Utilisation of Accident and Emergency Services by Patients Who Could Be Managed by General Practitioners
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

LC Paper No. CB(2)2279/11-12(03)
LC Paper No. CB(2)2279/11-12(03) For discussion on 11 June 2012 Legislative Council Panel on Health Services Redevelopment of Kwong Wah Hospital Purpose This paper briefs Members on the proposed redevelopment of Kwong Wah Hospital (KWH). Background 2. At present, the Hospital Authority (HA) provides public hospital services for Sham Shui Po, Mongkok, Wong Tai Sin, Kwai Tsing, Tsuen Wan and North Lantau districts through its Kowloon West (KW) cluster, which comprises KWH, Caritas Medical Centre, Our Lady of Maryknoll Hospital, Wong Tai Sin Hospital, Kwai Chung Hospital, Princess Margaret Hospital and Yan Chai Hospital. KWH was established in 1911 and is a major acute hospital offering a comprehensive range of acute care services. Need for Redevelopment of KWH Aging Hospital Buildings 3. The majority of the KWH buildings is over 50 years old. With the passage of time, its space provision has become inadequate and building services installations out-dated. The structural conditions of the buildings have also been deteriorating. Being located in a densely populated area, KWH is one of the busiest hospitals of HA. The extremely heavy utilisation of KWH has also accelerated deterioration of its facilities. 4. Apart from the Tung Wah Group of Hospitals (TWGHs) Tsui Tsin Tong Out-patient Building (TTT OPB) which was built in 1999 and the Tung Wah Museum which is a declared monument built in 1911, the rest of the hospital buildings at KWH are old and in need of redevelopment. The Main Hospital Building was constructed in stages between 1959 and 1964. The Staff Barracks, Chinese Medicine Clinical Research and Services Centre, Nurses’ Quarters and Administration Building were all constructed in the 1960s and are in need of constant repairs. -

HA Go Activation Location
HA Go Activation Location Region Hospital Counter G/F, Block A Grantham Hospital G/F, Kwok Tak Seng Heart Centre G/F, Lo Fong Shiu Po Eye Centre MacLehose Medical 2/F, Specialist Out-Patient Clinic Rehabilitation Centre Registration Office, Department of Clinical Oncology (Out-Patient Clinic), LG1/F, East Block Pamela Youde Nethersole J7, Psychiatric Out-Patient Department, 7/F, East Block Eastern Hospital Central Registration Centre, G/F, Specialist Out-Patient Block J2, Psychiatric Specialist Out-Patient Clinic J5, Child & Adolescent Psychiatric Day Centre 3/F, Block S 4/F, Block S Queen Mary Hospital 5/F, Block S Hong 6/F, Block S Kong 7/F, Block S Island 3/F, South Wing, David Trench Rehabilitation Centre Registration Counter, G/F, Specialist Out-Patient Ruttonjee Hospital Department The Duchess of Kent Children's Hospital at Specialist Out-Patient Clinic, G/F, A Block Sandy Bay Registration Counter, Specalist Out-Patient Clinic, G/F, Tung Wah Eastern Main Block Hospital Counter, Eye Clinic, G/F, TWGHs Lo Ka Chow Memorial Ophthalmic Centre Tung Wah Group of Hospitals Fung Yiu King Geriatric Day Hospital Hospital C5, Day Centre Tung Wah Hospital H3, Specialist Out-Patient Clinic L4, Eye, Nose & Throat Centre Tsan Yuk Hospital G/F, The Specialist Outpatient Clinic (Obstetrics) 1 / 4 HA Go Activation Location Region Hospital Counter Room 37, Ophthalmic Centre, 2/F, Wai Ming Block Caritas Medical Centre Specialist Out-Patient Clinic, 3/F, Wai Ming Block Reception Office, 4/F, Wai Ming Block Hong Kong Buddhist Enquiry counter, Out-Patient -

