Clavicle Fractures George M
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Altered Alignment of the Shoulder Girdle and Cervical Spine in Patients with Insidious Onset Neck Pain and Whiplash- Associated Disorder
Journal of Applied Biomechanics, 2011, 27, 181-191 © 2011 Human Kinetics, Inc. Altered Alignment of the Shoulder Girdle and Cervical Spine in Patients With Insidious Onset Neck Pain and Whiplash- Associated Disorder Harpa Helgadottir, Eythor Kristjansson, Sarah Mottram, Andrew Karduna, and Halldor Jonsson, Jr. Clinical theory suggests that altered alignment of the shoulder girdle has the potential to create or sustain symptomatic mechanical dysfunction in the cervical and thoracic spine. The alignment of the shoulder girdle is described by two clavicle rotations, i.e, elevation and retraction, and by three scapular rotations, i.e., upward rotation, internal rotation, and anterior tilt. Elevation and retraction have until now been assessed only in patients with neck pain. The aim of the study was to determine whether there is a pattern of altered alignment of the shoulder girdle and the cervical and thoracic spine in patients with neck pain. A three-dimensional device measured clavicle and scapular orientation, and cervical and thoracic alignment in patients with insidious onset neck pain (IONP) and whiplash-associated disorder (WAD). An asymptomatic control group was selected for baseline measurements. The symptomatic groups revealed a significantly reduced clavicle retraction and scapular upward rotation as well as decreased cranial angle. A difference was found between the symptomatic groups on the left side, whereas the WAD group revealed an increased scapular anterior tilt and the IONP group a decreased clavicle elevation. These changes may be an important mechanism for maintenance and recurrence or exacerbation of symptoms in patients with neck pain. Keywords: neck pain, whiplash, scapula, posture Clinical theory suggests that altered alignment of of Biomechanics. -

Midshaft Clavicle Fracture
You have a Midshaft Clavicle Fracture This is a break to the middle of your collar bone. Healing: It normally takes 6-12 weeks to heal, but symptoms can continue for 3-6 months. Smoking will slow down your healing. We would advise that you stop smoking while your fracture heals. Talk to your GP or go to www.smokefree.nhs.uk for more information. Pain and Swelling: Your shoulder may be swollen and you will have some pain. Taking pain medication and using ice or cold packs will help. More information is on the next page. Wearing your sling: Use your sling for 3 weeks. You can take it off to wash, dress and do your exercises. It does not need to be worn at night. Exercise and activity: It is important to start gentle exercises straight away to prevent stiffness. You will find pictures and instructions for your exercises below. You should not do any heavy lifting or overhead movement for the first 6 weeks. Follow up: You will see a shoulder specialist 3 weeks after your injury. They may do another x-ray to check the position of your fracture. They will explain the next stage of your rehabilitation. If you have not received your appointment letter within 1 week, please contact us. Contact us: If you are concerned about your symptoms, are unable to follow this rehabilitation plan or notice pain other than at your shoulder, please contact the Virtual Fracture Clinic. Updated 9th June 2021 Caring for your injury: Weeks 1-3 Remember to use your sling for the first 3 weeks. -

Comparison of Four Different Internal Fixation Methods in the Treatment of Distal Clavicle Fractures
EXPERIMENTAL AND THERAPEUTIC MEDICINE 19: 451-458, 2020 Comparison of four different internal fixation methods in the treatment of distal clavicle fractures LIANG LI*, HONGXIAO WU*, PEICHAO JIANG, XIAOCHUAN HAN, SHIYUAN CHEN and XUEZHONG YU Department of Orthopaedics, Dongying People's Hospital, Dongying, Shandong 257091, P.R. China Received March 15, 2019; Accepted August 8, 2019 DOI: 10.3892/etm.2019.8233 Abstract. This study compared the clinical efficacy of four of shoulder pain, an increase in the range of motion of the internal fixation methods in the treatment of distal clavicle shoulder, and a reduction in complications, and thus, are pref- fractures, in an effort to guide appropriate selection and erable for the early functional recovery of limbs. application in the clinic. Eighty‑four patients with distal clav- icle‑comminuted fractures were treated with a distal clavicle Introduction anatomic plate (group A), clavicular hook plate (group B), double‑plate vertical fixation (group C), or T‑shaped steel Due to its subcutaneous location, clavicle is one of the bones plate internal fixation (group D). The Constant‑Murley scoring that are most frequently fractured in the upper body due to car system was used to evaluate the shoulder joint function. The accidents and sports trauma. The incidence of distal clavicle fracture healing time, VAS, and postoperative complications fractures accounts for 12‑21% of all clavicular fractures (1). were compared and analyzed among the four groups. According Distal clavicle fractures are typically attributed to a direct to the Constant‑Murley evaluation standard, the excellent and blow to the point of the shoulder or a fall on an outstretched good rates of the four groups were 94.4, 73.1, 95 and 80% hand. -

