Simplified Signs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bird Trip Report, 11-12 March 2017 BIRDING in BRASSO SECO by Matt Kelly
Quarterly Bulletin of the Trinidad and Tobago Field Naturalists’ Club April – June 2017 Issue No: 2/2017 Bird Trip Report, 11-12 March 2017 BIRDING IN BRASSO SECO by Matt Kelly Selwyn Gomes and I left Port of Spain Community Museum in Arima, which was very at 7:30am on Saturday, March 11, 2017 and interesting. To do justice, an entire article needs to headed over the Northern Range for Brasso be devoted to that community. Seco. We meandered a bit along the way, first stopping at the Santa Rosa First Peoples’ (Continued on page 3) Male tufted coquette Photo by Matt Kelly Page 2 THE FIELD NATURALIST Issue No. 2/2017 Inside This Issue BIRD TRIP REPORT 1 BRASSO SECO Quarterly Bulletin of the - Matt Kelly Trinidad and Tobago Field Naturalists’ Club 50 YEARS OF AWNC April - June 2017 5 - Johanne Ryan Editors 8 IF YOU’VE GOT, IT FLAUNT IT Amy Deacon, Renoir Auguste, -Christopher K. Starr Associate Editor: Rupert Mends ‘NATURALIST IN’ SERIES Contributing writers BETWEEN ATLANTIC TIDES 9 Jessica Rozek, Christopher K. Starr, Hans Boos, Kris Sookdeo, - Christopher K Starr Renoir Auguste, Matt Kelly, Feroze Omardeen, Reynold Boyce, Johanne Ryan BIRD GROUP REPORT 11 GRAND COUVA Photographs - Matt Kelly Jessica Rozek, Aly Olliviere, Jeffrey Wong Sang, 13 YOUR IDEAS AND OBSERVATIONS Hans Boos, Kris Sookdeo, Christopher K. Starr, Renoir Auguste, Matt Kelly, Faraaz Abdool, Feroze Omardeen, Asif FIELD TRIP REPORT Khan, Kenneth Fournillier, Harold Diaz. 14 COCOA ESTATE AT FISHING POND - Reynold Boyce Design and Layout 16 CONFERENCE REPORT Eddison Baptiste and Amy Deacon CELEBRATING CARIBBEAN BIRD DIVERSITY - Jessica Rozek 18 STRATEGIC PLAN UPDATE - Compiled by Amy Deacon 19 ‘YOU SHOULDN’T BE IN SCHOOL’ The Trinidad and Tobago Field Naturalists’ Club Presentation of Elisha Tikasingh’s Memoirs is a non-profit, non-governmental organization 20 NATURE IN THE NEWS Management Committee 2017/2018 Compiled by Kris Sookdeo President …………….. -

Sign Language Typology Series
SIGN LANGUAGE TYPOLOGY SERIES The Sign Language Typology Series is dedicated to the comparative study of sign languages around the world. Individual or collective works that systematically explore typological variation across sign languages are the focus of this series, with particular emphasis on undocumented, underdescribed and endangered sign languages. The scope of the series primarily includes cross-linguistic studies of grammatical domains across a larger or smaller sample of sign languages, but also encompasses the study of individual sign languages from a typological perspective and comparison between signed and spoken languages in terms of language modality, as well as theoretical and methodological contributions to sign language typology. Interrogative and Negative Constructions in Sign Languages Edited by Ulrike Zeshan Sign Language Typology Series No. 1 / Interrogative and negative constructions in sign languages / Ulrike Zeshan (ed.) / Nijmegen: Ishara Press 2006. ISBN-10: 90-8656-001-6 ISBN-13: 978-90-8656-001-1 © Ishara Press Stichting DEF Wundtlaan 1 6525XD Nijmegen The Netherlands Fax: +31-24-3521213 email: [email protected] http://ishara.def-intl.org Cover design: Sibaji Panda Printed in the Netherlands First published 2006 Catalogue copy of this book available at Depot van Nederlandse Publicaties, Koninklijke Bibliotheek, Den Haag (www.kb.nl/depot) To the deaf pioneers in developing countries who have inspired all my work Contents Preface........................................................................................................10 -