New Territories
Branch ATM District Branch / ATM Address Voice Navigation ATM 1009 Kwai Chung Road, Kwai Chung, New Kwai Chung Road Branch P P Territories 7-11 Shek Yi Road, Sheung Kwai Chung, New Sheung Kwai Chung Branch P P P Territories 192-194 Hing Fong Road, Kwai Chung, New Ha Kwai Chung Branch P P P Territories Shop 102, G/F Commercial Centre No.1, Cheung Hong Estate Commercial Cheung Hong Estate, 12 Ching Hong Road, P P P P Centre Branch Tsing Yi, New Territories A18-20, G/F Kwai Chung Plaza, 7-11 Kwai Foo Kwai Chung Plaza Branch P P Road, Kwai Chung, New Territories Shop No. 114D, G/F, Cheung Fat Plaza, Cheung Fat Estate Branch P P P P Cheung Fat Estate, Tsing Yi, New Territories Shop 260-265, Metroplaza, 223 Hing Fong Metroplaza Branch P P Road, Kwai Chung, New Territories 40 Kwai Cheong Road, Kwai Chung, New Kwai Cheong Road Branch P P P P Territories Shop 115, Maritime Square, Tsing Yi Island, Maritime Square Branch P P New Territories Maritime Square Wealth Management Shop 309A-B, Level 3, Maritime Square, Tsing P P P Centre Yi, New Territories ATM No.1 at Open Space Opposite to Shop No.114, LG1, Multi-storey Commercial /Car Shek Yam Shopping Centre Park Accommodation(also known as Shek Yam Shopping Centre), Shek Yam Estate, 120 Lei Muk Road, Kwai Chung, New Territories. Shop No.202, 2/F, Cheung Hong Shopping Cheung Hong Estate Centre No.2, Cheung Hong Estate, 12 Ching P Hong Road, Tsing Yi, New Territories Shop No. -

Student Services Centre July 2017 Contents
Handbook For Non-local Degree-seeking Students Student Services Centre July 2017 Contents 1. PLANNING YOUR ARRIVAL P2 1.1 Important Dates 1.2 Things To Bring Along 1.3 Arrival Pick-up Service 2. Arrival and Orientation P5 2.1 Reporting and Hostel Check-in 2.2 Orientation 3. STUDYING AT LINGNAN P8 3.1 Course Registration 3.2 Graduation Requirements 3.3 Academic Support Services 4. FACILITIES AND STUDENT SERVICES P13 Facilities 4.1 Student Hostels 4.2 Dining Facilities 4.3 Sports Facilities 4.4 Chaplain’s Office 4.5 Prayer/ Meditation Room Student Services 4.6 Healthcare 4.7 Lingnan Host Family Scheme 4.8 Student Societies/ University Teams 4.9 Student Development Awards 5. FINANCIAL MATTERS P20 5.1 Bank Account, Automated Teller Machine and Credit Card 5.2 Expenses 5.3 Octopus Card 5.4 MTR Student Travel Scheme 6. LIVING IN HONG KONG P22 6.1 Hong Kong Identity Card 6.2 Internship / Part-time job 6.3 Weather and Clothing 6.4 Communication 7. COPING WITH A NEW CULTURE P26 7.1 Culture Shock 7.2 How do I Adjust and Cope with a New Culture 7.3 Tips on Adjustment from Senior Non-local Degree-seeking Students 8. APPENDICES P31 Appendix 1 Contacts of University Units/ Campus Facilities Appendix 2 Useful Contacts in Hong Kong Appendix 3.1 Transportation from Shen Zhen Airport / Lo Wu Railway Station to Lingnan University Appendix 3.2 Transportation from Hong Kong International Airport to Lingnan University Appendix 4 Mass Transit Railway (MTR) Route Map Appendix 5 Campus Map P1 Planning Your Arrival 1.1 Important Dates In each academic year, there are three Terms: Term 1, Term 2 and Summer Term. -

LEGISLATIVE COUNCIL PANEL on TRANSPORT Progress Update on the Installation of Speed Enforcement Camera and Red Light Camera
CB(1)477/03-04(02) LEGISLATIVE COUNCIL PANEL ON TRANSPORT Progress Update on the Installation of Speed Enforcement Camera and Red Light Camera Systems Introduction This paper updates Members on the progress of the installation of speed enforcement camera and red light camera systems. Background Speed Enforcement Cameras 2. Driving in excess of speed limits on the road has contributed to the occurrence and severity of most traffic accidents. Overseas experience shows that installation of speed enforcement cameras (SECs) at strategic locations is a useful means to combat speeding effectively. 3. Before January 1999, there were only 10 locations along Tolo Highway and Fanling Highway that were installed with SEC on- site equipment. In January 1999, we consulted this Panel on our proposal to expand the coverage of SECs to 60 other locations at strategic roads and expressways, and to place eight cameras at these locations on a rotational basis. The funding requirement for the procurement of cameras and computer systems, installation works, testing of equipment and contingencies was estimated to be $25.16m. Members supported the proposal. We subsequently secured the Finance Committee (FC)’s funding approval for the project in July 1999. However, as the price of the successful bid was lower than our estimate, we decided to add another 15 locations to the project, then making a total of 75 locations. The project was scheduled to be completed by September 2002. The list of locations is at Annex A. - 2 - Red Light Cameras 4. The red light camera (RLC) system aims to deter drivers from red light jumping which accounts for more than 80% of traffic signal offences. -

