Bones of the Upper Limbs Anatomy Team 434
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Body Mechanics As the Rotator Cuff Gether in a Cuff-Shape Across the Greater and Lesser Tubercles the on Head of the Humerus
EXPerT CONTENT Body Mechanics by Joseph E. Muscolino | Artwork Giovanni Rimasti | Photography Yanik Chauvin Rotator Cuff Injury www.amtamassage.org/mtj WORKING WITH CLieNTS AFFecTED BY THIS COmmON CONDITION ROTATOR CUFF GROUP as the rotator cuff group because their distal tendons blend and attach to- The four rotator cuff muscles are gether in a cuff-shape across the greater and lesser tubercles on the head of the supraspinatus, infraspinatus, the humerus. Although all four rotator cuff muscles have specific concen- teres minor, and subscapularis (Fig- tric mover actions at the glenohumeral (GH) joint, their primary functional ure 1). These muscles are described importance is to contract isometrically for GH joint stabilization. Because 17 Before practicing any new modality or technique, check with your state’s or province’s massage therapy regulatory authority to ensure that it is within the defined scope of practice for massage therapy. the rotator cuff group has both mover and stabilization roles, it is extremely functionally active and therefore often physically stressed and injured. In fact, after neck and low back conditions, the shoulder is the most com- Supraspinatus monly injured joint of the human body. ROTATOR CUFF PATHOLOGY The three most common types of rotator cuff pathology are tendinitis, tendinosus, and tearing. Excessive physi- cal stress placed on the rotator cuff tendon can cause ir- ritation and inflammation of the tendon, in other words, tendinitis. If the physical stress is chronic, the inflam- matory process often subsides and degeneration of the fascial tendinous tissue occurs; this is referred to as tendinosus. The degeneration of tendinosus results in weakness of the tendon’s structure, and with continued Teres minor physical stress, whether it is overuse microtrauma or a macrotrauma, a rotator cuff tendon tear might occur. -

Fractures Long Bones, Upper Limb (Includes Hand)
Ministry of Defence Synopsis of Causation Fractures Long Bones, Upper Limb (includes hand) Author: Mr John A Dent, Ninewells Hospital and Medical School, Dundee Validator: Mr Sheo Tibrewal, Queen Elizabeth Hospital, London September 2008 Disclaimer This synopsis has been completed by medical practitioners. It is based on a literature search at the standard of a textbook of medicine and generalist review articles. It is not intended to be a meta-analysis of the literature on the condition specified. Every effort has been taken to ensure that the information contained in the synopsis is accurate and consistent with current knowledge and practice and to do this the synopsis has been subject to an external validation process by consultants in a relevant specialty nominated by the Royal Society of Medicine. The Ministry of Defence accepts full responsibility for the contents of this synopsis, and for any claims for loss, damage or injury arising from the use of this synopsis by the Ministry of Defence. 2 1. Definition 1.1. A bone breaks as a result of a variety of injuring forces. The fracture produced in a long bone may be of its shaft or diaphysis; towards one of its ends where the bone widens (metaphysis); or of the end of the bone, where it forms a joint with the next bone (Figure 1). Fractures near a joint may involve the joint surface causing intra-articular fractures. 1.2. It must always be remembered that the soft tissues surrounding the bone will also be damaged to a varying extent by the injuring force. -

Should Joint Presentation File
6/5/2017 The Shoulder Joint Bones of the shoulder joint • Scapula – Glenoid Fossa Infraspinatus fossa – Supraspinatus fossa Subscapular fossa – Spine Coracoid process – Acromion process • Clavicle • Humerus – Greater tubercle Lesser tubercle – Intertubercular goove Deltoid tuberosity – Head of Humerus Shoulder Joint • Bones: – humerus – scapula Shoulder Girdle – clavicle • Articulation – glenohumeral joint • Glenoid fossa of the scapula (less curved) • head of the humerus • enarthrodial (ball and socket) 1 6/5/2017 Shoulder Joint • Connective tissue – glenoid labrum: cartilaginous ring, surrounds glenoid fossa • increases contact area between head of humerus and glenoid fossa. • increases joint stability – Glenohumeral ligaments: reinforce the glenohumeral joint capsule • superior, middle, inferior (anterior side of joint) – coracohumeral ligament (superior) • Muscles play a crucial role in maintaining glenohumeral joint stability. Movements of the Shoulder Joint • Arm abduction, adduction about the shoulder • Arm flexion, extension • Arm hyperflexion, hyperextension • Arm horizontal adduction (flexion) • Arm horizontal abduction (extension) • Arm external and internal rotation – medial and lateral rotation • Arm circumduction – flexion, abduction, extension, hyperextension, adduction Scapulohumeral rhythm • Shoulder Joint • Shoulder Girdle – abduction – upward rotation – adduction – downward rotation – flexion – elevation/upward rot. – extension – Depression/downward rot. – internal rotation – Abduction (protraction) – external rotation -

