Upper Limb Injuries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Wrist Fracture – Advice Following Removal of Your Cast
Wrist Fracture – advice following removal of your cast A plaster cast usually prevents a fracture from moving, but allows your fingers to move. The cast also reduces pain. What to expect It usually takes four to six weeks for new bone to form to heal your fracture. When the cast is removed most people find that their wrist is stiff, weak and uncomfortable to start with. It may also be prone to swelling and the skin dry or flaky, this is quite normal. It is normal to get some pain after your fracture. If you need painkillers you should take them as prescribed as this will allow you to do your exercises and use your wrist for light activities. You can ask a Pharmacist about over the counter painkillers. If your pain is severe, continuous or excessive you should contact your GP. The new bone gradually matures and becomes stronger over the next few months. It is likely to be tender and may hurt if you bang it. The muscles will be weak initially, but they should gradually build up as you start to use your hand and wrist. When can I start to use my hand and wrist? It is important to try and use your hand and wrist as normally as possible. Start with light activities like fastening buttons, washing your face, eating, turning the pages of books over etc. Build up as pain allows. Avoid lifting a kettle for 4 weeks If I have been given a Wrist splint You may have been given a wrist splint to wear. -

Fractures Long Bones, Upper Limb (Includes Hand)
Ministry of Defence Synopsis of Causation Fractures Long Bones, Upper Limb (includes hand) Author: Mr John A Dent, Ninewells Hospital and Medical School, Dundee Validator: Mr Sheo Tibrewal, Queen Elizabeth Hospital, London September 2008 Disclaimer This synopsis has been completed by medical practitioners. It is based on a literature search at the standard of a textbook of medicine and generalist review articles. It is not intended to be a meta-analysis of the literature on the condition specified. Every effort has been taken to ensure that the information contained in the synopsis is accurate and consistent with current knowledge and practice and to do this the synopsis has been subject to an external validation process by consultants in a relevant specialty nominated by the Royal Society of Medicine. The Ministry of Defence accepts full responsibility for the contents of this synopsis, and for any claims for loss, damage or injury arising from the use of this synopsis by the Ministry of Defence. 2 1. Definition 1.1. A bone breaks as a result of a variety of injuring forces. The fracture produced in a long bone may be of its shaft or diaphysis; towards one of its ends where the bone widens (metaphysis); or of the end of the bone, where it forms a joint with the next bone (Figure 1). Fractures near a joint may involve the joint surface causing intra-articular fractures. 1.2. It must always be remembered that the soft tissues surrounding the bone will also be damaged to a varying extent by the injuring force. -
What Is a Scaphoid Fracture?
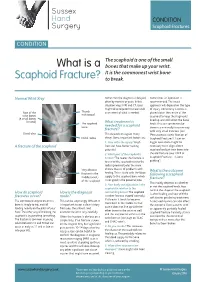
Sussex Hand CONDITION Surgery Scaphoid Fractures CONDITION The scaphoid is one of the small What is a bones that make up your wrist. It is the commonest wrist bone Scaphoid Fracture? to break. Normal Wrist Xray Sometimes the diagnosis is delayed, Sometimes an operation is often by months or years. In this recommended. The exact situation xrays, MRI and CT scans approach will depend on the type might all be required to make a full of injury. Commonly a screw is Rest of the Thumb assessment of what is needed. placed down the centre of the metacarpal wrist bones scaphoid to keep the fragments (8 small bones lined up and still whilst the bone in total) The scaphoid What treatment is heals. This can sometimes be bone needed for a scaphoid done in a minimally invasive way fracture? with very small incisions (see Distal ulna This depends on a great many ‘Percutaneous screw fixation of Distal radius things. Some important factors are: Scaphoid Fractures’). Later on 1. How old is the injury? Fresh bigger operations might be A fracture of the scaphoid fractures have better healing necessary to re-align a bent potential scaphoid and put new bone into 2. Which part of the scaphoid is the old fracture (see ‘ORIF of broken? The nearer the fracture is Scaphoid Fractures +/-bone to end of the scaphoid next to the grafting’). radius (proximal pole) the more Very obvious chance there is of problems with What is the outcome fracture in the healing. This is to do with the blood following a scaphoid middle (waist) supply to the scaphoid bone which fracture? of the scaphoid is not good in the proximal pole. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

