Operative Note 4: Internal Fixation of Clavicle Fracture
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
What Is a Scaphoid Fracture?
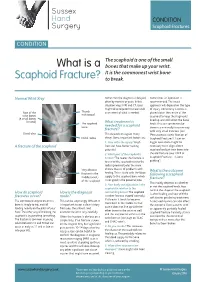
Sussex Hand CONDITION Surgery Scaphoid Fractures CONDITION The scaphoid is one of the small What is a bones that make up your wrist. It is the commonest wrist bone Scaphoid Fracture? to break. Normal Wrist Xray Sometimes the diagnosis is delayed, Sometimes an operation is often by months or years. In this recommended. The exact situation xrays, MRI and CT scans approach will depend on the type might all be required to make a full of injury. Commonly a screw is Rest of the Thumb assessment of what is needed. placed down the centre of the metacarpal wrist bones scaphoid to keep the fragments (8 small bones lined up and still whilst the bone in total) The scaphoid What treatment is heals. This can sometimes be bone needed for a scaphoid done in a minimally invasive way fracture? with very small incisions (see Distal ulna This depends on a great many ‘Percutaneous screw fixation of Distal radius things. Some important factors are: Scaphoid Fractures’). Later on 1. How old is the injury? Fresh bigger operations might be A fracture of the scaphoid fractures have better healing necessary to re-align a bent potential scaphoid and put new bone into 2. Which part of the scaphoid is the old fracture (see ‘ORIF of broken? The nearer the fracture is Scaphoid Fractures +/-bone to end of the scaphoid next to the grafting’). radius (proximal pole) the more Very obvious chance there is of problems with What is the outcome fracture in the healing. This is to do with the blood following a scaphoid middle (waist) supply to the scaphoid bone which fracture? of the scaphoid is not good in the proximal pole. -
EM Cases Digest Vol. 1 MSK & Trauma
THE MAGAZINE SERIES FOR ENHANCED EM LEARNING Vol. 1: MSK & Trauma Copyright © 2015 by Medicine Cases Emergency Medicine Cases by Medicine Cases is copyrighted as “All Rights Reserved”. This eBook is Creative Commons Attribution-NonCommercial- NoDerivatives 3.0 Unsupported License. Upon written request, however, we may be able to share our content with you for free in exchange for analytic data. For permission requests, write to the publisher, addressed “Attention: Permissions Coordinator,” at the address below. Medicine Cases 216 Balmoral Ave Toronto, ON, M4V 1J9 www.emergencymedicinecases.com This book has been authored with care to reflect generally accepted practices. As medicine is a rapidly changing field, new diagnostic and treatment modalities are likely to arise. It is the responsibility of the treating physician, relying on his/her experience and the knowledge of the patient, to determine the best management plan for each patient. The author(s) and publisher of this book are not responsible for errors or omissions or for any consequences from the application of the information in this book and disclaim any liability in connection with the use of this information. This book makes no guarantee with respect to the completeness or accuracy of the contents within. OUR THANKS TO... EDITORS IN CHIEF Anton Helman Taryn Lloyd PRODUCTION EDITOR Michelle Yee PRODUCTION MANAGER Garron Helman CHAPTER EDITORS Niran Argintaru Michael Misch PODCAST SUMMARY EDITORS Lucas Chartier Keerat Grewal Claire Heslop Michael Kilian PODCAST GUEST EXPERTS Andrew Arcand Natalie Mamen Brian Steinhart Mike Brzozowski Hossein Mehdian Arun Sayal Ivy Cheng Sanjay Mehta Laura Tate Walter Himmel Jonathan Pirie Rahim Valani Dave MacKinnon Jennifer Riley University of Toronto, Faculty of Medicine EM Cases is a venture of the Schwartz/ Reisman Emergency Medicine Institute. -

