Interpretation Oftrauma Radiographs by Junior Doctors in Accident And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
What Is a Scaphoid Fracture?
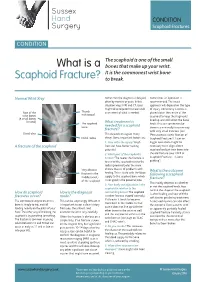
Sussex Hand CONDITION Surgery Scaphoid Fractures CONDITION The scaphoid is one of the small What is a bones that make up your wrist. It is the commonest wrist bone Scaphoid Fracture? to break. Normal Wrist Xray Sometimes the diagnosis is delayed, Sometimes an operation is often by months or years. In this recommended. The exact situation xrays, MRI and CT scans approach will depend on the type might all be required to make a full of injury. Commonly a screw is Rest of the Thumb assessment of what is needed. placed down the centre of the metacarpal wrist bones scaphoid to keep the fragments (8 small bones lined up and still whilst the bone in total) The scaphoid What treatment is heals. This can sometimes be bone needed for a scaphoid done in a minimally invasive way fracture? with very small incisions (see Distal ulna This depends on a great many ‘Percutaneous screw fixation of Distal radius things. Some important factors are: Scaphoid Fractures’). Later on 1. How old is the injury? Fresh bigger operations might be A fracture of the scaphoid fractures have better healing necessary to re-align a bent potential scaphoid and put new bone into 2. Which part of the scaphoid is the old fracture (see ‘ORIF of broken? The nearer the fracture is Scaphoid Fractures +/-bone to end of the scaphoid next to the grafting’). radius (proximal pole) the more Very obvious chance there is of problems with What is the outcome fracture in the healing. This is to do with the blood following a scaphoid middle (waist) supply to the scaphoid bone which fracture? of the scaphoid is not good in the proximal pole. -

EM Cases Digest Vol. 1 MSK & Trauma
THE MAGAZINE SERIES FOR ENHANCED EM LEARNING Vol. 1: MSK & Trauma Copyright © 2015 by Medicine Cases Emergency Medicine Cases by Medicine Cases is copyrighted as “All Rights Reserved”. This eBook is Creative Commons Attribution-NonCommercial- NoDerivatives 3.0 Unsupported License. Upon written request, however, we may be able to share our content with you for free in exchange for analytic data. For permission requests, write to the publisher, addressed “Attention: Permissions Coordinator,” at the address below. Medicine Cases 216 Balmoral Ave Toronto, ON, M4V 1J9 www.emergencymedicinecases.com This book has been authored with care to reflect generally accepted practices. As medicine is a rapidly changing field, new diagnostic and treatment modalities are likely to arise. It is the responsibility of the treating physician, relying on his/her experience and the knowledge of the patient, to determine the best management plan for each patient. The author(s) and publisher of this book are not responsible for errors or omissions or for any consequences from the application of the information in this book and disclaim any liability in connection with the use of this information. This book makes no guarantee with respect to the completeness or accuracy of the contents within. OUR THANKS TO... EDITORS IN CHIEF Anton Helman Taryn Lloyd PRODUCTION EDITOR Michelle Yee PRODUCTION MANAGER Garron Helman CHAPTER EDITORS Niran Argintaru Michael Misch PODCAST SUMMARY EDITORS Lucas Chartier Keerat Grewal Claire Heslop Michael Kilian PODCAST GUEST EXPERTS Andrew Arcand Natalie Mamen Brian Steinhart Mike Brzozowski Hossein Mehdian Arun Sayal Ivy Cheng Sanjay Mehta Laura Tate Walter Himmel Jonathan Pirie Rahim Valani Dave MacKinnon Jennifer Riley University of Toronto, Faculty of Medicine EM Cases is a venture of the Schwartz/ Reisman Emergency Medicine Institute. -

Scaphoid Fracture PA Radiograph
