Fractures Long Bones, Upper Limb (Includes Hand)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
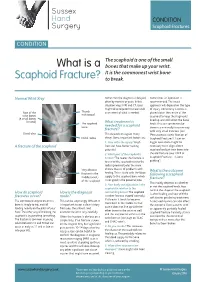
What Is a Scaphoid Fracture?
Sussex Hand CONDITION Surgery Scaphoid Fractures CONDITION The scaphoid is one of the small What is a bones that make up your wrist. It is the commonest wrist bone Scaphoid Fracture? to break. Normal Wrist Xray Sometimes the diagnosis is delayed, Sometimes an operation is often by months or years. In this recommended. The exact situation xrays, MRI and CT scans approach will depend on the type might all be required to make a full of injury. Commonly a screw is Rest of the Thumb assessment of what is needed. placed down the centre of the metacarpal wrist bones scaphoid to keep the fragments (8 small bones lined up and still whilst the bone in total) The scaphoid What treatment is heals. This can sometimes be bone needed for a scaphoid done in a minimally invasive way fracture? with very small incisions (see Distal ulna This depends on a great many ‘Percutaneous screw fixation of Distal radius things. Some important factors are: Scaphoid Fractures’). Later on 1. How old is the injury? Fresh bigger operations might be A fracture of the scaphoid fractures have better healing necessary to re-align a bent potential scaphoid and put new bone into 2. Which part of the scaphoid is the old fracture (see ‘ORIF of broken? The nearer the fracture is Scaphoid Fractures +/-bone to end of the scaphoid next to the grafting’). radius (proximal pole) the more Very obvious chance there is of problems with What is the outcome fracture in the healing. This is to do with the blood following a scaphoid middle (waist) supply to the scaphoid bone which fracture? of the scaphoid is not good in the proximal pole. -

The Differential Diagnosis of Bone Marrow Edema on Wrist MRI
Skeletal Radiology (2019) 48:1525–1539 https://doi.org/10.1007/s00256-019-03204-1 REVIEW ARTICLE Review article: the differential diagnosis of bone marrow edema on wrist MRI WanYin Lim1,2 & Asif Saifuddin3,4 Received: 5 December 2018 /Revised: 1 February 2019 /Accepted: 5 March 2019 /Published online: 22 March 2019 # ISS 2019 Abstract There is a large variety of conditions that can result in ‘bone marrow edema’ or ‘bone marrow lesions’ (BML) in the wrist on magnetic resonance imaging (MRI). The combination of clinical history and the distribution of the BML can serve as a valuable clue to a specific diagnosis. This article illustrates the different patterns of BML in the wrist to serve as a useful guide when reviewing wrist MRI studies. Imaging artefacts will also be briefly covered. Keywords MRI . Wrist . Marrow edema . Bone marrow lesion Introduction The etiology of BMLs can also be confusing due to the non-specific appearance, MRI demonstrating poorly defined Bone marrow lesions (BML), or marrow signal reduced T1-weighted spin echo (T1W SE) marrow signal in- hyperintensity on fluid-sensitive magnetic resonance im- tensity (SI) (Fig. 1a) with corresponding hyperintensity on aging (MRI) sequences, are observed in up to 36% of short tau inversion recovery (STIR), fat-suppressed T2W fast patients undergoing wrist MRI [1]. With regard to def- spin echo (FS T2W FSE), and fat-suppressed proton density- inition, the term ‘bone marrow lesion’ (BML) used in weighted fast spin echo (FS PDW FSE) sequences (Fig. 1b). this manuscript is synonymous with ‘edema-like marrow There may also be overlapping patterns between different en- signal’, ‘marrow edema-like signal’ or ‘bone marrow tities, but the combination of clinical history and lesion loca- edema pattern’ [2]. -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -

17 Radial Styloidectomy David M
17 Radial Styloidectomy David M. Kalainov, Mark S. Cohen, and Stephanie Sweet xcision of the radial styloid gained recognition osteotomy removed 92% of the radioscaphocapitate in 1948 when Barnard and Stubbins1 reported on and 21% of the long radiolunate ligament origins. The Eten scaphoid fracture nonunions treated with transverse osteotomy was the most invasive, detach- bone grafting and radial styloidectomy. The procedure ing 95% of the radioscaphocapitate and 46% of the has since been advocated to address radioscaphoid long radiolunate ligament origins. arthritis developing from a variety of injuries, includ- In another cadaveric model, Nakamura et al19 ex- ing previous fractures of the radial styloid and scaphoid, amined the effects of increasingly larger oblique sty- and arthritis related to posttraumatic scapholunate loidectomies on carpal stability. They concluded that instability.2–8 the procedure should be limited to a 3- to 4-mm bony Resection of the radial styloid has also been a use- resection. With axial loading, significantly increased ful adjunct to other procedures where there is poten- radial, ulnar, and palmar displacements of the carpus tial for impingement between the styloid process and were detected after removing 6-mm and 10-mm sty- distal scaphoid or trapezium.9–15 Authors have in- loid segments. The 6-mm cut violated the radio- cluded discussion of successful radial styloidectomy scaphocapitate ligament origin, whereas the 10-mm in descriptions of proximal row carpectomy, mid- cut removed the radioscaphocapitate and a portion of carpal arthrodesis, and triscaphe fusion procedures. the long radiolunate ligament origins. Only an in- On occasion, an individual may be too physically un- significant change in carpal translation was detected fit or unwilling to undergo an extensive operation to after a 3-mm osteotomy. -

Treatment of Scaphoid Nonunion with Olecranon Bone Graft and Compression Screw
DOI: http://dx.doi.org/10.1590/1413-785220162403155935 ORIGINAL ARTICLE TREATMENT OF SCAPHOID NONUNION WITH OLECRANON BONE GRAFT AND COMPRESSION SCREW ANTONIO TUFI NEDER FILHO1, EDUARDO TRALDI FRANCESCHINI2, ARLINDO GOMES PARDINI JÚNIOR2, MARCELO RIBERTO3, NILTON MAZZER3 1. Hospital Lifecenter, Belo Horizonte, MG, Brazil. 2. Hospital Ortopédico, Belo Horizonte, MG, Brazil. 3. Universidade de São Paulo, Faculdade de Medicina de Ribeirão Preto. Ribeirão Preto, SP, Brazil. ABSTRACT of the handgrip strength of the non-affected side, which was Objective: To evaluate the outcome of olecranon bone graft 37 kgf. The DASH score averaged 5 points. Conclusion: We and compression screw for the treatment of nonunion of believe that the use of bone graft obtained from the olecranon the Lichtman type I scaphoid. Method: We evaluated 15 pa- and secured with cannulated screw is a resolute technique for tients of 32 who underwent surgical treatment for nonunion cases of linear nonunion of the Lichtmann type I scaphoid. It of the Lichtman type I scaphoid with olecranon bone graft has the advantages of a new anesthesia for removal of the and screw compression. Results: We obtained 100% con- graft and the access is easy, providing a good exposure for solidation in our sample. The mean flexion of the wrist on removal and good aesthetic results. Level of evidence IV. the affected side was 68° and 75° on the non-affected side. Case series. The average extension was 63° and 72°, respectively. The average grip strength was 35 kgf. This corresponds to 98% Keywords: Scaphoid bone. Pseudarthrosis. Bone transplantation. Citation: Neder Filho AT, Franceschini ET, Pardini Junior AG, Riberto M, Mazzer N. -

What Is the Scaphoid View ?