Midshaft Clavicle Fracture
You have a Midshaft Clavicle Fracture This is a break to the middle of your collar bone. Healing: It normally takes 6-12 weeks to heal, but symptoms can continue for 3-6 months. Smoking will slow down your healing. We would advise that you stop smoking while your fracture heals. Talk to your GP or go to www.smokefree.nhs.uk for more information. Pain and Swelling: Your shoulder may be swollen and you will have some pain. Taking pain medication and using ice or cold packs will help. More information is on the next page. Wearing your sling: Use your sling for 3 weeks. You can take it off to wash, dress and do your exercises. It does not need to be worn at night. Exercise and activity: It is important to start gentle exercises straight away to prevent stiffness. You will find pictures and instructions for your exercises below. You should not do any heavy lifting or overhead movement for the first 6 weeks. Follow up: You will see a shoulder specialist 3 weeks after your injury. They may do another x-ray to check the position of your fracture. They will explain the next stage of your rehabilitation. If you have not received your appointment letter within 1 week, please contact us. Contact us: If you are concerned about your symptoms, are unable to follow this rehabilitation plan or notice pain other than at your shoulder, please contact the Virtual Fracture Clinic. Updated 9th June 2021 Caring for your injury: Weeks 1-3 Remember to use your sling for the first 3 weeks. -

Comparison of Four Different Internal Fixation Methods in the Treatment of Distal Clavicle Fractures
EXPERIMENTAL AND THERAPEUTIC MEDICINE 19: 451-458, 2020 Comparison of four different internal fixation methods in the treatment of distal clavicle fractures LIANG LI*, HONGXIAO WU*, PEICHAO JIANG, XIAOCHUAN HAN, SHIYUAN CHEN and XUEZHONG YU Department of Orthopaedics, Dongying People's Hospital, Dongying, Shandong 257091, P.R. China Received March 15, 2019; Accepted August 8, 2019 DOI: 10.3892/etm.2019.8233 Abstract. This study compared the clinical efficacy of four of shoulder pain, an increase in the range of motion of the internal fixation methods in the treatment of distal clavicle shoulder, and a reduction in complications, and thus, are pref- fractures, in an effort to guide appropriate selection and erable for the early functional recovery of limbs. application in the clinic. Eighty‑four patients with distal clav- icle‑comminuted fractures were treated with a distal clavicle Introduction anatomic plate (group A), clavicular hook plate (group B), double‑plate vertical fixation (group C), or T‑shaped steel Due to its subcutaneous location, clavicle is one of the bones plate internal fixation (group D). The Constant‑Murley scoring that are most frequently fractured in the upper body due to car system was used to evaluate the shoulder joint function. The accidents and sports trauma. The incidence of distal clavicle fracture healing time, VAS, and postoperative complications fractures accounts for 12‑21% of all clavicular fractures (1). were compared and analyzed among the four groups. According Distal clavicle fractures are typically attributed to a direct to the Constant‑Murley evaluation standard, the excellent and blow to the point of the shoulder or a fall on an outstretched good rates of the four groups were 94.4, 73.1, 95 and 80% hand. -

Complications Associated with Clavicular Fracture
NOR200061.qxd 9/11/09 1:23 PM Page 217 Complications Associated With Clavicular Fracture George Mouzopoulos ▼ Emmanuil Morakis ▼ Michalis Stamatakos ▼ Mathaios Tzurbakis The objective of our literature review was to inform or- subclavian vein, due to its stable connection with the thopaedic nurses about the complications of clavicular frac- clavicle via the cervical fascia, can also be subjected to ture, which are easily misdiagnosed. For this purpose, we injuries (Casbas et al., 2005). Damage to the internal searched MEDLINE (1965–2005) using the key words clavicle, jugular vein, the suprascapular artery, the axillary, and fracture, and complications. Fractures of the clavicle are usu- carotid artery after a clavicular fracture has also been ally thought to be easily managed by symptomatic treatment reported (Katras et al., 2001). About 50% of injuries to the subclavian arteries are in a broad arm sling. However, it is well recognized that not due to fractures of the clavicle because the proximal all clavicular fractures have a good outcome. Displaced or part is dislocated superiorly by the sternocleidomas- comminuted clavicle fractures are associated with complica- toid, causing damage to the vessel (Sodhi, Arora, & tions such as subclavian vessels injury, hemopneumothorax, Khandelwal, 2007). If no injury happens during the ini- brachial plexus paresis, nonunion, malunion, posttraumatic tial displacement of the fractured part, then it is un- arthritis, refracture, and other complications related to os- likely to happen later, because the distal segment is dis- teosynthesis. Herein, we describe what the orthopaedic nurse placed downward and forward due to shoulder weight, should know about the complications of clavicular fractures. -