Anastasia Bauer the Use of Signing Space in a Shared Signing Language of Australia Sign Language Typology 5
Anastasia Bauer The Use of Signing Space in a Shared Signing Language of Australia Sign Language Typology 5 Editors Marie Coppola Onno Crasborn Ulrike Zeshan Editorial board Sam Lutalo-Kiingi Irit Meir Ronice Müller de Quadros Roland Pfau Adam Schembri Gladys Tang Erin Wilkinson Jun Hui Yang De Gruyter Mouton · Ishara Press The Use of Signing Space in a Shared Sign Language of Australia by Anastasia Bauer De Gruyter Mouton · Ishara Press ISBN 978-1-61451-733-7 e-ISBN 978-1-61451-547-0 ISSN 2192-5186 e-ISSN 2192-5194 Library of Congress Cataloging-in-Publication Data A CIP catalog record for this book has been applied for at the Library of Congress. Bibliographic information published by the Deutsche Nationalbibliothek The Deutsche Nationalbibliothek lists this publication in the Deutsche Nationalbibliografie; detailed bibliographic data are available on the Internet at http://dnb.dnb.de. ” 2014 Walter de Gruyter, Inc., Boston/Berlin and Ishara Press, Lancaster, United Kingdom Printing and binding: CPI books GmbH, Leck Țȍ Printed on acid-free paper Printed in Germany www.degruyter.com Acknowledgements This book is the revised and edited version of my doctoral dissertation that I defended at the Faculty of Arts and Humanities of the University of Cologne, Germany in January 2013. It is the result of many experiences I have encoun- tered from dozens of remarkable individuals who I wish to acknowledge. First of all, this study would have been simply impossible without its partici- pants. The data that form the basis of this book I owe entirely to my Yolngu family who taught me with patience and care about this wonderful Yolngu language. -
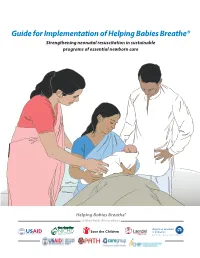
Guide for Implementation of Helping Babies Breathe®
Guide for Implementation of Helping Babies Breathe® Strengthening neonatal resuscitation in sustainable programs of essential newborn care Guide for Implementation of Helping Babies Breathe® (HBB): Strengthening neonatal resuscitation in sustainable programs of essential newborn care. 2011. Elk Grove Village, IL: American Academy of Pediatrics Helping Babies Breathe® (HBB) aims to help meet Millennium Development Goal 4 targets for reduction of child mortality by addressing one of the most important causes of neonatal death: intrapartum-related events (birth asphyxia). HBB is an evidence-based educational program which teaches the simple steps that effectively resuscitate the majority of infants not breathing at birth. Helping Babies Breathe is designed to coordinate with other interventions in a package selected to improve neonatal and maternal health. HBB can be used as the resuscitation component in courses teaching Essential Newborn Care (WHO) and courses in midwifery skills. HBB can be used at all levels in the health system. It extends resuscitation training to first-level health facilities and health workers in resource-limited settings, where these skills are most lacking. It also can be used in higher-level health facilities, including tertiary facilities, where it complements, but does not replace, comprehensive resuscitation programs such as the Neonatal Resuscitation Program (NRP). Both HBB and NRP teach the same first steps in resuscitation, but NRP also includes the use of supplemental oxygen, chest compressions, intubation, and medications. HBB uses a learner-centered educational methodology with emphasis on mastery of key skills. Pictorial, color-coded print materials and a low-cost, high-fidelity neonatal simulator engage learners and empower them to continue learning in the workplace. -