Suprascapular Nerve Lesions at the Spinoglenoid Notch: Report of Three Cases and Review of the Literature 243
Journal ofNeurology, Neurosurgery, and Psychiatry 1991;54:241-243 241 Suprascapular nerve lesions at the spinoglenoid J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.54.3.241 on 1 March 1991. Downloaded from notch: report of three cases and review of the literature Jay A Liveson, Michael J Bronson, Michael A Pollack Abstract of root involvement (cervical pain, and change Lesions of the suprascapular nerve can from Valsalva's manoeuvre). His past medical occur at the supraspinatus notch (SSN) history was negative. On physical examination or at the spinoglenoid notch (SGN). Elec- cranial nerves were normal. No weakness was tromyographic (EMG), evaluation of the detected on careful manual muscle examin- infraspinatus, and especially the supra- ation. Sensation was intact. Deep tendon spinatus muscles distinguishes SGN reflexes were active and symmetrical with no from SSN lesions. Three cases of SGN pathological reflexes. There was no Homer's lesions, which are more common than sign. SSN lesions, are presented. The patient gave up weight lifting and started a programme of physiotherapy. His shoulder ache resolved rapidly, but his muscle Entrapment of the suprascapular nerve at the bulk did not return to normal for another 12 suprascapular notch (SSN) was first described months. He reported completely normal func- in 1963 by Kopell and Thompson.' No alter- tion. native entrapment site was recognised until 1981 when the first case of spinoglenoid notch Case 2 (SGN) entrapmnt was described by Ganzhorn A 22 year old right handed male was skeet et al.2 Since then nine additional cases of SGN shooting, a month before his examination. -

Scapular Motion Tracking Using Acromion Skin Marker Cluster: in Vitro Accuracy Assessment
Scapular Motion Tracking Using Acromion Skin Marker Cluster: In Vitro Accuracy Assessment Andrea Cereatti, Claudio Rosso, Ara Nazarian, Joseph P. DeAngelis, Arun J. Ramappa & Ugo Della Croce Journal of Medical and Biological Engineering ISSN 1609-0985 J. Med. Biol. Eng. DOI 10.1007/s40846-015-0010-2 1 23 Your article is protected by copyright and all rights are held exclusively by Taiwanese Society of Biomedical Engineering. This e- offprint is for personal use only and shall not be self-archived in electronic repositories. If you wish to self-archive your article, please use the accepted manuscript version for posting on your own website. You may further deposit the accepted manuscript version in any repository, provided it is only made publicly available 12 months after official publication or later and provided acknowledgement is given to the original source of publication and a link is inserted to the published article on Springer's website. The link must be accompanied by the following text: "The final publication is available at link.springer.com”. 1 23 Author's personal copy J. Med. Biol. Eng. DOI 10.1007/s40846-015-0010-2 ORIGINAL ARTICLE Scapular Motion Tracking Using Acromion Skin Marker Cluster: In Vitro Accuracy Assessment Andrea Cereatti • Claudio Rosso • Ara Nazarian • Joseph P. DeAngelis • Arun J. Ramappa • Ugo Della Croce Received: 11 October 2013 / Accepted: 20 March 2014 Ó Taiwanese Society of Biomedical Engineering 2015 Abstract Several studies have recently investigated how estimated using an AMC combined with a single anatom- the implementations of acromion marker clusters (AMCs) ical calibration, the accuracy was highly dependent on the method and stereo-photogrammetry affect the estimates of specimen and the type of motion (maximum errors between scapula kinematics. -