Hospital Authority Special Visiting Arrangement in Hospitals/Units with Non-Acute Settings Under Emergency Response Level Notes to Visitors
Hospital Authority Special Visiting Arrangement in Hospitals/Units with Non-acute Settings under Emergency Response Level Notes to Visitors 1. Hospital Authority implemented special visiting arrangement in four phases on 21 April 2021, 29 May 2021, 25 June 2021 and 23 July 2021 respectively (as appended table). Cluster Hospitals/Units with non-acute settings Cheshire Home, Chung Hom Kok Ruttonjee Hospital Hong Kong East Mixed Infirmary and Convalescent Wards Cluster Tung Wah Eastern Hospital Wong Chuk Hang Hospital Grantham Hospital MacLehose Medical Rehabilitation Centre Hong Kong West The Duchess of Kent Children’s Hospital at Sandy Bay Cluster Tung Wah Group of Hospitals Fung Yiu King Hospital Tung Wah Hospital Kowloon East Haven of Hope Hospital Cluster Hong Kong Buddhist Hospital Kowloon Central Kowloon Hospital (Except Psychiatric Wards) Cluster Our Lady of Maryknoll Hospital Tung Wah Group of Hospitals Wong Tai Sin Hospital Caritas Medical Centre Developmental Disabilities Unit, Wai Yee Block Medical and Geriatrics/Orthopaedics Rehabilitation Wards and Palliative Care Ward, Wai Ming Block North Lantau Hospital Kowloon West Extended Care Wards Cluster Princess Margaret Hospital Lai King Building Yan Chai Hospital Orthopaedics and Traumatology Rehabilitation Ward and Medical Extended Care Unit (Rehabilitation and Infirmary Wards), Multi-services Complex New Territories Bradbury Hospice East Cluster Cheshire Home, Shatin North District Hospital 4B Convalescent Rehabilitation Ward Shatin Hospital (Except Psychiatric Wards) Tai Po Hospital (Except Psychiatric Wards) Pok Oi Hospital Tin Ka Ping Infirmary New Territories Siu Lam Hospital West Cluster Tuen Mun Hospital Rehabilitation Block (Except Day Wards) H1 Palliative Ward 2. Hospital staff will contact patients’ family members for explanation of special visiting arrangement and scheduling the visits. -
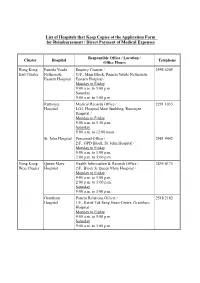
List of Hospitals That Keep Copies of the Application Form for Reimbursement / Direct Payment of Medical Expenses
List of Hospitals that Keep Copies of the Application Form for Reimbursement / Direct Payment of Medical Expenses Responsible Office / Location / Cluster Hospital Telephone Office Hours Hong Kong Pamela Youde Enquiry Counter / 2595 6205 East Cluster Nethersole G/F., Main Block, Pamela Youde Nethersole Eastern Hospital Eastern Hospital / Monday to Friday 9:00 a.m. to 5:00 p.m. Saturday 9:00 a.m. to 1:00 p.m. Ruttonjee Medical Records Office / 2291 1035 Hospital LG1, Hospital Main Building, Ruttonjee Hospital / Monday to Friday 9:00 a.m. to 5:30 p.m. Saturday 9:00 a.m. to 12:00 noon St. John Hospital Personnel Office / 2981 9442 2/F., OPD Block, St. John Hospital / Monday to Friday 9:00 a.m. to 1:00 p.m. 2:00 p.m. to 5:00 p.m. Hong Kong Queen Mary Health Information & Records Office / 2855 4175 West Cluster Hospital 2/F., Block S, Queen Mary Hospital / Monday to Friday 9:00 a.m. to 1:00 p.m. 2:00 p.m. to 5:00 p.m. Saturday 9:00 a.m. to 1:00 p.m. Grantham Patient Relations Officer / 2518 2182 Hospital 1/F., Kwok Tak Seng Heart Centre, Grantham Hospital / Monday to Friday 9:00 a.m. to 5:00 p.m. Saturday 9:00 a.m. to 1:00 p.m. - 2 - Responsible Office / Location / Cluster Hospital Telephone Office Hours Kowloon Kwong Wah Medical Report Office / 3517 5216 West Cluster Hospital 1/F., Central Stack, Kwong Wah Hospital / Monday to Friday 9:00 a.m. -

