17 Radial Styloidectomy David M
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fractures Long Bones, Upper Limb (Includes Hand)
Ministry of Defence Synopsis of Causation Fractures Long Bones, Upper Limb (includes hand) Author: Mr John A Dent, Ninewells Hospital and Medical School, Dundee Validator: Mr Sheo Tibrewal, Queen Elizabeth Hospital, London September 2008 Disclaimer This synopsis has been completed by medical practitioners. It is based on a literature search at the standard of a textbook of medicine and generalist review articles. It is not intended to be a meta-analysis of the literature on the condition specified. Every effort has been taken to ensure that the information contained in the synopsis is accurate and consistent with current knowledge and practice and to do this the synopsis has been subject to an external validation process by consultants in a relevant specialty nominated by the Royal Society of Medicine. The Ministry of Defence accepts full responsibility for the contents of this synopsis, and for any claims for loss, damage or injury arising from the use of this synopsis by the Ministry of Defence. 2 1. Definition 1.1. A bone breaks as a result of a variety of injuring forces. The fracture produced in a long bone may be of its shaft or diaphysis; towards one of its ends where the bone widens (metaphysis); or of the end of the bone, where it forms a joint with the next bone (Figure 1). Fractures near a joint may involve the joint surface causing intra-articular fractures. 1.2. It must always be remembered that the soft tissues surrounding the bone will also be damaged to a varying extent by the injuring force. -

CS-FFRA-05 – 2005-16 Super Duty Fabricated Radius Arms NOTE
Carli Suspension: 422 Jenks Circle, Corona, CA 92880 Tech Support: (714) 532-2798 CS-FFRA-05 – 2005-16 Super Duty Fabricated Radius Arms NOTE: Please review the product instructions prior to attempting installation to ensure installer is equipped with all tools and capabilities necessary to complete the product installation. We recommend thoroughly reading the instructions at least twice prior to attempting Installation. Before beginning disassembly of the vehicle, check the “What’s Included” section of the instructions to ensure you’ve received all parts necessary to complete installation. Further, verify that the parts received are PROPER TO YOUR application (year range, motor, etc.) to avoid potential down-time in correcting potential discrepancies. Any discrepancies will be handled by Carli Suspension and the correcting products will be shipped UPS Ground. LIFETIME PRODUCT WARRANTY Carli Suspension provides a limited lifetime product warranty against defects in workmanship and materials from date of purchase to the original purchaser for all products produced by Carli Suspension. Parts not manufactured by, but made to Carli Suspension’s specifications by third party manufacturers will carry a warranty through their respective manufacturer. (i.e. King Shocks, Bilstein Shocks, Fox Shocks). Deaver Leaf Spring’s warranty will be processed by Carli Suspension. Proof of purchase (from the original purchaser only) will be required to process any warranty claims. Carli Suspension products must be purchased for the listed Retail Price reflected by the price listed on the Carli Suspension Website at the time of purchase. Carli Suspension reserves the right to refuse warranty claims made by any customer refusing or unable to present proof of purchase, or presenting proof of purchase reflecting a price lower than Carli Suspension’s Retail Price at the time the item was purchased. -
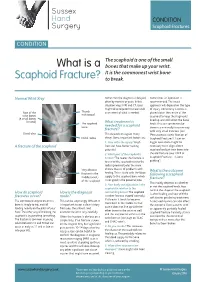
What Is a Scaphoid Fracture?
Sussex Hand CONDITION Surgery Scaphoid Fractures CONDITION The scaphoid is one of the small What is a bones that make up your wrist. It is the commonest wrist bone Scaphoid Fracture? to break. Normal Wrist Xray Sometimes the diagnosis is delayed, Sometimes an operation is often by months or years. In this recommended. The exact situation xrays, MRI and CT scans approach will depend on the type might all be required to make a full of injury. Commonly a screw is Rest of the Thumb assessment of what is needed. placed down the centre of the metacarpal wrist bones scaphoid to keep the fragments (8 small bones lined up and still whilst the bone in total) The scaphoid What treatment is heals. This can sometimes be bone needed for a scaphoid done in a minimally invasive way fracture? with very small incisions (see Distal ulna This depends on a great many ‘Percutaneous screw fixation of Distal radius things. Some important factors are: Scaphoid Fractures’). Later on 1. How old is the injury? Fresh bigger operations might be A fracture of the scaphoid fractures have better healing necessary to re-align a bent potential scaphoid and put new bone into 2. Which part of the scaphoid is the old fracture (see ‘ORIF of broken? The nearer the fracture is Scaphoid Fractures +/-bone to end of the scaphoid next to the grafting’). radius (proximal pole) the more Very obvious chance there is of problems with What is the outcome fracture in the healing. This is to do with the blood following a scaphoid middle (waist) supply to the scaphoid bone which fracture? of the scaphoid is not good in the proximal pole. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Upper Extremity Fractures
Department of Rehabilitation Services Physical Therapy Standard of Care: Distal Upper Extremity Fractures Case Type / Diagnosis: This standard applies to patients who have sustained upper extremity fractures that require stabilization either surgically or non-surgically. This includes, but is not limited to: Distal Humeral Fracture 812.4 Supracondylar Humeral Fracture 812.41 Elbow Fracture 813.83 Proximal Radius/Ulna Fracture 813.0 Radial Head Fractures 813.05 Olecranon Fracture 813.01 Radial/Ulnar shaft fractures 813.1 Distal Radius Fracture 813.42 Distal Ulna Fracture 813.82 Carpal Fracture 814.01 Metacarpal Fracture 815.0 Phalanx Fractures 816.0 Forearm/Wrist Fractures Radius fractures: • Radial head (may require a prosthesis) • Midshaft radius • Distal radius (most common) Residual deformities following radius fractures include: • Loss of radial tilt (Normal non fracture average is 22-23 degrees of radial tilt.) • Dorsal angulation (normal non fracture average palmar tilt 11-12 degrees.) • Radial shortening • Distal radioulnar (DRUJ) joint involvement • Intra-articular involvement with step-offs. Step-off of as little as 1-2 mm may increase the risk of post-traumatic arthritis. 1 Standard of Care: Distal Upper Extremity Fractures Copyright © 2007 The Brigham and Women's Hospital, Inc. Department of Rehabilitation Services. All rights reserved. Types of distal radius fracture include: • Colle’s (Dinner Fork Deformity) -- Mechanism: fall on an outstretched hand (FOOSH) with radial shortening, dorsal tilt of the distal fragment. The ulnar styloid may or may not be fractured. • Smith’s (Garden Spade Deformity) -- Mechanism: fall backward on a supinated, dorsiflexed wrist, the distal fragment displaces volarly. • Barton’s -- Mechanism: direct blow to the carpus or wrist. -