UC Berkeley Dissertations, Department of Linguistics
UC Berkeley Dissertations, Department of Linguistics Title Politeness in Japanese Sign Language (JSL): Polite JSL Expression as Evidence for Intermodal Language Contact Influence Permalink https://escholarship.org/uc/item/4jq1v247 Author George, Johnny Publication Date 2011 eScholarship.org Powered by the California Digital Library University of California Politeness in Japanese Sign Language (JSL): Polite JSL expression as evidence for intermodal language contact influence By Johnny Earl George A dissertation submitted in partial satisfaction of the requirements for the degree of Doctor of Philosophy in LINGUISTICS in the GRADUATE DIVISION of the UNIVERSITY OF CALIFORNIA, BERKELEY Committee in charge: Professor Eve Sweetser, Chair Professor Sharon Inkelas Professor Yoko Hasegawa Fall 2011 Politeness in Japanese Sign Language (JSL): Polite JSL expression as evidence for intermodal language contact influence © 2011 by Johnny Earl George 1 ABSTRACT Politeness in Japanese Sign Language (JSL): Polite JSL expression as evidence for intermodal language contact influence by Johnny Earl George Doctor of Philosophy in Linguistics University of California, Berkeley Professor Eve Sweetser, Chair This dissertation shows how signers mark polite register in JSL and uncovers a number of features salient to the linguistic encoding of politeness. My investigation of JSL politeness considers the relationship between Japanese sign and speech and how users of these languages adapt their communicative style based on the social context. This work examines: the Deaf Japanese community as minority language users and the concomitant effects on the development of JSL; politeness in JSL independently and in relation to spoken Japanese, along with the subsequent implications for characterizing polite Japanese communicative interaction; and the results of two studies that provide descriptions of the ways in which JSL users linguistically encode polite register. -

Higher Education in China, a Paradigm Shift from Conventional to Online Teaching
Higher Education Studies; Vol. 11, No. 2; 2021 ISSN 1925-4741 E-ISSN 1925-475X Published by Canadian Center of Science and Education Higher Education in China, a Paradigm Shift from Conventional to Online Teaching Wang He1, 2, 3 & Gao Wei4, 5 1 DBA Candidate of University of Wales Trinity Saint David London Campus, UK 2 Vice President, Hankou University, Wuhan, China 3 Associate Professor & Dean of College of Media, Hankou University, Wuhan, China 4 PhD Candidate, Wuhan University of Technology, China 5 Dean of College of International Exchange, Hankou University, Wuhan, China Correspondence: Gao Wei, Dean of College of International Exchange, Hankou University, Wuhan, China. E-mail: [email protected] Received: February 6, 2021 Accepted: March 4, 2021 Online Published: March 6, 2021 doi:10.5539/hes.v11n2p30 URL: https://doi.org/10.5539/hes.v11n2p30 Abstract The entire education system, from elementary school to higher education, distorted during the lockdown period. The latest 2019 coronavirus disease (COVID-19) is not only recorded in China, but also globally. This research is an account of the online teaching paradigm assumed in the teaching method by most of universities in China and subsequent tests over the course. It looks forward to offering resources rich in knowledge for future academic decision-making in any adversity. The aim of this research paper is to explain the prerequisites for online education and teaching during the COVID-19 pandemic and how to effectively turn formal education into online education through the use of virtual classrooms and other main online instruments in an ever-changing educational setting by leveraging existing educational tools. -

Review: Marcello Barbieri (Ed) (2007) Introduction to Biosemiotics. the New Biological Synthesis
tripleC 5(3): 104-109, 2007 ISSN 1726-670X http://tripleC.uti.at Review: Marcello Barbieri (Ed) (2007) Introduction to Biosemiotics. The new biological synthesis. Dordrecht: Springer Günther Witzany telos – Philosophische Praxis Vogelsangstr. 18c A-5111-Buermoos/Salzburg Austria E-mail: [email protected] 1 Thematic background without utterances we act as non-uttering indi- viduals being dependent on the discourse de- Maybe it is no chance that the discovery of the rived meaning processes of a linguistic (e.g. sci- genetic code occurred during the hot phase of entific) community. philosophy of science discourse about the role of This position marks the primary difference to language in generating models of scientific ex- the subject of knowledge of Kantian knowledge planation. The code-metaphor was introduced theories wherein one subject alone in principle parallel to other linguistic terms to denote lan- could be able to generate sentences in which it guage like features of the nucleic acid sequence generates knowledge. This abstractive fallacy molecules such as “code without commas” was ruled out in the early 50s of the last century (Francis Crick). At the same time the 30 years of being replaced by the “community of investiga- trying to establish an exact scientific language to tors” (Peirce) represented by the scientific com- delimit objective sentences from non-objective munity in which every single scientist is able the ones derived one of his peaks in the linguistic place his utterance looking for being integrated turn. in the discourse community in which his utter- ances will be proven whether they are good ar- 1.1 Changing subjects of knowledge guments or not. -