PE1897 Wrist and Hand Stretches
Patient and Family Education Wrist and Hand Stretches How can I help my child do the stretches? Use these exercises to help stretch the You play an important role in your child’s therapy. Older children may need wrist and hand. reminders to do their stretches every day. You may need to help position your younger child for the stretches. Or you may need to help stretch your child’s hand or arm. Be sure to pay attention to your child’s alignment and posture to make sure each stretch is performed correctly. How often should my child do the stretches? These stretches should be done twice a day, or as instructed by your therapist: ______________________________________________________________ Stretches Wrist extension Hold arm out in front Use opposite hand to bend wrist up with fingers straight Option to straighten elbow for increased stretch Hold for 30 seconds or _______ Repeat 2 times or ___________ VHI Wrist extension Sit with elbows on table Place palms together Slowly lower wrists to table Hold for 30 seconds or ______ Repeat 2 times or __________ VHI Wrist flexion Hold arm out in front Use opposite hand to bend wrist down Option to straighten elbow for increased stretch Option to curl fingers for increased stretch Hold for 30 seconds or ______ VHI Repeat 2 times or __________ 1 of 2 Wrist and Hand Stretches Wrist radial/ulnar deviation To Learn More Hold arm at side of body with palm • Occupational/Physical facing forward Therapy 206-987-2113 Use opposite hand to straighten wrist toward the thumb side Do not allow the wrist to flex forward to extend backward Free Interpreter Hold for 30 seconds or ______ Services Repeat 2 times or __________ • In the hospital, ask BioEx Systems Inc.* your child’s nurse. -

Hand, Elbow, Wrist Pain
Physical and Sports Therapy Hand, Elbow, Wrist Pain The hand is a wondrously complex structure of tiny bones, muscles, ligaments, and tendons which work together to perform tasks. The wrist and elbow are stabilizing joints that support the steady use of the hand and provide attachment points for the muscles that control the hand and wrist. All three of these areas are prone to injury from overuse or trauma. Their complexity requires the skills of an expert for proper rehabilitation from injury. Some Hand, Wrist, and Elbow Issues Include: Tennis/Golfer’s Elbow: Tendonitis, or inflammation of the tendons, at the muscular attachments near the elbow. Symptoms typically include tenderness on the sides of the elbow, which increase with use of the wrist and hand, such as shaking hands or picking up a gallon of milk. Tendonitis responds well to therapy, using eccentric exercise, stretching, and various manual therapy techniques. Carpal Tunnel Syndrome: Compression of the Median Nerve at the hand/base of your wrist. Symptoms include pain, numbness, and tingling of the first three fingers. The condition is well-known for waking people at night. Research supports the use of therapy, particularly in the early phase, for alleviation of the compression through stretching and activity modification. Research indicates that the longer symptoms are present before initiating treatment, the worse the outcome for therapy and surgical intervention due to underlying physiological changes of the nerve. What can Physical or Occupational therapy do for Hand, Wrist, or Elbow pain? Hand, wrist, and elbow injuries are commonly caused by trauma, such as a fall or overuse. -