30 y/o male with acute left wrist pain Student Name….None was listed Atul Kumar, MD, MS PA Radiograph Non Contrast Coronal CT ? Scaphoid Fracture PA radiograph Distal pole Scaphoid fracture Proximal pole • PA x-ray showing transverse scaphoid fracture. Non Contrast Coronal CT Capitate Trapezoid Hamate Trapezium Triquetrum Lunate Scaphoid fracture Scaphoid Fracture • Mechanism: direct axial compression or with hyperextension (fall onto an outstretched hand). • Symptoms: pain localized at the radial aspect of wrist often associated with swelling and reduced grip strength. – Pain in anatomic snuffbox suspicious for waist fracture, which is the most common type. • Because scaphoid fractures are often radiologically occult, any tenderness in the anatomic snuffbox should be treated as a scaphoid fracture. • Scaphoid blood supply (palmar carpal branch of the radial artery) runs from the distal to the proximal pole. Transverse fracture of the proximal pole can lead to osteonecrosis and nonunion due to disruption of blood flow. http://epmonthly.com/wp-content/uploads/2016/04/OrthoB.png Scaphoid Fracture • Differential diagnosis: distal radius fracture, wrist sprain, and other carpal injuries other than scaphoid. • In suspected scaphoid fractures, plain radiographs (including PA, true lateral, oblique, and scaphoid views) are ordered as the first diagnostic step. • However, the false negative rate for radiographs taken immediately after injury up to 20-54%. • Definitive diagnosis can be made by MRI or CT scan. They have a comparable diagnostic accuracy and do not result in overtreatments. Avascular necrosis/Nonunion Scaphoid view radiograph (A) and CT scan (B) showing nonunion (arrow) and avascular necrosis (asterisk) and the Terry Thomas sign – scapholunate ligament injury (arrowhead). -

Wrist Injury Article 12-19-16
ARTICLE: Wrist Injuries This week we are going to talk about 3 unusual wrist injuries all of which can cause considerable problems and the potential complications of each. The first is a TFCC injury. The TFCC or triangular fibrocartilage is a small meniscus or pad on the ulnar side of the wrist (pinky side) which can become torn during a fall on an outstretched hand and can cause clicking, popping and pain on this side of the wrist. The TFCC is sometimes difficult to detect and often misdiagnosed as a wrist sprain but is rather different than a sprained wrist in that it is not an injury of ligament but is an injury of cartilage. The injury can be spotted with a shear test and is properly diagnosed with an arthrogram. The second unusual injury to the wrist is the scaphoid fracture. The scaphoid fracture of the wrist is a bone injury which occurs when the scaphoid bone on the radial side of the wrist (thumb side) is broken at it’s waist (center) injuring the blood supply to the proximal pole of the scaphoid. This injury results in avascular necrosis or bone death of the scaphoid. Also occurring after a fall on an outstretched hand the scaphoid fracture is often misdiagnosed as a wrist sprain but is more correctly described as a fracture. The hallmark symptom of a scaphoid fracture is it’s failure to heal and persistent pain on the radial side of the wrist. The scaphoid fracture is often missed on the initial x-ray as the bone has not had time yet to die off and is often seen on a second film. -

Your Wrist Bones
www.healthinfo.org.nz Your wrist bones Your wrist is made up of eight small bones (called the carpal bones). Each carpal bone has a specific name, shown in the image on the right. The carpal bones connect with the two long bones in your forearm (the radius and ulna). Your wrist moves where they connect. This makes your wrist a very complex structure, as there are many different joints within it. If any one of your carpal bones breaks, it can change position slightly, causing pain and problems with movement. Occasionally it can also lead to arthritis. Causes of a broken wrist A broken wrist usually happens from falling on to an outstretched hand. Serious accidents, such as car accidents, motorcycle accidents, or falls from a ladder cause more serious breaks. Weak bones (for example, in someone with osteoporosis) tend to break more easily. If you break your wrist without significant force, your doctor may recommend checking if you have osteoporosis. If you meet the criteria, they may send you for a bone density scan. Any one of the 10 bones in your wrist can break, but the most common bone to break is the radius, in your forearm. This is called a distal radius fracture. Another common wrist fracture is a scaphoid fracture, which is a break in one of your small carpal bones. This can be difficult to diagnose, and there is a risk a scaphoid fracture might not heal. Your wrist can break in many different ways, and some breaks are worse than others. How bad a break it is depends on how many pieces a bone breaks into, whether they are stable or move around a lot, and whether the broken ends of the bone are still in the right place. -