Bones Can Tell Us More Compiled By: Nancy Volk
Bones Can Tell Us More Compiled By: Nancy Volk Strong Bones Sometimes only a few bones are found in a location in an archeological dig. VOCABULARY A few bones can tell about the height of a person. This is possible due to the Femur ratios of the bones. It has been determined that there are relationships between the femur, tibia, humerus, and radius and a person’s height. Humerus Radius Here is a little help to identify these four bones and formulas to assist with Tibia determining the height of a person based on bone length. Humerus Femur: Humerus: The thigh is the region of the femur. The arm bone most people call the From the hip bone to the knee bone. upper arm. It is found from the elbow to the shoulder joints. Inside This Packet Radius Strong Bones 1 New York State Standards 1 Activity: Bone Relationships 2 Information for the Teacher 4 Tibia: Radius: The larger and stronger of the two bones The bone found in the forearm that New York State Standards in the leg below the knee bone. extends from the side of the elbow to Middle School In vertebrates It is recognized as the the wrist. Standard 4: Living Environment strongest weight bearing bone in the Idea 1: 1.2a, 1.2b, 1.2e, 1.2f body. Life Sciences - Post Module 3 Middle School Page 1 Activity: Bone Relationships MATERIALS NEEDED Skeleton Formulas: Tape Measure Bone relationship is represented by the following formulas: Directions and formulas P represents the person’s height. The last letter of each formula stands for the Calculator known length of the bone (femur, tibia, humerus, or radius) through measurement. -

The Differential Diagnosis of Bone Marrow Edema on Wrist MRI
Skeletal Radiology (2019) 48:1525–1539 https://doi.org/10.1007/s00256-019-03204-1 REVIEW ARTICLE Review article: the differential diagnosis of bone marrow edema on wrist MRI WanYin Lim1,2 & Asif Saifuddin3,4 Received: 5 December 2018 /Revised: 1 February 2019 /Accepted: 5 March 2019 /Published online: 22 March 2019 # ISS 2019 Abstract There is a large variety of conditions that can result in ‘bone marrow edema’ or ‘bone marrow lesions’ (BML) in the wrist on magnetic resonance imaging (MRI). The combination of clinical history and the distribution of the BML can serve as a valuable clue to a specific diagnosis. This article illustrates the different patterns of BML in the wrist to serve as a useful guide when reviewing wrist MRI studies. Imaging artefacts will also be briefly covered. Keywords MRI . Wrist . Marrow edema . Bone marrow lesion Introduction The etiology of BMLs can also be confusing due to the non-specific appearance, MRI demonstrating poorly defined Bone marrow lesions (BML), or marrow signal reduced T1-weighted spin echo (T1W SE) marrow signal in- hyperintensity on fluid-sensitive magnetic resonance im- tensity (SI) (Fig. 1a) with corresponding hyperintensity on aging (MRI) sequences, are observed in up to 36% of short tau inversion recovery (STIR), fat-suppressed T2W fast patients undergoing wrist MRI [1]. With regard to def- spin echo (FS T2W FSE), and fat-suppressed proton density- inition, the term ‘bone marrow lesion’ (BML) used in weighted fast spin echo (FS PDW FSE) sequences (Fig. 1b). this manuscript is synonymous with ‘edema-like marrow There may also be overlapping patterns between different en- signal’, ‘marrow edema-like signal’ or ‘bone marrow tities, but the combination of clinical history and lesion loca- edema pattern’ [2]. -

