents within. OUR THANKS TO... EDITORS IN CHIEF Anton Helman Taryn Lloyd PRODUCTION EDITOR Michelle Yee PRODUCTION MANAGER Garron Helman CHAPTER EDITORS Niran Argintaru Michael Misch PODCAST SUMMARY EDITORS Lucas Chartier Keerat Grewal Claire Heslop Michael Kilian PODCAST GUEST EXPERTS Andrew Arcand Natalie Mamen Brian Steinhart Mike Brzozowski Hossein Mehdian Arun Sayal Ivy Cheng Sanjay Mehta Laura Tate Walter Himmel Jonathan Pirie Rahim Valani Dave MacKinnon Jennifer Riley University of Toronto, Faculty of Medicine EM Cases is a venture of the Schwartz/ Reisman Emergency Medicine Institute. -

The Differential Diagnosis of Bone Marrow Edema on Wrist MRI
Skeletal Radiology (2019) 48:1525–1539 https://doi.org/10.1007/s00256-019-03204-1 REVIEW ARTICLE Review article: the differential diagnosis of bone marrow edema on wrist MRI WanYin Lim1,2 & Asif Saifuddin3,4 Received: 5 December 2018 /Revised: 1 February 2019 /Accepted: 5 March 2019 /Published online: 22 March 2019 # ISS 2019 Abstract There is a large variety of conditions that can result in ‘bone marrow edema’ or ‘bone marrow lesions’ (BML) in the wrist on magnetic resonance imaging (MRI). The combination of clinical history and the distribution of the BML can serve as a valuable clue to a specific diagnosis. This article illustrates the different patterns of BML in the wrist to serve as a useful guide when reviewing wrist MRI studies. Imaging artefacts will also be briefly covered. Keywords MRI . Wrist . Marrow edema . Bone marrow lesion Introduction The etiology of BMLs can also be confusing due to the non-specific appearance, MRI demonstrating poorly defined Bone marrow lesions (BML), or marrow signal reduced T1-weighted spin echo (T1W SE) marrow signal in- hyperintensity on fluid-sensitive magnetic resonance im- tensity (SI) (Fig. 1a) with corresponding hyperintensity on aging (MRI) sequences, are observed in up to 36% of short tau inversion recovery (STIR), fat-suppressed T2W fast patients undergoing wrist MRI [1]. With regard to def- spin echo (FS T2W FSE), and fat-suppressed proton density- inition, the term ‘bone marrow lesion’ (BML) used in weighted fast spin echo (FS PDW FSE) sequences (Fig. 1b). this manuscript is synonymous with ‘edema-like marrow There may also be overlapping patterns between different en- signal’, ‘marrow edema-like signal’ or ‘bone marrow tities, but the combination of clinical history and lesion loca- edema pattern’ [2]. -

Scaphoid Fracture PA Radiograph
30 y/o male with acute left wrist pain Student Name….None was listed Atul Kumar, MD, MS PA Radiograph Non Contrast Coronal CT ? Scaphoid Fracture PA radiograph Distal pole Scaphoid fracture Proximal pole • PA x-ray showing transverse scaphoid fracture. Non Contrast Coronal CT Capitate Trapezoid Hamate Trapezium Triquetrum Lunate Scaphoid fracture Scaphoid Fracture • Mechanism: direct axial compression or with hyperextension (fall onto an outstretched hand). • Symptoms: pain localized at the radial aspect of wrist often associated with swelling and reduced grip strength. – Pain in anatomic snuffbox suspicious for waist fracture, which is the most common type. • Because scaphoid fractures are often radiologically occult, any tenderness in the anatomic snuffbox should be treated as a scaphoid fracture. • Scaphoid blood supply (palmar carpal branch of the radial artery) runs from the distal to the proximal pole. Transverse fracture of the proximal pole can lead to osteonecrosis and nonunion due to disruption of blood flow. http://epmonthly.com/wp-content/uploads/2016/04/OrthoB.png Scaphoid Fracture • Differential diagnosis: distal radius fracture, wrist sprain, and other carpal injuries other than scaphoid. • In suspected scaphoid fractures, plain radiographs (including PA, true lateral, oblique, and scaphoid views) are ordered as the first diagnostic step. • However, the false negative rate for radiographs taken immediately after injury up to 20-54%. • Definitive diagnosis can be made by MRI or CT scan. They have a comparable diagnostic accuracy and do not result in overtreatments. Avascular necrosis/Nonunion Scaphoid view radiograph (A) and CT scan (B) showing nonunion (arrow) and avascular necrosis (asterisk) and the Terry Thomas sign – scapholunate ligament injury (arrowhead). -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -

17 Radial Styloidectomy David M
17 Radial Styloidectomy David M. Kalainov, Mark S. Cohen, and Stephanie Sweet xcision of the radial styloid gained recognition osteotomy removed 92% of the radioscaphocapitate in 1948 when Barnard and Stubbins1 reported on and 21% of the long radiolunate ligament origins. The Eten scaphoid fracture nonunions treated with transverse osteotomy was the most invasive, detach- bone grafting and radial styloidectomy. The procedure ing 95% of the radioscaphocapitate and 46% of the has since been advocated to address radioscaphoid long radiolunate ligament origins. arthritis developing from a variety of injuries, includ- In another cadaveric model, Nakamura et al19 ex- ing previous fractures of the radial styloid and scaphoid, amined the effects of increasingly larger oblique sty- and arthritis related to posttraumatic scapholunate loidectomies on carpal stability. They concluded that instability.2–8 the procedure should be limited to a 3- to 4-mm bony Resection of the radial styloid has also been a use- resection. With axial loading, significantly increased ful adjunct to other procedures where there is poten- radial, ulnar, and palmar displacements of the carpus tial for impingement between the styloid process and were detected after removing 6-mm and 10-mm sty- distal scaphoid or trapezium.9–15 Authors have in- loid segments. The 6-mm cut violated the radio- cluded discussion of successful radial styloidectomy scaphocapitate ligament origin, whereas the 10-mm in descriptions of proximal row carpectomy, mid- cut removed the radioscaphocapitate and a portion of carpal arthrodesis, and triscaphe fusion procedures. the long radiolunate ligament origins. Only an in- On occasion, an individual may be too physically un- significant change in carpal translation was detected fit or unwilling to undergo an extensive operation to after a 3-mm osteotomy. -

Wrist Injury Article 12-19-16
ARTICLE: Wrist Injuries This week we are going to talk about 3 unusual wrist injuries all of which can cause considerable problems and the potential complications of each. The first is a TFCC injury. The TFCC or triangular fibrocartilage is a small meniscus or pad on the ulnar side of the wrist (pinky side) which can become torn during a fall on an outstretched hand and can cause clicking, popping and pain on this side of the wrist. The TFCC is sometimes difficult to detect and often misdiagnosed as a wrist sprain but is rather different than a sprained wrist in that it is not an injury of ligament but is an injury of cartilage. The injury can be spotted with a shear test and is properly diagnosed with an arthrogram. The second unusual injury to the wrist is the scaphoid fracture. The scaphoid fracture of the wrist is a bone injury which occurs when the scaphoid bone on the radial side of the wrist (thumb side) is broken at it’s waist (center) injuring the blood supply to the proximal pole of the scaphoid. This injury results in avascular necrosis or bone death of the scaphoid. Also occurring after a fall on an outstretched hand the scaphoid fracture is often misdiagnosed as a wrist sprain but is more correctly described as a fracture. The hallmark symptom of a scaphoid fracture is it’s failure to heal and persistent pain on the radial side of the wrist. The scaphoid fracture is often missed on the initial x-ray as the bone has not had time yet to die off and is often seen on a second film. -

Treatment of Scaphoid Nonunion with Olecranon Bone Graft and Compression Screw
DOI: http://dx.doi.org/10.1590/1413-785220162403155935 ORIGINAL ARTICLE TREATMENT OF SCAPHOID NONUNION WITH OLECRANON BONE GRAFT AND COMPRESSION SCREW ANTONIO TUFI NEDER FILHO1, EDUARDO TRALDI FRANCESCHINI2, ARLINDO GOMES PARDINI JÚNIOR2, MARCELO RIBERTO3, NILTON MAZZER3 1. Hospital Lifecenter, Belo Horizonte, MG, Brazil. 2. Hospital Ortopédico, Belo Horizonte, MG, Brazil. 3. Universidade de São Paulo, Faculdade de Medicina de Ribeirão Preto. Ribeirão Preto, SP, Brazil. ABSTRACT of the handgrip strength of the non-affected side, which was Objective: To evaluate the outcome of olecranon bone graft 37 kgf. The DASH score averaged 5 points. Conclusion: We and compression screw for the treatment of nonunion of believe that the use of bone graft obtained from the olecranon the Lichtman type I scaphoid. Method: We evaluated 15 pa- and secured with cannulated screw is a resolute technique for tients of 32 who underwent surgical treatment for nonunion cases of linear nonunion of the Lichtmann type I scaphoid. It of the Lichtman type I scaphoid with olecranon bone graft has the advantages of a new anesthesia for removal of the and screw compression. Results: We obtained 100% con- graft and the access is easy, providing a good exposure for solidation in our sample. The mean flexion of the wrist on removal and good aesthetic results. Level of evidence IV. the affected side was 68° and 75° on the non-affected side. Case series. The average extension was 63° and 72°, respectively. The average grip strength was 35 kgf. This corresponds to 98% Keywords: Scaphoid bone. Pseudarthrosis. Bone transplantation. Citation: Neder Filho AT, Franceschini ET, Pardini Junior AG, Riberto M, Mazzer N. -