The Appendicular Skeleton Appendicular Skeleton
THE SKELETAL SYSTEM: THE APPENDICULAR SKELETON APPENDICULAR SKELETON The primary function is movement It includes bones of the upper and lower limbs Girdles attach the limbs to the axial skeleton SKELETON OF THE UPPER LIMB Each upper limb has 32 bones Two separate regions 1. The pectoral (shoulder) girdle (2 bones) 2. The free part (30 bones) THE PECTORAL (OR SHOULDER) GIRDLE UPPER LIMB The pectoral girdle consists of two bones, the scapula and the clavicle The free part has 30 bones 1 humerus (arm) 1 ulna (forearm) 1 radius (forearm) 8 carpals (wrist) 19 metacarpal and phalanges (hand) PECTORAL GIRDLE - CLAVICLE The clavicle is “S” shaped The medial end articulates with the manubrium of the sternum forming the sternoclavicular joint The lateral end articulates with the acromion forming the acromioclavicular joint THE CLAVICLE PECTORAL GIRDLE - CLAVICLE The clavicle is convex in shape anteriorly near the sternal junction The clavicle is concave anteriorly on its lateral edge near the acromion CLINICAL CONNECTION - FRACTURED CLAVICLE A fall on an outstretched arm (F.O.O.S.H.) injury can lead to a fractured clavicle The clavicle is weakest at the junction of the two curves Forces are generated through the upper limb to the trunk during a fall Therefore, most breaks occur approximately in the middle of the clavicle PECTORAL GIRDLE - SCAPULA Also called the shoulder blade Triangular in shape Most notable features include the spine, acromion, coracoid process and the glenoid cavity FEATURES ON THE SCAPULA Spine - -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Complications Associated with Clavicular Fracture
NOR200061.qxd 9/11/09 1:23 PM Page 217 Complications Associated With Clavicular Fracture George Mouzopoulos ▼ Emmanuil Morakis ▼ Michalis Stamatakos ▼ Mathaios Tzurbakis The objective of our literature review was to inform or- subclavian vein, due to its stable connection with the thopaedic nurses about the complications of clavicular frac- clavicle via the cervical fascia, can also be subjected to ture, which are easily misdiagnosed. For this purpose, we injuries (Casbas et al., 2005). Damage to the internal searched MEDLINE (1965–2005) using the key words clavicle, jugular vein, the suprascapular artery, the axillary, and fracture, and complications. Fractures of the clavicle are usu- carotid artery after a clavicular fracture has also been ally thought to be easily managed by symptomatic treatment reported (Katras et al., 2001). About 50% of injuries to the subclavian arteries are in a broad arm sling. However, it is well recognized that not due to fractures of the clavicle because the proximal all clavicular fractures have a good outcome. Displaced or part is dislocated superiorly by the sternocleidomas- comminuted clavicle fractures are associated with complica- toid, causing damage to the vessel (Sodhi, Arora, & tions such as subclavian vessels injury, hemopneumothorax, Khandelwal, 2007). If no injury happens during the ini- brachial plexus paresis, nonunion, malunion, posttraumatic tial displacement of the fractured part, then it is un- arthritis, refracture, and other complications related to os- likely to happen later, because the distal segment is dis- teosynthesis. Herein, we describe what the orthopaedic nurse placed downward and forward due to shoulder weight, should know about the complications of clavicular fractures. -