Imaging and Treatment of Scaphoid Fractures and Their Complications
159 Imaging and Treatment of Scaphoid Fractures and Their Complications Mihra S. Taljanovic, M.D., M.Sc., F.A.C.R. 1 Apostolos Karantanas, M.D., Ph.D. 2, 3 James F. Griffith, M.D. 4 Gregory L. DeSilva, M.D. 5 Joshua D. Rieke, M.D. 1 Joseph E. Sheppard, M.D. 5 1 Department of Medical Imaging, The University of Arizona Health Address for correspondence and reprint requests Mihra S. Taljanovic, Network, Tucson, Arizona. M.D., M.Sc., Department of Medical Imaging, The University of Arizona 2 Department of Radiology, University of Crete, Heraklion, Greece. Health Network, 1501 N. Campbell Ave., Tucson, AZ 85724-5067 3 Department of Medical Imaging, University Hospital, Heraklion, (e-mail: [email protected]). Greece. 4 Department of Imaging and Interventional Radiology, Prince of Wales Hospital, Shatin, New Territories, Hong Kong. 5 Department of Orthopaedic Surgery, The University of Arizona Health Network, Tucson, Arizona. Semin Musculoskelet Radiol 2012;16:159–174. Abstract The scaphoid is the most commonly fractured carpal bone, with frequent complications that are predisposed by its anatomical location, anatomical configuration (shape and length), and vascular supply. The most common mechanism of injury is a fall onto an outstretched hand. Imaging plays a significant role in the initial evaluation and treatment of scaphoid fractures and their complications. Radiography should be the first imaging modality in the initial evaluation and follow-up of scaphoid fractures. Computed tomography with its superb spatial resolution enables better visualization and charac- terization of the fracture line, and the amount of displacement and angulation of the fracture fragments. -

Section J: Trauma J
Section J: Trauma J Clinical/Diagnostic Investigation Recommendation Dose Comment Problem (Grade) Head J01. Head injury SXR Not indicated [B] d There is poor correlation between the presence of a skull fracture and a clinically significant head injury. The only (For children see indications for skull x-rays in the setting of trauma are Section L) suspected open or depressed skull fractures, if CT is not available and suspected child abuse. Section J: Trauma CT Indicated [A] dd CT is indicated in all patients with a severe head injury (GCS <13). In patients with a minor head injury (GCS 13-15 and witnessed loss of consciousness or disorientation or definite amnesia) CT is indicated to rule out an injury requiring neurosurgical intervention if there is: • GCS <15 2 hours after the injury • Suspected open or depressed skull fracture • Any sign of a basal skull fracture • Two or more episodes of vomiting • Age > 65 years To rule out any other clinically significant intracranial injury, the following additional risk factors justify obtaining CT: • Amnesia for before the impact lasting > 30 minutes • Dangerous mechanism of injury (motor vehicle accident or fall from> 3 feet or 5 stairs or more). CTA Specialized dd CTA should be performed with presentation of high energy Investigation [B] transfer mechanism or if associated with any of the following: • Displaced mid-face fracture • Basilar skull fracture with carotid canal involvement • Focal neurological deficit • Cervical vertebral body or transverse foramen fracture • Fracture at C1-C3 • Clothesline type injury or seat belt abrasion with significant swelling/pain • Altered mental status Face and orbits J02. -

Comparison of Computed Tomographic and Magnetic Resonance Imaging in Fracture Healing After Spinal Injury