What Is the Scaphoid View ?
Journal of Indonesian Orthopaedic, Volume 40, Number 3, December 2012 7 What is The Scaphoid view ? Djunifer Hasudungan Sagala, Henry Yurianto, M. Ruksal Saleh, Idrus A. Paturusi Department of Orthopaedic and Traumatology Faculty of Medicine, Hasanuddin University, Wahidin Sudirohusodo General Hospital Makassar, Indonesia ABSTRACT Introduction. More than 60% of wrist injuries are associated with scaphoid bone fractures in young active people. Scaphoid fracture dif›cult to diagnose on initial radiography due to unique and complex structures of scaphoid bone, its overlapping position between other carpals bone and still no general consensus about how and which radiographic view should be taken for better expose. This let scaphoid fracture into potential complication such as non-union, delayed union, decrease of wrist joint motion, osteoarthritis of radiocarpal joint and avascular necrosis. Materials and Methods. Serial initial projection of radiograph was investigated to get the better view of scaphoid bone. Postero-anterior projection within wrist joint in extension 10°, 15°, and 20° with maximum ulnar deviation using wrist joint frame was found making the scaphoid clearer. The database was compared to get the ideal view of scaphoid. Extension and ulnar deviation were performed due to fiexed position of scaphoid anatomically in neutral wrist joint position. Results. Good exposure of scaphoid is got from performing radiographic examination of wrist joint 10° extended with maximum ulnar deviation position, in a total of 60 right and left wrist joint samples of young active men and women. Conclusions. Ten degrees extension with ulnar deviation wrist joint position can be proposed to be one of standard scaphoid view on plain radiography. -

Your Wrist Bones
www.healthinfo.org.nz Your wrist bones Your wrist is made up of eight small bones (called the carpal bones). Each carpal bone has a specific name, shown in the image on the right. The carpal bones connect with the two long bones in your forearm (the radius and ulna). Your wrist moves where they connect. This makes your wrist a very complex structure, as there are many different joints within it. If any one of your carpal bones breaks, it can change position slightly, causing pain and problems with movement. Occasionally it can also lead to arthritis. Causes of a broken wrist A broken wrist usually happens from falling on to an outstretched hand. Serious accidents, such as car accidents, motorcycle accidents, or falls from a ladder cause more serious breaks. Weak bones (for example, in someone with osteoporosis) tend to break more easily. If you break your wrist without significant force, your doctor may recommend checking if you have osteoporosis. If you meet the criteria, they may send you for a bone density scan. Any one of the 10 bones in your wrist can break, but the most common bone to break is the radius, in your forearm. This is called a distal radius fracture. Another common wrist fracture is a scaphoid fracture, which is a break in one of your small carpal bones. This can be difficult to diagnose, and there is a risk a scaphoid fracture might not heal. Your wrist can break in many different ways, and some breaks are worse than others. How bad a break it is depends on how many pieces a bone breaks into, whether they are stable or move around a lot, and whether the broken ends of the bone are still in the right place. -

Imaging and Treatment of Scaphoid Fractures and Their Complications
159 Imaging and Treatment of Scaphoid Fractures and Their Complications Mihra S. Taljanovic, M.D., M.Sc., F.A.C.R. 1 Apostolos Karantanas, M.D., Ph.D. 2, 3 James F. Griffith, M.D. 4 Gregory L. DeSilva, M.D. 5 Joshua D. Rieke, M.D. 1 Joseph E. Sheppard, M.D. 5 1 Department of Medical Imaging, The University of Arizona Health Address for correspondence and reprint requests Mihra S. Taljanovic, Network, Tucson, Arizona. M.D., M.Sc., Department of Medical Imaging, The University of Arizona 2 Department of Radiology, University of Crete, Heraklion, Greece. Health Network, 1501 N. Campbell Ave., Tucson, AZ 85724-5067 3 Department of Medical Imaging, University Hospital, Heraklion, (e-mail: [email protected]). Greece. 4 Department of Imaging and Interventional Radiology, Prince of Wales Hospital, Shatin, New Territories, Hong Kong. 5 Department of Orthopaedic Surgery, The University of Arizona Health Network, Tucson, Arizona. Semin Musculoskelet Radiol 2012;16:159–174. Abstract The scaphoid is the most commonly fractured carpal bone, with frequent complications that are predisposed by its anatomical location, anatomical configuration (shape and length), and vascular supply. The most common mechanism of injury is a fall onto an outstretched hand. Imaging plays a significant role in the initial evaluation and treatment of scaphoid fractures and their complications. Radiography should be the first imaging modality in the initial evaluation and follow-up of scaphoid fractures. Computed tomography with its superb spatial resolution enables better visualization and charac- terization of the fracture line, and the amount of displacement and angulation of the fracture fragments.