Persian Sign Gesture Translation to English Spoken Language on Smartphone
Published by : International Journal of Engineering Research & Technology (IJERT) http://www.ijert.org ISSN: 2278-0181 Vol. 9 Issue 06, June-2020 Persian Sign Gesture Translation to English Spoken Language on Smartphone Muhammad Reza Jafari Dr. Vinod Kumar Computer Science & Engineering Department Computer Science & Engineering Department Delhi Technological University (DTU) Delhi Technological University (DTU) Delhi, India Delhi, India Abstract — Hearing impaired and others with verbal Persian language is no exception. Figure 1 shows the Persian challenges face difficulty to communicate with society; Sign sign Language Alphabets. Language represents their communication such as numbers or phrases. The communication becomes a challenge with people from other countries using different languages. Additionally, the sign language is different from one country to another. That is, learning one sign language doesn’t mean learning all sign languages. To translate a word from sign language to a spoken language is a challenge and to change a particular word from that language to another language is even a bigger challenge. In such cases, there is necessity for 2 interpreters: One from sign language to the source-spoken language and one from the source language to the target language. There is ample research done on sign recognition, yet this paper focuses on translating gestures from one language to another. In this study, we are proposing the use of smartphone as a platform for Sign Language recognition, because smartphones are available worldwide. Smartphones are limited in computational power and we propose a system of client- server application where most of processing tasks are done on the server side. In client-server application system, client could be a smartphone application that captures images of sign gestures to be recognized and sent to a server. -

Hand-To-Hand Combat, Or Mouth-To-Mouth Resuscitation?
BEHAVIORAL AND BRAIN SCIENCES (2003) 26, 199–260 Printed in the United States of America From mouth to hand: Gesture, speech, and the evolution of right-handedness Michael C. Corballis Department of Psychology, University of Auckland, Private Bag 92019, Auckland, New Zealand. [email protected] Abstract: The strong predominance of right-handedness appears to be a uniquely human characteristic, whereas the left-cerebral dom- inance for vocalization occurs in many species, including frogs, birds, and mammals. Right-handedness may have arisen because of an association between manual gestures and vocalization in the evolution of language. I argue that language evolved from manual gestures, gradually incorporating vocal elements. The transition may be traced through changes in the function of Broca’s area. Its homologue in monkeys has nothing to do with vocal control, but contains the so-called “mirror neurons,” the code for both the production of manual reaching movements and the perception of the same movements performed by others. This system is bilateral in monkeys, but pre- dominantly left-hemispheric in humans, and in humans is involved with vocalization as well as manual actions. There is evidence that Broca’s area is enlarged on the left side in Homo habilis, suggesting that a link between gesture and vocalization may go back at least two million years, although other evidence suggests that speech may not have become fully autonomous until Homo sapiens appeared some 170,000 years ago, or perhaps even later. The removal of manual gesture as a necessary component of language may explain the rapid advance of technology, allowing late migrations of Homo sapiens from Africa to replace all other hominids in other parts of the world, including the Neanderthals in Europe and Homo erectus in Asia. -

Sign Language Ideologies: Practices and Politics
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Heriot Watt Pure Annelies Kusters, Mara Green, Erin Moriarty and Kristin Snoddon Sign language ideologies: Practices and politics While much research has taken place on language attitudes and ideologies regarding spoken languages, research that investigates sign language ideol- ogies and names them as such is only just emerging. Actually, earlier work in Deaf Studies and sign language research uncovered the existence and power of language ideologies without explicitly using this term. However, it is only quite recently that scholars have begun to explicitly focus on sign language ideologies, conceptualized as such, as a field of study. To the best of our knowledge, this is the first edited volume to do so. Influenced by our backgrounds in anthropology and applied linguistics, in this volume we bring together research that addresses sign language ideologies in practice. In other words, this book highlights the importance of examining language ideologies as they unfold on the ground, undergirded by the premise that what we think that language can do (ideology) is related to what we do with language (practice).¹ All the chapters address the tangled confluence of sign lan- guage ideologies as they influence, manifest in, and are challenged by commu- nicative practices. Contextual analysis shows that language ideologies are often situation-dependent and indeed often seemingly contradictory, varying across space and moments in time. Therefore, rather than only identifying language ideologies as they appear in metalinguistic discourses, the authors in this book analyse how everyday language practices implicitly or explicitly involve ideas about those practices and the other way around. -