Scaphoid Fracture PA Radiograph
30 y/o male with acute left wrist pain Student Name….None was listed Atul Kumar, MD, MS PA Radiograph Non Contrast Coronal CT ? Scaphoid Fracture PA radiograph Distal pole Scaphoid fracture Proximal pole • PA x-ray showing transverse scaphoid fracture. Non Contrast Coronal CT Capitate Trapezoid Hamate Trapezium Triquetrum Lunate Scaphoid fracture Scaphoid Fracture • Mechanism: direct axial compression or with hyperextension (fall onto an outstretched hand). • Symptoms: pain localized at the radial aspect of wrist often associated with swelling and reduced grip strength. – Pain in anatomic snuffbox suspicious for waist fracture, which is the most common type. • Because scaphoid fractures are often radiologically occult, any tenderness in the anatomic snuffbox should be treated as a scaphoid fracture. • Scaphoid blood supply (palmar carpal branch of the radial artery) runs from the distal to the proximal pole. Transverse fracture of the proximal pole can lead to osteonecrosis and nonunion due to disruption of blood flow. http://epmonthly.com/wp-content/uploads/2016/04/OrthoB.png Scaphoid Fracture • Differential diagnosis: distal radius fracture, wrist sprain, and other carpal injuries other than scaphoid. • In suspected scaphoid fractures, plain radiographs (including PA, true lateral, oblique, and scaphoid views) are ordered as the first diagnostic step. • However, the false negative rate for radiographs taken immediately after injury up to 20-54%. • Definitive diagnosis can be made by MRI or CT scan. They have a comparable diagnostic accuracy and do not result in overtreatments. Avascular necrosis/Nonunion Scaphoid view radiograph (A) and CT scan (B) showing nonunion (arrow) and avascular necrosis (asterisk) and the Terry Thomas sign – scapholunate ligament injury (arrowhead). -

Wrist Injury Article 12-19-16
ARTICLE: Wrist Injuries This week we are going to talk about 3 unusual wrist injuries all of which can cause considerable problems and the potential complications of each. The first is a TFCC injury. The TFCC or triangular fibrocartilage is a small meniscus or pad on the ulnar side of the wrist (pinky side) which can become torn during a fall on an outstretched hand and can cause clicking, popping and pain on this side of the wrist. The TFCC is sometimes difficult to detect and often misdiagnosed as a wrist sprain but is rather different than a sprained wrist in that it is not an injury of ligament but is an injury of cartilage. The injury can be spotted with a shear test and is properly diagnosed with an arthrogram. The second unusual injury to the wrist is the scaphoid fracture. The scaphoid fracture of the wrist is a bone injury which occurs when the scaphoid bone on the radial side of the wrist (thumb side) is broken at it’s waist (center) injuring the blood supply to the proximal pole of the scaphoid. This injury results in avascular necrosis or bone death of the scaphoid. Also occurring after a fall on an outstretched hand the scaphoid fracture is often misdiagnosed as a wrist sprain but is more correctly described as a fracture. The hallmark symptom of a scaphoid fracture is it’s failure to heal and persistent pain on the radial side of the wrist. The scaphoid fracture is often missed on the initial x-ray as the bone has not had time yet to die off and is often seen on a second film. -