Spinal Cord (2009) 47, 874–877 & 2009 International Spinal Cord Society All rights reserved 1362-4393/09 $32.00 www.nature.com/sc ORIGINAL ARTICLE Comparison of computed tomographic and magnetic resonance imaging in fracture healing after spinal injury R Warwick1, JM Willatt2, B Singhal3, J Borremans4 and T Meagher1 1Department of Radiology, Stoke Mandeville Hospital, Aylesbury, Bucks, UK; 2Department of Radiology, University of Michigan, Ann Arbor, MI, USA; 3National Spinal Injuries Centre, Stoke Mandeville Hospital, Aylesbury, Bucks, UK and 4Spinal Surgery and Rehabilitation Medicine Regionalverbund Kirchlicher Krankenha¨user Bruder Klaus Krankenhaus Heitere Weg 10, Waldkirch, Germany Study design: Single-centre, prospective (comparative cohort) clinical study, with ethical approval and patient consent. Objective: Confirmation of vertebral fracture union can pose significant challenges for clinicians in the management of spinal cord injury and in the decisions around patient mobilization. Bony union is usually assessed with computed tomography (CT). This study hypothesizes that magnetic resonance imaging (MRI) can identify vertebral bone union. Setting: A major spinal injuries unit in the United Kingdom. Method: Patients underwent CT and MRI at 12 weeks post-injury, if conservatively managed, or 12 weeks post-fixation. With CT as the gold standard, the MRI scans were reviewed blind to the CT result and indicators for fracture healing were compared. Results: A total of 35 patients with 55 fractures were imaged. Comparison of CT and MRI showed sensitivity of 88%, specificity of 100% and positive predictive value of 100% for fracture union imaged with MRI using CT as the gold standard. Conclusion: MRI correlates well with CT in identifying vertebral fracture union and non-union. -
Early Management of Upper Limb Fractures in General Practice
Bones • THEME Early management of upper limb fractures in general practice eneral practitioners are frequently confronted with BACKGROUND Upper limb injuries are very G injuries to the upper limb, most commonly from falls. David Spain, common and patients frequently present to general practitioners for treatment. Circumstances This article focusses on upper limb fractures and the MBBS, FRACGP, important issues relevant to correct early management. FACEM, is Director, of the injury and varied patient factors are critical Allamanda 24 Hour to assessment. Outcome of these injuries involves History of injury Emergency Care short term pain control and diagnosis; fracture Centre, Allamanda immobilisation, comfort and function in the A careful history should consider in detail the circum- Private Hospital, Senior Staff Specialist, treatment device medium term; and longer term, stances of the accident or fall (Table 1). This helps predict Emergency the best functional outcome. likely injury and is essential to distinguish simple slip falls Department, Gold OBJECTIVE This article aims to guide GPs from medical causes of collapse. Isolated injury must be Coast Hospital, and Clinical Senior Lecturer, through the initial assessment and early distinguished from an injury as a part of actual or potential the University of management of fractures and provides a logical, multiple trauma. Patients with a severe dramatic and Queensland. simple structure for this process. Understanding painful injury can be distracted, often resulting in other of different injury patterns and patient injuries of significance being initially overlooked. Simple characteristics to assist correct overall enquiry about other possible injury often unearths management is emphasised and the correct unusual replies. -
Upper Limb Injuries
- 1 - BCCH Emergency Department UPPER LIMB INJURIES Resource pack Developed by: RENA HEATHCOTE RN Rena Heathcote BCCH Emergency Department 2012 - 2 - FRACTURES The shoulder Dislocation +/_ fracture of humeral head History • A dislocated shoulder generally follows a fall onto their arm, or directly onto their shoulder, causing the humeral head to dislocate from the joint capsule and out of the socket. • This usually results in an anterior (towards the front) dislocation of the humeral head, where it is positioned in front of the joint socket. More rarely the humeral head dislocates posteriorly (behind) or inferiorly (underneath). Assessment • The patient usually walks in holding their arm, and in obvious pain • There is obvious deformity to the shoulder joint, noted as flattening to the top of the arm at the shoulder joint (the deltoid muscle region), and more obvious bony prominence. Obvious deformity of the shoulder, In this case, the humeral head has dislocated inferiorly Rena Heathcote BCCH Emergency Department 2012 - 3 - • The humeral head can at times be felt in the axilla • Caution: The axillary nerve can become damaged causing paralysis over the deltoid region, and the absence of sensation over a patch below the shoulder. • Sensation and radial pulse must always be checked Treatment • Remove all rings on digits to prevent swelling and neuro‐vascular compromise • Place the patients’ arm in a broad arm sling, according to the patients’ comfort • These patients should have an immediate shoulder x‐ray to exclude any underlying accompanying -