Medial Clavicle Fracture Dislocation Surgically Treated: Case Report Miguel Frias*, Renato Ramos, Marco Bernardes, Tiago Pinheiro Torres and Pedro Lourenço
ISSN: 2469-5777 Frias et al. Trauma Cases Rev 2018, 4:066 DOI: 10.23937/2469-5777/1510066 Volume 4 | Issue 2 Trauma Cases and Reviews Open Access CASE REPORT Medial Clavicle Fracture Dislocation Surgically Treated: Case Report Miguel Frias*, Renato Ramos, Marco Bernardes, Tiago Pinheiro Torres and Pedro Lourenço Centro Hospitalar de Vila Nova de Gaia/Espinho, Portugal *Corresponding author: Miguel Frias, Centro Hospitalar de Vila Nova de Gaia/Espinho, Porto, Portugal Check for updates injury to the trachea and esophagus and the possibility Abstract of pneumothorax [7]. The medial clavicle fracture is a rare injury and almost all the times conservatively treated. Therefore, the number of Although rare, such injuries require rapid diagnosis operations reported in the literature are limited. Posterior followed by effective treatment to avoid future dislocation can result in serious complications and such complications [8]. Specifically, periarticular and injuries require rapid diagnosis followed by effective treat- ment to avoid future complications. The present case re- intraarticular fractures remain a therapeutic challenge: ports a case of a 33-year-old healthy man that was involved The medial fragment is too small to stabilize with in a high-fall, being diagnosed with a rare displaced medi- common linear implants, and bending forces that occur al clavicular fracture associated with an unstable posterior during shoulder motion are disproportionately high lateral fragment dislocation surgically treated. Imagiological images and intraoperative photographs are presented. The [9]. Indications for surgery have traditionally included authors collected this case in order to report this rare and open fractures, soft-tissue damage, or neurovascular complex injury. -

Right Or Left Bones? Clavicle Ulna
Right or Left Bones? Clavicle Ulna . Together, the clavicles make a . Lay the ulna on the table. “handlebar” shape (low at the middle . Can you see the radial notch? of the chest, higher near the shoulders). o If yes, the open side of the . The blunt tip (sternal end) touches the trochlear (semilunar) notch tells sternum at the middle of the chest. you the bone orientation (see . The round tip (acromial end) touches the photo 1). scapula at the shoulder. o If no, the open side of the . The bumpy side of the clavicle faces the trochlear (semilunar) notch is the rib cage. opposite of the bone orientation . The smooth side of the clavicle faces (see photo 2). outward Radius Fibula . The styloid process always touches the . The smoother tip (head of the fibula) thumb. touches the knee. If the lower end of the radius (near the . The rougher tip (lateral malleolus) styloid process) is rough, you are touches the ankle. looking at the back of the wrist. The point of the lateral malleolus points . If the lower end of the radius is smooth, to the pinkie toe, not the middle of the you are looking at the inside of the wrist. foot. The front of the fibula (anterior view) has an edge. The back of the fibula (posterior view) is flat. References: University of Liverpool Faculty of Health and Life Sciences. (2013). Radius and ulna (right forearm) [Digital photograph]. Retrieved from https://www.flickr.com/photos/liverpoolhls/10819145494. . -
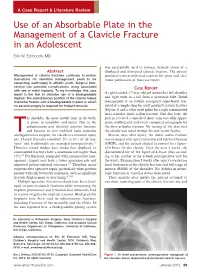
Use of an Absorbable Plate in the Management of a Clavicle Fracture in an Adolescent
A Case Report & Literature Review Use of an Absorbable Plate in the Management of a Clavicle Fracture in an Adolescent Eric W. Edmonds, MD was successfully used to manage delayed union of a Abstract displaced and shortened clavicle fracture. The patient Management of clavicle fractures continues to evolve. provided written informed consent for print and elec- Indications for operative management seem to be tronic publication of this case report. expanding, particularly in athletic youth. Surgical inter- vention has potential complications, many associated ASE EPORT with use of metal implants. To my knowledge, this case C R report is the first to describe use of a biodegradable A right-handed, 17-year-old girl injured her left shoulder implant. The subcutaneous position of the clavicle makes and right wrist in a fall from a mountain bike. Initial it ideal for fixation with a biodegradable implant in which management at an outside emergency department con- no second surgery is required for implant removal. sisted of a simple sling for a left midshaft clavicle fracture (Figure 1) and a volar wrist splint for a right comminuted intra-articular distal radius fracture. One day later, the he shoulder, the most mobile joint in the body, patient received a univalved short arm cast with appro- is prone to instability and injury. Due to the priate molding and underwent computed tomography for subcutaneous and relatively anterior location, the intra-articular fracture. No tenting of the skin over and because its thin midshaft lacks muscular the clavicle was noted during this visit to our facility. Tand ligamentous support, the clavicle is a common injury Sixteen days after injury, the distal radius fracture site. -