Spontaneous Fracture of the Scapula Spines in Association with Severe Rotator Cuff Disease and Osteoporosis
Central Annals of Musculoskeletal Disorders Case Report *Corresponding author Hans Van der Wall, CNI Molecular Imaging & University of Notre Dame, Sydney, Australia, Tel: +61 2 9736 1040; Spontaneous Fracture of the FAX: +61 2 9736 2095; Email: [email protected] Submitted: 25 March 2020 Scapula Spines in Association Accepted: 07 April 2020 Published: 10 April 2020 ISSN: 2578-3599 with Severe Rotator Cuff Copyright © 2020 Robert B, et al. Disease and Osteoporosis OPEN ACCESS 1 2 3 Breit Robert , Strokon Andrew , Burton Leticia , Van der Wall Keywords H3* and Bruce Warwick3 • Scapular fracture • Rotator cuff arthropathy 1CNI Molecular Imaging, Australia • Osteoporosis 2Sydney Private Hospital, Australia • Scintigraphy 3CNI Molecular Imaging & University of Notre Dame, Sydney, Australia • SPECT/ CT 4Concord Hospital, Australia Abstract We present the case of a 74 year-old woman with diabetes mellitus and established osteoporosis who initially presented with increasing pain and disability of the shoulders. Investigations showed severe rotator cuff disease. This was treated conservatively with physiotherapy and corticosteroid injection into both joints with good pain relief but no improvement in function. She subsequently presented with increasing posterior thoracic pain with plain films reporting no evidence of rib fracture. Bone scintigraphy showed severe rotator cuff disease and degenerative joint disease at multiple sites. The single photon emission computed tomography (SPECT)/ x-ray Computed Tomography (CT) showed bilateral scapula spine fractures of long standing with a probable non-union on the left side. These fractures are rare and difficult to treat when associated with rotator cuff disease. INTRODUCTION Fractures of the scapula spine are rare, with a reported level of dysfunction remained significant with marked restriction frequency of less than twenty cases in the literature [1-8]. -
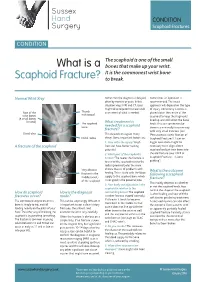
What Is a Scaphoid Fracture?
Sussex Hand CONDITION Surgery Scaphoid Fractures CONDITION The scaphoid is one of the small What is a bones that make up your wrist. It is the commonest wrist bone Scaphoid Fracture? to break. Normal Wrist Xray Sometimes the diagnosis is delayed, Sometimes an operation is often by months or years. In this recommended. The exact situation xrays, MRI and CT scans approach will depend on the type might all be required to make a full of injury. Commonly a screw is Rest of the Thumb assessment of what is needed. placed down the centre of the metacarpal wrist bones scaphoid to keep the fragments (8 small bones lined up and still whilst the bone in total) The scaphoid What treatment is heals. This can sometimes be bone needed for a scaphoid done in a minimally invasive way fracture? with very small incisions (see Distal ulna This depends on a great many ‘Percutaneous screw fixation of Distal radius things. Some important factors are: Scaphoid Fractures’). Later on 1. How old is the injury? Fresh bigger operations might be A fracture of the scaphoid fractures have better healing necessary to re-align a bent potential scaphoid and put new bone into 2. Which part of the scaphoid is the old fracture (see ‘ORIF of broken? The nearer the fracture is Scaphoid Fractures +/-bone to end of the scaphoid next to the grafting’). radius (proximal pole) the more Very obvious chance there is of problems with What is the outcome fracture in the healing. This is to do with the blood following a scaphoid middle (waist) supply to the scaphoid bone which fracture? of the scaphoid is not good in the proximal pole. -