Distal Radius Fracture
Distal Radius Fracture Osteoporosis, a common condition where bones become brittle, increases the risk of a wrist fracture if you fall. How are distal radius fractures diagnosed? Your provider will take a detailed health history and perform a physical evaluation. X-rays will be taken to confirm a fracture and help determine a treatment plan. Sometimes an MRI or CT scan is needed to get better detail of the fracture or to look for associated What is a distal radius fracture? injuries to soft tissues such as ligaments or Distal radius fracture is the medical term for tendons. a “broken wrist.” To fracture a bone means it is broken. A distal radius fracture occurs What is the treatment for distal when a sudden force causes the radius bone, radius fracture? located on the thumb side of the wrist, to break. The wrist joint includes many bones Treatment depends on the severity of your and joints. The most commonly broken bone fracture. Many factors influence treatment in the wrist is the radius bone. – whether the fracture is displaced or non-displaced, stable or unstable. Other Fractures may be closed or open considerations include age, overall health, (compound). An open fracture means a bone hand dominance, work and leisure activities, fragment has broken through the skin. There prior injuries, arthritis, and any other injuries is a risk of infection with an open fracture. associated with the fracture. Your provider will help determine the best treatment plan What causes a distal radius for your specific injury. fracture? Signs and Symptoms The most common cause of distal radius fracture is a fall onto an outstretched hand, • Swelling and/or bruising at the wrist from either slipping or tripping. -

Conservative Vs. Surgical Management of Ulnar Styloid Fractures Associated with Distal Radius Fractures
CLINICAL RESEARCH Conservative vs. surgical management of ulnar styloid fractures associated with distal radius fractures Cristian Robles, Santiago Iglesias, Christian Allende Nores, Pablo Rotella, Martín Caloia, Miguel Capomassi Orthopedics and Traumatology Department, Sanatorio Allende (Córdoba, Argentina) ABSTRACT Objectives: To evaluate potential differences in clinical and radiological outcomes after surgical versus conservative management of ulnar styloid fractures associated with unstable distal radius fractures treated by locked volar plating. Materials and Methods: This was a multicenter, retrospective and descriptive study including surgical patients treated at four different institutions between 2009 and 2012 for ulnar styloid fractures associated with unstable distal radius fractures. Ulnar styloid fractures were treated con- servatively in group I and surgically in group II. Results: The average follow-up was 56 months. The study included 57 patients divided into two groups (group I [29 cases] and group II [28 cases]). Patients in group II had 2.76 times (95% CI: 1.086; 8.80) more chances of achieving bone union than those in group I. DASH and pain scores, both at rest and during activity, did not show significant differences between the two groups (p = 0.276 and p = 0.877). Group I presented milder ulnar deviation and better strength (p = 0.0194 and p = 0.024). Conclusions: Although patients who underwent surgery for ulnar styloid fractures had 2.76 more chances of achieving bone union than those who received conservative management, there were no significant differences between both groups in subjective evaluations (DASH and pain scores) or when considering the degree of ulnar styloid involve- ment. However, the parameters of strength and ulnar deviation were better in the conservative management group. -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -

The Anatomy of the Bicipital Tuberosity and Distal Biceps Tendon
The anatomy of the bicipital tuberosity and distal biceps tendon Augustus D. Mazzocca, MD,a Mark Cohen, MD,b Eric Berkson, MD,b Gregory Nicholson, MD,b Bradley C. Carofino, MD,a Robert Arciero, MD,a and Anthony A. Romeo, MDb Farmington, CT, and Chicago, IL The anatomy of the distal biceps tendon and bicipi- and the mean BT-radial styloid angle is 123° Ϯ 10°. tal tuberosity (BT) is important in the pathophysiol- None of the measurements correlated with patient ogy of tendon rupture, as well as surgical repair. age, sex, or race. We concluded that the morphology Understanding the dimensions of the BT and its an- of the BT ridge is variable. The insertion footprint of gular relationship to the radial head and radial the distal biceps tendon is on the ulnar aspect of the styloid will facilitate surgical procedures such as re- BT ridge. The dimensions of the radius and BT are ap- construction of the distal biceps tendon, radial head plicable to several surgical procedures about the el- prosthesis implantation, and reconstruction of proxi- bow. (J Shoulder Elbow Surg 2007;16:122-127.) mal radius trauma. We examined 178 dried cadav- eric radii, and the following measurements were col- The recognition and treatment of distal biceps ten- lected: radial length, length and width of the BT, don ruptures have increased over time. Previously, diameter of the radius just distal to the BT, distance this injury was considered rare; only 65 cases were from the radial head to the BT, radial head diame- reported before 1941.2,4 However, a more recent ter, width of the radius at the BT, radial neck-shaft retrospective study identified the incidence to be 1.2 10 angle, and styloid angle.