Hospital Authority List of Medical Social Services Units (January 2019)
Hospital Authority List of Medical Social Services Units (January 2019) Name of Hospital Address Tel No. Fax No. 1. Alice Ho Miu Ling Nethersole 11 Chuen On Road, Tai Po, N.T. 2689 2020 2662 3152 Hospital (Non- psychiatric medical social service) 2. Bradbury Hospital 17 A Kung Kok Shan Road, 2645 8832 2762 1518 Shatin, N.T. 3. Caritas Medical Centre 111 Wing Hong Street, 3408 7709 2785 3192 Shamshuipo, Kowloon 4. Cheshire Home 128 Chung Hom Kok Road, 2899 1391 2813 8752 (Chung Hom Kok) Hong Kong 5. Cheshire Home (Shatin) 30 A Kung Kok Shan Road, 2636 7269 2636 7242 Shatin, N.T. 6. TWGHs Fung Yiu King Hospital 9 Sandy Bay Road, Hong Kong 2855 6236 2904 9021 7. Grantham Hospital 125 Wong Chuk Hang Road, 2518 2678 2580 7629 Aberdeen, Hong Kong 8. Haven of Hope Hospital 8 Haven of Hope Road, 2703 8227 2703 8230 Tseung Kwan O, Kowloon 9. Hong Kong Buddhist Hospital 10 Heng Lam Road, Lok Fu, 2339 6253 2339 6298 Kowloon 10. Kowloon Hospital Mezzanine Floor, Kowloon 3129 7806/ 3129 7838 (Ward 2B at Rehabilitation Hospital Rehabilitation Building, 3129 7831 Building ) 147A, Argyle Street, Kowloon 11. Kwong Wah Hospital 25 Waterloo Road, Kowloon 3517 2900 3517 2959 12. MacLehose Medical 7 Sha Wan Drive, 2872 7131 2872 7909 Rehabilitation Centre Pokfulam, Hong Kong Name of Hospital Address Tel No. Fax No. 13. Our Lady of Maryknoll Hospital 118 Shatin Pass Road, 2354 2285 2324 8719 Wong Tai Sin, Kowloon 14. Pok Oi Hospital Au Tau, Yuen Long, N.T. 2486 8140 2486 8095 2486 8141 15. -
Chapter 7: Healthcare in Hong Kong
Chapter 7: Healthcare in Hong Kong The Hong Kong Hospital Authority The Hong Kong Hospital Authority (HA) is responsible for managing all local public hospitals in Hong Kong. Staff of the HA can communicate in Chinese (mainly the Cantonese dialect) and / or English. If interpretation is needed for other languages, the HA will use reasonable endeavours to arrange for patients free interpretation services provided by third parties / consulates. Information about the HA, including the contact details of public hospitals, can be found on its website at www.ha.org.hk.Information on Accident and Emergency Departments and General Out-patient Clinics is also available in eight other languages, namely Bahasa Indonesian, Hindi, Nepali, Punjabi (Indian), Punjabi (Pakistani), Tagalog, Thai, Urdu on the website. Accident & Emergency services The Accident & Emergency (A&E) services are provided at 18 public hospitals under the HA. They deliver a high standard of service for critically ill or injured persons who need urgent medical attention. They also provide medical support for victims of disasters. To ensure that patients with more serious conditions are accorded higher priority in medical treatment, the HA adopts a triage system which classifies patients attending the A&E Departments into five categories according to their clinical conditions: critical, emergency, urgent, semi-urgent or non-urgent. Patients who do not require emergency attendance should seek medical treatment in public or private clinics. Hospital Address Telephone Service Hours Alice Ho Miu Ling 11 Chuen On Road 2689-2000 Nethersole Hospital Tai Po, NT Caritas Medical 111 Wing Hong Street 3408-7911 24 hours Centre Sham Shui Po, Kowloon KwongWah 25 Waterloo Road, Kowloon 2332-2311 Hospital 46 Chapter 7 North District 9 Po Kin Road 2683-8888 Hospital Sheung Shui, NT North Lantau 1/F, 8 Chung Yan Road 3467-7000 Hospital Tung Chung, Lantau, N.T. -