Rehabilitation Guidelines for Shoulder Debridement, Decompression and Distal Clavicle Excision
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Shoulder Debridement, Decompression and Distal Clavicle Excision Acromion Front View Back View Supraspinatus Supraspinatus Long head of bicep Type I Infraspinatus Short Teres head of bicep Minor Subscapularis Type II Front View Type III Figure 1 Shoulder anatomy Image Copyright 2010 UW Health Sports Medicine Center. Figure 2 Acromion classifications Subscapularis The shoulder is made up of three The rotator cuff connects the bones: the scapula (shoulder blade), humerus to the scapula. The rotator the humerus (upper arm bone) and cuff is formed by the tendons of the clavicle (collarbone). One part of four muscles: the supraspinatus, the scapula, called the glenoid fossa, infraspinatus, teres minor and is coupled with the humerus to Figure 3 Rotator cuff anatomy subscapularis (Figure 3). The stability make up the socket of the shoulder Image property of Primal Pictures, Ltd., primalpictures.com. Use and movement of the shoulder is of this image without authorization from Primal Pictures, Ltd. is (Figure 1). prohibited. controlled primarily by the rotator The glenoid is very shallow and cuff muscles, with assistance from may be performed using instruments flat. The glenoid labrum is a the ligaments, glenoid labrum and (about the size of a pencil which rim of soft tissue that turns the capsule of the shoulder. Labral include a camera and other surgical flat surface of the glenoid into a tears and rotator cuff tears are instruments) inserted through deeper socket that molds to fit often caused by a direct injury to small incisions in the shoulder, to the head of the humerus. -

Journal of Clinical Review & Case Reports
ISSN: 2573-9565 Case Report Journal of Clinical Review & Case Reports Eyes can’t See What the Mind doesn’t know - A case of Pneumothorax Complicating Clavicle Fracture Ahmed I¹,³*, Niaz Z², Kassem W³ and Nabeel M³ *Corresponding author Iftikhar Ahmed, Consultant, Aldara Hospital and Medical Centre, ¹University of the Southampton, UK Riyadh KSA, University of Southampton, UK Yardville Compound, 2 P.O. Box 1105 - Riyadh 11431 Tel: +966 (11) 420-7845, E-mail: Mayo Hospital, Lahore Pakistan [email protected] 3 Aldara Hospital and Medical Centre, Riyadh, KSA Submitted: 27 Dec 2017; Accepted: 03 Jan 2018; Published: 22 Jan 2018 Abstract Pneoumothorax is an infrequent but serious complication of clavicular fractures. The importance of its prompt recognition and management cannot be overstated. There have been few cases reported in medical literature (English+ Non-English) but all those patients had respiratory signs or symptoms at presentation. We hereby report a case of isolated clavicular fracture associated with pneumothorax where patient had no respiratory symptoms at the time of presentation and diagnosis was missed. This case highlights that clinical signs may be subtle initially, when attention is focused on obvious bony disruption. We advocate obtaining a routine chest x-ray in all patients with displaced clavicular fracture regardless of respiratory status. Keywords: Pneumothorax, Clavicular Fracture, Thoracocentesis the left clavicular region with painful shoulder movement. He was in no respiratory distress and his pulse, blood pressure, respirator Introduction rate and oxygen saturations were all within the normal range. His A pneumothorax refers to a collection of gas in the pleural space systemic examination was documented as unremarkable.