Arthroscopic Decompression of the Suprascapular Nerve at the Spinoglenoid Notch and Suprascapular Notch Through the Subacromial Space
Technical Note Arthroscopic Decompression of the Suprascapular Nerve at the Spinoglenoid Notch and Suprascapular Notch Through the Subacromial Space Neil Ghodadra, M.D., Shane J. Nho, M.D., M.S., Nikhil N. Verma, M.D., Stefanie Reiff, B.A., Dana P. Piasecki, M.D., Matthew T. Provencher, M.D., and Anthony A. Romeo, M.D. Abstract: Suprascapular nerve entrapment can cause disabling shoulder pain. Suprascapular nerve release is often performed for compression neuropathy and to release pressure on the nerve associated with arthroscopic labral repair. This report describes a novel all-arthroscopic technique for decom- pression of the suprascapular nerve at the suprascapular notch or spinoglenoid notch through a subacromial approach. Through the subacromial space, spinoglenoid notch cysts can be visualized between the supraspinatus and infraspinatus at the base of the scapular spine. While viewing the subacromial space through the lateral portal, the surgeon can use a shaver through the posterior portal to decompress a spinoglenoid notch cyst at the base of the scapular spine. To decompress the suprascapular nerve at the suprascapular notch, a shaver through the posterior portal removes the soft tissue on the acromion and distal clavicle to expose the coracoclavicular ligaments. The medial border of the conoid ligament is identified and followed to its coracoid attachment. The supraspinatus muscle is retracted with a blunt trocar placed through an accessory Neviaser portal. The transverse scapular ligament, which courses inferior to the suprascapular artery, is sectioned with arthroscopic scissors, and the suprascapular nerve is decompressed. Key Words: Arthroscopy—Suprascapular nerve—Transverse scapular ligament—Suprascapular notch—Rotator cuff—Shoulder. -

Altered Alignment of the Shoulder Girdle and Cervical Spine in Patients with Insidious Onset Neck Pain and Whiplash- Associated Disorder
Journal of Applied Biomechanics, 2011, 27, 181-191 © 2011 Human Kinetics, Inc. Altered Alignment of the Shoulder Girdle and Cervical Spine in Patients With Insidious Onset Neck Pain and Whiplash- Associated Disorder Harpa Helgadottir, Eythor Kristjansson, Sarah Mottram, Andrew Karduna, and Halldor Jonsson, Jr. Clinical theory suggests that altered alignment of the shoulder girdle has the potential to create or sustain symptomatic mechanical dysfunction in the cervical and thoracic spine. The alignment of the shoulder girdle is described by two clavicle rotations, i.e, elevation and retraction, and by three scapular rotations, i.e., upward rotation, internal rotation, and anterior tilt. Elevation and retraction have until now been assessed only in patients with neck pain. The aim of the study was to determine whether there is a pattern of altered alignment of the shoulder girdle and the cervical and thoracic spine in patients with neck pain. A three-dimensional device measured clavicle and scapular orientation, and cervical and thoracic alignment in patients with insidious onset neck pain (IONP) and whiplash-associated disorder (WAD). An asymptomatic control group was selected for baseline measurements. The symptomatic groups revealed a significantly reduced clavicle retraction and scapular upward rotation as well as decreased cranial angle. A difference was found between the symptomatic groups on the left side, whereas the WAD group revealed an increased scapular anterior tilt and the IONP group a decreased clavicle elevation. These changes may be an important mechanism for maintenance and recurrence or exacerbation of symptoms in patients with neck pain. Keywords: neck pain, whiplash, scapula, posture Clinical theory suggests that altered alignment of of Biomechanics. -