Master of Science in Marketing and International Business
Master of Science in Marketing and International Business STUDENT HANDBOOK 2020/21 2 3 TABLE OF CONTENTS 1. About Lingnan University ...............................................................................................7 1.1 Vision, Mission and Core Values ...................................................................................8 1.2 Graduate Attributes for Taught Postgraduate (TPg) Programmes .............................9 2 Programme Information .............................................................................................. 10 2.1 Background .................................................................................................................. 10 2.2 Aims and Learning Goals ............................................................................................ 10 2.3 Entrance Requirements .............................................................................................. 11 2.4 Mode of Study ............................................................................................................. 11 2.5 Normal and Maximum Duration of Study .................................................................. 11 2.6 Medium of Instruction ................................................................................................. 11 2.7 Contributing Departments /Units/External Partners ................................................. 11 2.8 Programme Structure .................................................................................................. 12 2.8.1 Curriculum..................................................................................................... -

Methodological Study on the Evaluation of Face Mask Use Scale Among Public Adult: Cross-Language and Psychometric Testing
Korean Journal of Adult Nursing eISSN 2288-338X Vol. 32 No. 1, 46-56, February 2020 https://doi.org/10.7475/kjan.2020.32.1.46 ORIGINAL ARTICLE Open Access Methodological Study on the Evaluation of Face Mask Use Scale among Public Adult: Cross-Language and Psychometric Testing Lam, Simon Ching1 · Chong, Andy Chun Yin2 · Chung, Jessie Yuk Seng2 · Lam, Ming Yee3 · Chan, Lai Man4 · Shum, Cho Yee5 · Wong, Eliza Yi Ni5 · Mok, Yat Man6 · Lam, Ming Tat7 · Chan, Man Man5 · Tong, Ka Ying8 · Chu, Oi Lee5 · Siu, Fong Kiu4 · Cheung, Jamie Hau Man9 1Assistant Professor, School of Nursing, The Hong Kong Polytechnic University, Hong Kong SAR 2Senior Lecturer, School of Nursing and Health Studies, The Open University of Hong Kong, Hong Kong SAR 3Registered Nurse, Yan Chai Hospital, Hospital Authority, Hong Kong SAR 4Registered Nurse, Caritas Medical Center, Hospital Authority, Hong Kong SAR 5Registered Nurse, Prince of Wales Hospital, Hospital Authority, Hong Kong SAR 6Registered Nurse, Ruttonjee Hospital, Hospital Authority, Hong Kong SAR 7Registered Nurse, Queen Mary Hospital, Hospital Authority, Hong Kong SAR 8Registered Nurse, St. Paul's Hospital, Hong Kong Island, Hong Kong SAR 9Registered Nurse, Department of Health, Hong Kong SAR Purpose: This study aimed to establish the translation adequacy and examine the psychometric properties of Face Mask Use Scale (FMUS). Methods: This methodological study employed a cross-sectional design with repeated measures. Phase 1 examined the equivalence and relevance of English and Chinese versions of FMUS. Phase 2 examined the internal consistency, stability and construct validity. Different sample batches (213 university students and 971 general public) were used appropriately for psychometric testing. -

List of Medical Social Services Units Under Social Welfare Department
List of Medical Social Services Units Under Social Welfare Department Hong Kong Name of Hospital/Clinic Tel. No. Email Address 1. Queen Mary Hospital 2255 3762 [email protected] 2255 3764 2. Wong Chuk Hang Hospital 2873 7201 [email protected] 3. Pamela Youde Nethersole Eastern 2595 6262 [email protected] Hospital 4. Pamela Youde Nethersole Eastern 2595 6773 [email protected] Hospital (Psychiatric Department) Kowloon Name of Hospital/Clinic Tel. No. Email Address 5. Tseung Kwan O Hospital 2208 0335 [email protected] 2208 0327 6. United Christian Hospital 3949 5178 [email protected] (Psychiatry) 7. Queen Elizabeth Hospital 3506 7021 [email protected] 3506 7027 3506 5499 3506 4021 8. Hong Kong Eye Hospital 2762 3069 [email protected] 9. Kowloon Hospital Rehabilitation 3129 7857 [email protected] Building 10. Kowloon Hospital 3129 6193 [email protected] 11. Kowloon Hospital 2768 8534 [email protected] (Psychiatric Department) 1 The New Territories Name of Hospital/Clinic Tel. No. Email Address 12. Prince of Wales Hospital 3505 2400 [email protected] 13. Shatin Hospital 3919 7521 [email protected] 14. Tai Po Hospital 2607 6304 [email protected] Sub-office Tai Po Hospital (Child and Adolescent 2689 2486 [email protected] Mental Health Centre) 15. North District Hospital 2683 7750 [email protected] 16. Tin Shui Wai Hospital 3513 5391 [email protected] 17. Castle Peak Hospital 2456 7401 [email protected] 18. Siu Lam Hospital 2456 7186 [email protected] 19.