Diagnosis and Management of Scaphoid Fractures T
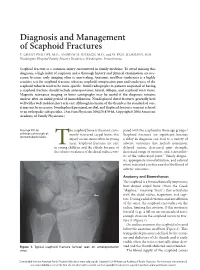
Diagnosis and Management of Scaphoid Fractures T. GRANT PHILLIPS, M.D., ANDREW M. REIBACH, M.D., and W. PAUL SLOMIANY, M.D. Washington Hospital Family Practice Residency, Washington, Pennsylvania Scaphoid fracture is a common injury encountered in family medicine. To avoid missing this diagnosis, a high index of suspicion and a thorough history and physical examination are nec- essary, because early imaging often is unrevealing. Anatomic snuffbox tenderness is a highly sensitive test for scaphoid fracture, whereas scaphoid compression pain and tenderness of the scaphoid tubercle tend to be more specific. Initial radiographs in patients suspected of having a scaphoid fracture should include anteroposterior, lateral, oblique, and scaphoid wrist views. Magnetic resonance imaging or bone scintigraphy may be useful if the diagnosis remains unclear after an initial period of immobilization. Nondisplaced distal fractures generally heal well with a well-molded short arm cast. Although inclusion of the thumb is the standard of care, it may not be necessary. Nondisplaced proximal, medial, and displaced fractures warrant referral to an orthopedic subspecialist. (Am Fam Physician 2004;70:879-84. Copyright© 2004 American Academy of Family Physicians.) See page 801 for he scaphoid bone is the most com- pared with the scaphoid in these age groups.1 definitions of strength-of- monly fractured carpal bone; this Scaphoid fractures are significant because recommendation labels. injury occurs most often in young a delay in diagnosis can lead to a variety of men. Scaphoid fractures are rare adverse outcomes that include nonunion, inT young children and the elderly because of delayed union, decreased grip strength, the relative weakness of the distal radius com- decreased range of motion, and osteoarthri- tis of the radiocarpal joint.2 Timely diagno- sis, appropriate immobilization, and referral when indicated can decrease the likelihood of adverse outcomes. -

6 Osteoporosis and Fractures
Arthritis and osteoporo sis in Australia 2008 6 Osteoporosis and fractures Osteoporosis (meaning ‘porous bones’) is a condition in which the bones weaken and lose structural integrity, resulting in high risk of fracture. People with osteoporosis may have substantially decreased bone mass, clinically defined as bone mineral density (BMD) a certain amount below the average level in young adults. The decrease in bone mass makes the bones more fragile and they are broken more easily than bones of ‘normal’ mass. A major feature of osteoporosis is fractures that occur following little or no trauma, known as ‘minimal trauma fractures’. These fractures may affect bodily movement and functioning, which can result in disability, affect social interaction and quality of life, and lead to a loss of independence. Hip fractures in older people are a common result of longstanding osteoporosis and are associated with high levels of morbidity and increased mortality. This chapter provides an overview of the nature, impacts and treatment of osteoporosis. It also describes some of the more common osteoporotic fractures, and outlines various fracture prevention strategies. Prevalence and detection of osteoporosis Self-reported data indicate that almost 581,000 Australians have been diagnosed with osteoporosis, with the vast majority being over 55 years of age. Women are much more likely to report osteoporosis than men. However, osteoporosis has no outward symptoms, and people often do not know that they have the condition until a fracture occurs. It is believed that the number of people who have osteoporosis, and who are therefore at high risk of fracture, is much larger than the estimates obtained from self-reported information.