Radiohamate Impingement After Proximal Row Carpectomy ‘Radiohamate Impingement PRC’
Acta Orthop. Belg., 2020, 86 e-supplement 1, 19-21 CASE REPORT Radiohamate impingement after proximal row carpectomy ‘Radiohamate impingement PRC’ Pieter Caekebeke, Luc De Smet From the Department of Orthopaedics UZ Leuven, Pellenberg, Belgium Radiocarpal impingement after PRC is a well-known from 0% to 18% (5). Radiocarpal and pisiform complication due to impingement of the radial styloid impingement have been described after PRC. The against the radial carpal bones. A less common first is probably due to the proximalization of the impingement syndrome is that of the pisiforme. distal row with impingement of the trapezium/ We describe a radiohamate impingement and its trapezoid against the radial styloid process. The diagnosis and treatment. Based on a case we saw treatment is a radial styloid process resection for at our practice. Diagnosis is bases on standard radiographs and SPECT-CT. The treatment is the first and a pisiformectomy for the latter (3,5). No initially conservative. Surgery is necessary when other impingement syndromes have been described. conservative treatment fails and consists of resectie We present a case of radiohamate impingement of the proximal pole of the hamate. syndrome after proximal row carpectomy. Keywords: Radiohamate ; impingement ; proximal row CASE REPORT carpectomy. A 53-year-old mechanic contacted us 1 year after a work-accident with localized radiocarpal INTRODUCTION pain and swelling. Radiographs showed a stage Proximal row carpectomy (PRC) is a well- two SLAC wrist. (Fig. 1) A PRC with synovectomy established motion-preserving salvage procedure was performed. The following 3 years were for degenerative disorders of the proximal carpal uneventful with no to minimal pain complaints. -
Suprascapular Nerve Entrapment: Technique for Arthroscopic Release
Techniques in Shoulder and Elbow Surgery 7(2):000–000, 2006 Ó 2006 Lippincott Williams & Wilkins, Philadephia | REVIEW | Suprascapular Nerve Entrapment: Technique for Arthroscopic Release Peter J. Millett, MD, MSc Steadman Hawkins Clinic, Vail, CO Harvard Medical School Boston, MA R. Shane Barton, MD, Iva´n H. Pacheco, MD, and Reuben Gobezie, MD Harvard Shoulder Service Harvard Medical School Brigham and Women’s Hospital Massachusetts General Hospital Boston, MA | ABSTRACT with suprascapular nerve palsy may present with an often vague range of symptoms or even be asympto- Suprascapular neuropathy can be caused by a variety of matic.3 Pain over the posterolateral shoulder or easy anatomic and pathologic entities as the nerve courses fatigability with overhead activities may be reported, or from the brachial plexus through the suprascapular and painless weakness of external rotation with or without spinoglenoid notches to innervate the supraspinatus and spinatus muscle atrophy may be noted. Compression of infraspinatus muscles. We describe techniques for arthro- the nerve at both the suprascapular and spinoglenoid scopically accessing the nerve at both the suprascapular notches are commonly reported mechanisms of injury and spinoglenoid notches and decompressing structural and will be discussed in detail. lesions that may be contributing to the neuropathy. The physical examination plays a critical role in Keywords: suprascapular neuropathy, suprascapular discerning the site of suprascapular nerve injury. notches, spinoglenoid notches, cyst decompression, arthro- Clinical observation of the patient’s shoulder girdle is scopic release important. More proximal injury, as seen with supra- | HISTORICAL PERSPECTIVE scapular notch compression, may result in atrophy of both the supraspinatus and infraspinatus, whereas more Isolated injury to the suprascapular nerve has long been distal compression at the spinoglenoid notch will result recognized as an etiologic entity producing shoulder pain in isolated infraspinatus weakness and atrophy (Fig. -

The Appendicular Skeleton Appendicular Skeleton
THE SKELETAL SYSTEM: THE APPENDICULAR SKELETON APPENDICULAR SKELETON The primary function is movement It includes bones of the upper and lower limbs Girdles attach the limbs to the axial skeleton SKELETON OF THE UPPER LIMB Each upper limb has 32 bones Two separate regions 1. The pectoral (shoulder) girdle (2 bones) 2. The free part (30 bones) THE PECTORAL (OR SHOULDER) GIRDLE UPPER LIMB The pectoral girdle consists of two bones, the scapula and the clavicle The free part has 30 bones 1 humerus (arm) 1 ulna (forearm) 1 radius (forearm) 8 carpals (wrist) 19 metacarpal and phalanges (hand) PECTORAL GIRDLE - CLAVICLE The clavicle is “S” shaped The medial end articulates with the manubrium of the sternum forming the sternoclavicular joint The lateral end articulates with the acromion forming the acromioclavicular joint THE CLAVICLE PECTORAL GIRDLE - CLAVICLE The clavicle is convex in shape anteriorly near the sternal junction The clavicle is concave anteriorly on its lateral edge near the acromion CLINICAL CONNECTION - FRACTURED CLAVICLE A fall on an outstretched arm (F.O.O.S.H.) injury can lead to a fractured clavicle The clavicle is weakest at the junction of the two curves Forces are generated through the upper limb to the trunk during a fall Therefore, most breaks occur approximately in the middle of the clavicle PECTORAL GIRDLE - SCAPULA Also called the shoulder blade Triangular in shape Most notable features include the spine, acromion, coracoid process and the glenoid cavity FEATURES ON THE SCAPULA Spine -