Journal of Indonesian Orthopaedic, Volume 40, Number 3, December 2012 7 What is The Scaphoid view ? Djunifer Hasudungan Sagala, Henry Yurianto, M. Ruksal Saleh, Idrus A. Paturusi Department of Orthopaedic and Traumatology Faculty of Medicine, Hasanuddin University, Wahidin Sudirohusodo General Hospital Makassar, Indonesia ABSTRACT Introduction. More than 60% of wrist injuries are associated with scaphoid bone fractures in young active people. Scaphoid fracture dif›cult to diagnose on initial radiography due to unique and complex structures of scaphoid bone, its overlapping position between other carpals bone and still no general consensus about how and which radiographic view should be taken for better expose. This let scaphoid fracture into potential complication such as non-union, delayed union, decrease of wrist joint motion, osteoarthritis of radiocarpal joint and avascular necrosis. Materials and Methods. Serial initial projection of radiograph was investigated to get the better view of scaphoid bone. Postero-anterior projection within wrist joint in extension 10°, 15°, and 20° with maximum ulnar deviation using wrist joint frame was found making the scaphoid clearer. The database was compared to get the ideal view of scaphoid. Extension and ulnar deviation were performed due to fiexed position of scaphoid anatomically in neutral wrist joint position. Results. Good exposure of scaphoid is got from performing radiographic examination of wrist joint 10° extended with maximum ulnar deviation position, in a total of 60 right and left wrist joint samples of young active men and women. Conclusions. Ten degrees extension with ulnar deviation wrist joint position can be proposed to be one of standard scaphoid view on plain radiography. -
Early Management of Upper Limb Fractures in General Practice
Bones • THEME Early management of upper limb fractures in general practice eneral practitioners are frequently confronted with BACKGROUND Upper limb injuries are very G injuries to the upper limb, most commonly from falls. David Spain, common and patients frequently present to general practitioners for treatment. Circumstances This article focusses on upper limb fractures and the MBBS, FRACGP, important issues relevant to correct early management. FACEM, is Director, of the injury and varied patient factors are critical Allamanda 24 Hour to assessment. Outcome of these injuries involves History of injury Emergency Care short term pain control and diagnosis; fracture Centre, Allamanda immobilisation, comfort and function in the A careful history should consider in detail the circum- Private Hospital, Senior Staff Specialist, treatment device medium term; and longer term, stances of the accident or fall (Table 1). This helps predict Emergency the best functional outcome. likely injury and is essential to distinguish simple slip falls Department, Gold OBJECTIVE This article aims to guide GPs from medical causes of collapse. Isolated injury must be Coast Hospital, and Clinical Senior Lecturer, through the initial assessment and early distinguished from an injury as a part of actual or potential the University of management of fractures and provides a logical, multiple trauma. Patients with a severe dramatic and Queensland. simple structure for this process. Understanding painful injury can be distracted, often resulting in other of different injury patterns and patient injuries of significance being initially overlooked. Simple characteristics to assist correct overall enquiry about other possible injury often unearths management is emphasised and the correct unusual replies. -
Upper Limb Injuries
- 1 - BCCH Emergency Department UPPER LIMB INJURIES Resource pack Developed by: RENA HEATHCOTE RN Rena Heathcote BCCH Emergency Department 2012 - 2 - FRACTURES The shoulder Dislocation +/_ fracture of humeral head History • A dislocated shoulder generally follows a fall onto their arm, or directly onto their shoulder, causing the humeral head to dislocate from the joint capsule and out of the socket. • This usually results in an anterior (towards the front) dislocation of the humeral head, where it is positioned in front of the joint socket. More rarely the humeral head dislocates posteriorly (behind) or inferiorly (underneath). Assessment • The patient usually walks in holding their arm, and in obvious pain • There is obvious deformity to