EM Cases Digest Vol. 1 MSK & Trauma
THE MAGAZINE SERIES FOR ENHANCED EM LEARNING Vol. 1: MSK & Trauma Copyright © 2015 by Medicine Cases Emergency Medicine Cases by Medicine Cases is copyrighted as “All Rights Reserved”. This eBook is Creative Commons Attribution-NonCommercial- NoDerivatives 3.0 Unsupported License. Upon written request, however, we may be able to share our content with you for free in exchange for analytic data. For permission requests, write to the publisher, addressed “Attention: Permissions Coordinator,” at the address below. Medicine Cases 216 Balmoral Ave Toronto, ON, M4V 1J9 www.emergencymedicinecases.com This book has been authored with care to reflect generally accepted practices. As medicine is a rapidly changing field, new diagnostic and treatment modalities are likely to arise. It is the responsibility of the treating physician, relying on his/her experience and the knowledge of the patient, to determine the best management plan for each patient. The author(s) and publisher of this book are not responsible for errors or omissions or for any consequences from the application of the information in this book and disclaim any liability in connection with the use of this information. This book makes no guarantee with respect to the completeness or accuracy of the contents within. OUR THANKS TO... EDITORS IN CHIEF Anton Helman Taryn Lloyd PRODUCTION EDITOR Michelle Yee PRODUCTION MANAGER Garron Helman CHAPTER EDITORS Niran Argintaru Michael Misch PODCAST SUMMARY EDITORS Lucas Chartier Keerat Grewal Claire Heslop Michael Kilian PODCAST GUEST EXPERTS Andrew Arcand Natalie Mamen Brian Steinhart Mike Brzozowski Hossein Mehdian Arun Sayal Ivy Cheng Sanjay Mehta Laura Tate Walter Himmel Jonathan Pirie Rahim Valani Dave MacKinnon Jennifer Riley University of Toronto, Faculty of Medicine EM Cases is a venture of the Schwartz/ Reisman Emergency Medicine Institute. -

Pediatric Orthopedic Injuries… … from an ED State of Mind
Traumatic Orthopedics Peds RC Exam Review February 28, 2019 Dr. Naminder Sandhu, FRCPC Pediatric Emergency Medicine Objectives to cover today • Normal bone growth and function • Common radiographic abnormalities in MSK diseases • Part 1: Atraumatic – Congenital abnormalities – Joint and limb pain – Joint deformities – MSK infections – Bone tumors – Common gait disorders • Part 2: Traumatic – Common pediatric fractures and soft tissue injuries by site Overview of traumatic MSK pain Acute injuries • Fractures • Joint dislocations – Most common in ED: patella, digits, shoulder, elbow • Muscle strains – Eg. groin/adductors • Ligament sprains – Eg. Ankle, ACL/MCL, acromioclavicular joint separation Chronic/ overuse injuries • Stress fractures • Tendonitis • Bursitis • Fasciitis • Apophysitis Overuse injuries in the athlete WHY do they happen?? Extrinsic factors: • Errors in training • Inappropriate footwear Overuse injuries Intrinsic: • Poor conditioning – increased injuries early in season • Muscle imbalances – Weak muscle near strong (vastus medialus vs lateralus patellofemoral pain) – Excessive tightness: IT band, gastroc/soleus Sever disease • Anatomic misalignments – eg. pes planus, genu valgum or varum • Growth – strength and flexibility imbalances • Nutrition – eg. female athlete triad Misalignment – an intrinsic factor Apophysitis • *Apophysis = natural protruberance from a bone (2ndary ossification centres, often where tendons attach) • Examples – Sever disease (Calcaneal) – Osgood Schlatter disease (Tibial tubercle) – Sinding-Larsen-Johansson -