Your Wrist Bones
www.healthinfo.org.nz Your wrist bones Your wrist is made up of eight small bones (called the carpal bones). Each carpal bone has a specific name, shown in the image on the right. The carpal bones connect with the two long bones in your forearm (the radius and ulna). Your wrist moves where they connect. This makes your wrist a very complex structure, as there are many different joints within it. If any one of your carpal bones breaks, it can change position slightly, causing pain and problems with movement. Occasionally it can also lead to arthritis. Causes of a broken wrist A broken wrist usually happens from falling on to an outstretched hand. Serious accidents, such as car accidents, motorcycle accidents, or falls from a ladder cause more serious breaks. Weak bones (for example, in someone with osteoporosis) tend to break more easily. If you break your wrist without significant force, your doctor may recommend checking if you have osteoporosis. If you meet the criteria, they may send you for a bone density scan. Any one of the 10 bones in your wrist can break, but the most common bone to break is the radius, in your forearm. This is called a distal radius fracture. Another common wrist fracture is a scaphoid fracture, which is a break in one of your small carpal bones. This can be difficult to diagnose, and there is a risk a scaphoid fracture might not heal. Your wrist can break in many different ways, and some breaks are worse than others. How bad a break it is depends on how many pieces a bone breaks into, whether they are stable or move around a lot, and whether the broken ends of the bone are still in the right place. -

Medial Clavicle Fracture Dislocation Surgically Treated: Case Report Miguel Frias*, Renato Ramos, Marco Bernardes, Tiago Pinheiro Torres and Pedro Lourenço
ISSN: 2469-5777 Frias et al. Trauma Cases Rev 2018, 4:066 DOI: 10.23937/2469-5777/1510066 Volume 4 | Issue 2 Trauma Cases and Reviews Open Access CASE REPORT Medial Clavicle Fracture Dislocation Surgically Treated: Case Report Miguel Frias*, Renato Ramos, Marco Bernardes, Tiago Pinheiro Torres and Pedro Lourenço Centro Hospitalar de Vila Nova de Gaia/Espinho, Portugal *Corresponding author: Miguel Frias, Centro Hospitalar de Vila Nova de Gaia/Espinho, Porto, Portugal Check for updates injury to the trachea and esophagus and the possibility Abstract of pneumothorax [7]. The medial clavicle fracture is a rare injury and almost all the times conservatively treated. Therefore, the number of Although rare, such injuries require rapid diagnosis operations reported in the literature are limited. Posterior followed by effective treatment to avoid future dislocation can result in serious complications and such complications [8]. Specifically, periarticular and injuries require rapid diagnosis followed by effective treat- ment to avoid future complications. The present case re- intraarticular fractures remain a therapeutic challenge: ports a case of a 33-year-old healthy man that was involved The medial fragment is too small to stabilize with in a high-fall, being diagnosed with a rare displaced medi- common linear implants, and bending forces that occur al clavicular fracture associated with an unstable posterior during shoulder motion are disproportionately high lateral fragment dislocation surgically treated. Imagiological images and intraoperative photographs are presented. The [9]. Indications for surgery have traditionally included authors collected this case in order to report this rare and open fractures, soft-tissue damage, or neurovascular complex injury. -
Use of an Absorbable Plate in the Management of a Clavicle Fracture in an Adolescent
A Case Report & Literature Review Use of an Absorbable Plate in the Management of a Clavicle Fracture in an Adolescent Eric W. Edmonds, MD was successfully used to manage delayed union of a Abstract displaced and shortened clavicle fracture. The patient Management of clavicle fractures continues to evolve. provided written informed consent for print and elec- Indications for operative management seem to be tronic publication of this case report. expanding, particularly in athletic youth. Surgical inter- vention has potential complications, many associated ASE EPORT with use of metal implants. To my knowledge, this case C R report is the first to describe use of a biodegradable A right-handed, 17-year-old girl injured her left shoulder implant. The subcutaneous position of the clavicle makes and right wrist in a fall from a mountain bike. Initial it ideal for fixation with a biodegradable implant in which management at an outside emergency department con- no second surgery is required for implant removal. sisted of a simple sling for a left midshaft clavicle fracture (Figure 1) and a volar wrist splint for a right comminuted intra-articular distal radius fracture. One day later, the he shoulder, the most mobile joint in the body, patient received a univalved short arm cast with appro- is prone to instability and injury. Due to the priate molding and underwent computed tomography for subcutaneous and relatively anterior location, the intra-articular fracture. No tenting of the skin over and because its thin midshaft lacks muscular the clavicle was noted during this visit to our facility. Tand ligamentous support, the clavicle is a common injury Sixteen days after injury, the distal radius fracture site. -