the shoulder joint, noted as flattening to the top of the arm at the shoulder joint (the deltoid muscle region), and more obvious bony prominence. Obvious deformity of the shoulder, In this case, the humeral head has dislocated inferiorly Rena Heathcote BCCH Emergency Department 2012 - 3 - • The humeral head can at times be felt in the axilla • Caution: The axillary nerve can become damaged causing paralysis over the deltoid region, and the absence of sensation over a patch below the shoulder. • Sensation and radial pulse must always be checked Treatment • Remove all rings on digits to prevent swelling and neuro‐vascular compromise • Place the patients’ arm in a broad arm sling, according to the patients’ comfort • These patients should have an immediate shoulder x‐ray to exclude any underlying accompanying -
Diagnosis and Management of Scaphoid Fractures T
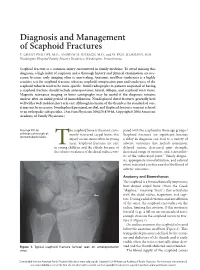
Diagnosis and Management of Scaphoid Fractures T. GRANT PHILLIPS, M.D., ANDREW M. REIBACH, M.D., and W. PAUL SLOMIANY, M.D. Washington Hospital Family Practice Residency, Washington, Pennsylvania Scaphoid fracture is a common injury encountered in family medicine. To avoid missing this diagnosis, a high index of suspicion and a thorough history and physical examination are nec- essary, because early imaging often is unrevealing. Anatomic snuffbox tenderness is a highly sensitive test for scaphoid fracture, whereas scaphoid compression pain and tenderness of the scaphoid tubercle tend to be more specific. Initial radiographs in patients suspected of having a scaphoid fracture should include anteroposterior, lateral, oblique, and scaphoid wrist views. Magnetic resonance imaging or bone scintigraphy may be useful if the diagnosis remains unclear after an initial period of immobilization. Nondisplaced distal fractures generally heal well with a well-molded short arm cast. Although inclusion of the thumb is the standard of care, it may not be necessary. Nondisplaced proximal, medial, and displaced fractures warrant referral to an orthopedic subspecialist. (Am Fam Physician 2004;70:879-84. Copyright© 2004 American Academy of Family Physicians.) See page 801 for he scaphoid bone is the most com- pared with the scaphoid in these age groups.1 definitions of strength-of- monly fractured carpal bone; this Scaphoid fractures are significant because recommendation labels. injury occurs most often in young a delay in diagnosis can lead to a variety of men. Scaphoid fractures are rare adverse outcomes that include nonunion, inT young children and the elderly because of delayed union, decreased grip strength, the relative weakness of the distal radius com- decreased range of motion, and osteoarthri- tis of the radiocarpal joint.2 Timely diagno- sis, appropriate immobilization, and referral when indicated can decrease the likelihood of adverse outcomes. -

Homologies of the Carpal Bones in Flying Squirrels (Pteromyinae): a Review
Mammal Study 26: 61-68 (2001) •. R . © the Mammalogical Society of Japan ' ,u" •XCTrc" Homologies of the carpal bones in flying squirrels (Pteromyinae): a review Richard W. Thorington, Jr.1 and Brian J. Stafford2 1 ^Department of Vertebrate Zoology, National Museum of Natural History, Smithsonian Institution, Washington, DC 20560-0108 USA 2Department of Anatomy, Howard University College of Medicine, 520 W Street, N.W., Washington, DC 20059 USA Abstract. The homologies of the carpal bones of flying squirrels, presented by Oshida et al. (2000a, b), are reviewed, together with the evidence supporting traditional homology assessments. Evidence for the homology of the styliform cartilage of flying squirrels with the hypothenar cartilage of other squirrels is also reviewed. Development, articulations, topography, and muscle insertions favor both the traditional hypothesis of homology assess- ments of the carpal bones and also the hypothesis that the styliform cartilage is homologous with the hypothenar cartilage. Key words: carpal homologies, flying squirrels, Pteromyinae, styliform cartilage. In two papers, Oshida et al. (2000a, b) described the styliform cartilage of flying squirrels and suggested that it is homologous with the pisiform bone of other mammals. This is a revolutionary interpretation of the homology of the carpus. It contrasts with the hypothe- sis of Thorington et al. (1998) that the styliform cartilage of flying squirrels is homologous with the hypothenar cartilage of other squirrels. In addition, the homology assessments of Oshida et al. (2000a, b) for all the proximal carpal bones differ fundamentally from the more traditional hypothesis followed by many authors, e.g. Hill (1937), Bryant (1945), Holmgren (1952), Grasse and Dekeyser (1955), Thorington (1984), Thorington et al. -