Stretching and Positioning Regime for Upper Limb
Information for patients and visitors Stretching and Positioning Regime for Upper Limb Physiotherapy Department This leaflet has been designed to remind you of the exercises you Community & Therapy Services have been taught, the correct techniques and who to contact with any queries. For more information about our Trust and the services we provide please visit our website: www.nlg.nhs.uk Information for patients and visitors Muscle Tone Muscle tone is an unconscious low level contraction of your muscles while they are at rest. The purpose of this is to keep your muscles primed and ready to generate movement. Several neurological causes may change a person’s muscle tone to increase or decrease resulting in a lack of movement. Over time, a lack of movement can cause stiffness, pain, and spasticity. In severe cases this may also lead to contractures. Spasticity Spasticity can be defined as a tightening or stiffness of the muscle due to increased muscle tone. It can interfere with normal functioning. It can also greatly increase fatigue. However, exercise, properly done, is vital in managing spasticity. The following tips may prove helpful: • Avoid positions that make the spasticity worse • Daily stretching of muscles to their full length will help to manage the tightness of spasticity, and allow for optimal movement • Moving a tight muscle to a new position may result in an increase in spasticity. If this happens, allow a few minutes for the muscles to relax • When exercising, try to keep head straight • Sudden changes in spasticity may -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Design of a Working Model of an Upper Limb Prosthesis: Wrist Mechanism
DESIGN OF A WORKING MODEL OF AN UPPER LIMB PROSTHESIS: WRIST MECHANISM BY SAHIL VIKAS DANGE A thesis submitted to the Graduate School|New Brunswick Rutgers, The State University of New Jersey in partial fulfillment of the requirements for the degree of Master of Science Graduate Program in Mechanical and Aerospace Engineering Written under the direction of Professor William Craelius and Professor Noshir A. Langrana and approved by New Brunswick, New Jersey October, 2017 ABSTRACT OF THE THESIS Design of a working model of an upper limb prosthesis: Wrist Mechanism by Sahil Vikas Dange Thesis Directors: Professor William Craelius and Professor Noshir A. Langrana This thesis demonstrates a new design for an upper limb prosthetic wrist that gives 3 independent degrees of freedom (DOFs) through individual mechanisms. A human wrist has 3 degrees of freedom i.e. Flexion-Extension, Radial- Ulnar deviation and Pronation-Supination. The upper limb prostheses that are currently available in the market generally provide 1 (usually Pronation- Supination) or at most 2 degrees of freedom, which is not sufficient for daily life. For this thesis, a new wrist having all the 3 DOFs was designed in the SolidWorks software, a prototype was 3D printed and a basic analysis of the mechanical properties of the model through SolidWorks simulation was carried out. The prototype mechanisms were then connected to servo motors, with potentiometers as their inputs, that were programmed through an arduino and were tested to see if they work as expected. Faithful recreation of the wrist motions was achieved and the range of motion (ROM) of this prosthesis was similar to the ROM of an actual human wrist. -

Human Functional Anatomy 213 Upper & Lower Limbs Compared
Human Functional Anatomy 213 week 6 1 Human Functional Anatomy 213 week 6 2 HUMAN FUNCTIONAL ANATOMY 213 DORSAL and VENTRAL, UPPER & LOWER LIMBS COMPARED PREAXIAL and POSTAXIAL THIS WEEKS LAB: Limbs evolved from paddles or fins, each with The hand and Foot 1. Dorsal and ventral sides 2. Preaxial and postaxial edges. In this lecture During Dorsal and ventral, Preaxial and postaxial development, Similarities in structure – Homology? human limbs were 1. Bones the same, but 2. Muscles rotations and 3. Nerves differential Muscles of the Shoulder and Hip/Arm and Thigh growth have The hand and foot modified the Muscles of the leg/foot and forearm/hand overall shape. The preaxial border is closer to the head and therefore supplied by more cranial nerves. We can identify the preaxial and postaxial borders in adult limbs by the first and fifth digits of the hand and foot Veins and nerves Human Functional Anatomy 213 week 6 3 Human Functional Anatomy 213 week 6 4 Similarities in structure - Homology PROXIMAL MUSCLES IN THE UPPER AND LOWER LIMBS Bones and joints Shoulder & Hip – Ball and socket joints Shoulder and arm Hip and thigh Humerus & Femur – Single bone in the proximal segment. Triceps Quadruceps etc Radial nerve Femoral nerve Knee & Elbow – hinge/uniaxial joints. Biceps etc Hamstrings Leg & Forearm – Two bones in the distal segment Musculocutaneous nerve Tibial nerve Tibia & Radius – Preaxial bones. Fibula & ulna – Postaxial bones Deltoid plus Gluteals & TFL posterior axillary muscles plus 6 lateral rotators Axillary nerve and post cord Gluteal nerves Ankle & Wrist – tarsals & carpals Even in the Pectorals Adductors hand and foot we Pectoral nerves Obturator nerve can find homologies between the carpal and tarsal bones.