Imaging and Treatment of Scaphoid Fractures and Their Complications
159 Imaging and Treatment of Scaphoid Fractures and Their Complications Mihra S. Taljanovic, M.D., M.Sc., F.A.C.R. 1 Apostolos Karantanas, M.D., Ph.D. 2, 3 James F. Griffith, M.D. 4 Gregory L. DeSilva, M.D. 5 Joshua D. Rieke, M.D. 1 Joseph E. Sheppard, M.D. 5 1 Department of Medical Imaging, The University of Arizona Health Address for correspondence and reprint requests Mihra S. Taljanovic, Network, Tucson, Arizona. M.D., M.Sc., Department of Medical Imaging, The University of Arizona 2 Department of Radiology, University of Crete, Heraklion, Greece. Health Network, 1501 N. Campbell Ave., Tucson, AZ 85724-5067 3 Department of Medical Imaging, University Hospital, Heraklion, (e-mail: [email protected]). Greece. 4 Department of Imaging and Interventional Radiology, Prince of Wales Hospital, Shatin, New Territories, Hong Kong. 5 Department of Orthopaedic Surgery, The University of Arizona Health Network, Tucson, Arizona. Semin Musculoskelet Radiol 2012;16:159–174. Abstract The scaphoid is the most commonly fractured carpal bone, with frequent complications that are predisposed by its anatomical location, anatomical configuration (shape and length), and vascular supply. The most common mechanism of injury is a fall onto an outstretched hand. Imaging plays a significant role in the initial evaluation and treatment of scaphoid fractures and their complications. Radiography should be the first imaging modality in the initial evaluation and follow-up of scaphoid fractures. Computed tomography with its superb spatial resolution enables better visualization and charac- terization of the fracture line, and the amount of displacement and angulation of the fracture fragments. -

Section J: Trauma J
Section J: Trauma J Clinical/Diagnostic Investigation Recommendation Dose Comment Problem (Grade) Head J01. Head injury SXR Not indicated [B] d There is poor correlation between the presence of a skull fracture and a clinically significant head injury. The only (For children see indications for skull x-rays in the setting of trauma are Section L) suspected open or depressed skull fractures, if CT is not available and suspected child abuse. Section J: Trauma CT Indicated [A] dd CT is indicated in all patients with a severe head injury (GCS <13). In patients with a minor head injury (GCS 13-15 and witnessed loss of consciousness or disorientation or definite amnesia) CT is indicated to rule out an injury requiring neurosurgical intervention if there is: • GCS <15 2 hours after the injury • Suspected open or depressed skull fracture • Any sign of a basal skull fracture • Two or more episodes of vomiting • Age > 65 years To rule out any other clinically significant intracranial injury, the following additional risk factors justify obtaining CT: • Amnesia for before the impact lasting > 30 minutes • Dangerous mechanism of injury (motor vehicle accident or fall from> 3 feet or 5 stairs or more). CTA Specialized dd CTA should be performed with presentation of high energy Investigation [B] transfer mechanism or if associated with any of the following: • Displaced mid-face fracture • Basilar skull fracture with carotid canal involvement • Focal neurological deficit • Cervical vertebral body or transverse foramen fracture • Fracture at C1-C3 • Clothesline type injury or seat belt abrasion with significant swelling/pain • Altered mental status Face and orbits J02.