Diagnostic and Therapeutic Approach to Acute Scaphoid Fractures
Published online: 2020-11-24 THIEME Update Article | Artículo de Actualización 109 Diagnostic and Therapeutic Approach to Acute Scaphoid Fractures Abordaje diagnóstico y terapéutico de las fracturas agudas de escafoides Fernando Polo Simón1,2,3 Belén García Medrano1,3 Pedro J. Delgado Serrano1,3 1 Hand Surgery and Microsurgery Unit, Hospital Universitario HM Address for correspondence Fernando Polo Simón, MD, Unidad de Montepríncipe, Boadilla del Monte, Madrid, Spain Cirugía de la Mano y Microcirugía, Hospital Universitario HM 2 Mutua Universal, Madrid, Spain Montepríncipe, Boadilla del Monte, Madrid 3 Orthopedic Surgery and Traumatology Service, Hospital (e-mail: [email protected]). Universitario HM Montepríncipe, Boadilla del Monte, Madrid, Spain Rev Iberam Cir Mano 2020;48:109–118. Abstract The scaphoid is the carpal bone that most often fractures, accounting for up to 70% of carpal fractures and 11% of hand fractures. It is the second most common arm fracture, only surpassed by fractures of the distal radius. Despite being so common, these fractures can be difficult to diagnose and treat due to the anatomic and physiological particularities of the bone, including its precarious vascularization, its complex three-dimensional structure, and its ligament connections, which greatly contribute to the risk of complications such as malunion, pseudoarthrosis and avascular necrosis. Although there are many published Keywords studies on the treatment of these injuries, there is still controversy over what is the most ► scaphoid fracture suitable one for certain fracture types. The present article is a comprehensive and updated ► carpus review of the literature. Combining strategies for clinical and radiological diagnosis, we ► wrist propose a complete algorithm for the diagnosis of scaphoid fractures based on the varying ► scaphoid availability of resources, and we also describe the most appropriate therapeutic approach for ► carpal fractures the different types of acute fractures of this bone. -

Biodiversity of the Thoracic Limb Skeleton in Coypu
Scientific Works. Series C. Veterinary Medicine. Vol. LXV (2), 2019 ISSN 2065-1295; ISSN 2343-9394 (CD-ROM); ISSN 2067-3663 (Online); ISSN-L 2065-1295 BIODIVERSITY OF THE THORACIC LIMB SKELETON IN COYPU Anca ȘEICARU University of Agronomic Sciences and Veterinary Medicine of Bucharest, Faculty of Veterinary Medicine, 105, Spaiul Independenței, District 5, Bucharest, Romania Corresponding author email: [email protected] Abstract The paper presents the thoracic limb skeleton of the coypu as compared to the rabbit. The scapular girdle is represented by the scapula and the clavicle, bones that are well developed in this species. The acromion is short and tuberous. The ratio between the infraspinous and supraspinous fossae is 2/1. The deltoid tuberosity of the humerus appears evident. Contrary to existing literature, which describes the absence of the supratrochlear foramen, we identified it in two of the three investigated corpses. Between the bones of the forearm a wide interosseous space is present. The thoracic basipodium is represented by 9 carpian bones because a central bone is interposed between the proximal row and the distal row. The following bones appear in the latero-medial line of the proximal row: pisiform, scaphoid, triquetral, lunate. The latero-medial line of the distal row contains the following bones: hamate, capitate, trapezoid and trapezium. Key words: coypu, rabbit, thoracic limb skeleton. INTRODUCTION Boiling, as an alternative method of processing, was performed in water with The coypu belongs to the Animalia Kingdom, common detergents. Vertebrata Phylum, Mammalia Class, At the end of the maceration process, the bones Myocastoridae Family, coypus Species. were washed with water jet and subjected to the This study aims to bring an addition to the bleaching process with 11% hydrogen peroxide existing data in the literature.