Invisible People Poverty and Empowerment in Indonesia
POVERTY AND EMPOWERMENT IN INDONESIA presented by PNPM Mandiri — Indonesia’s National Program for Community Empowerment INVISIBLE PEOPLE POVERTY AND EMPOWERMENT IN INDONESIA Text by Irfan Kortschak photographs by Poriaman Sitanggang with an introduction by Scott Guggenheim presented by PNPM Mandiri — Indonesia’s National Program for Community Empowerment 06 Bengkala, North Bali WHERE EVERYONE SPEAKS DEAF TALK Bengkala is a small village in North Bali. For more than a century, around 2% of “In a village with a large number of deaf the babies here have been born profoundly deaf. In 2008, out of a total population people, the schoolteacher says: ‘Kata of 2450, there were 46 profoundly deaf people, known in the village as kolok. Kolok is what keeps us together as a People who can hear are known as inget. Almost everyone here, both kolok and single community. In Bengkala, being inget, can speak a sign language known as Kata Kolok, or Deaf Talk. deaf is not something carried by the Kata Kolok is a rich and developed language. Like all developed sign languages, kolok alone. It’s something that belongs it uses visually transmitted sign patterns to convey meaning. These sign patterns to the entire community.” usually involve a combination of hand signals; movements of the hands, arms, or body; and facial expressions. Kata Kolok is not dependent on or derived from Balinese, the spoken language of the village, or any other spoken language. It is only slightly influenced by Indonesian Sign Language. It is a distinct, unique language that has a complex grammar of its own. -
Sample File Creator & Lead Developer Military Advisor Yaeger, Cole Busse, Garth Elliott, Andrew J
Sample file www.diasexmachina.com Sample file Creator & Lead Developer Military Advisor Yaeger, Cole Busse, Garth Elliott, Andrew J. Hayford, Chris Tavares Dias Geoffrey Lamb Michael Dake, Jonathon Dyer, James Rivera, Seth Hartley, David Harrison, James Sizemore, Baradaelin, Lead Writers Playtesters Robert Biskin, Patrick Malone, L Kevin Watson, Vahn Kergonan, John T Coleman, Jeremy Wildie, Mathew Chris Dias, Christopher Stilson, Conan Veitch Devon Apple, Jack Gulick, Brian Jones, David Breitenbach, Jose Luis Porfirio, James Gavin, John Jones, Cassandra de Kanter, Jason de Kanter, Rogers, Kean P Stuart, Antonio Martorell Ferriol, Bill Fate Edition Developer Megan Halko, Tyler Halko, Robert Hanz, Tyler "Gryffn88" Stilson, Peter Gates, Kristopher Stein, Christopher Peregrin Stilson Powell, Christopher Ruthenbeck, Sarah Stilson Selenio, Oliver von Spreckelsen, Max Kaehn, Richard J Legg Jr, Peter Dean, Philip Walpole, Sebastian Dietz, Cover Design & Layout Kickstarter Backers Mark A. Siefert, Francois "Stereofm" M., Teppo Pen- nanen, Conan James, Josh Louie, Hamish Thomson, Joshua Raynack Bob Whitely, Courtney Raines, Elisabeth Espiritu, Brian Mead, Derek "Pineapple Steak" Swoyer, Stephen Michael "gleepism" McCormack, Jordan Lazzari, Sar- Abel, Daryl Pruett, Sterling Brucks, Chris Snyder, calistic, Jason LaDue, Matt Dowd, James VanderZan- Cover Illustration Clayton Guerry, Melody Haren Anderson, Louis- den, Ryder DeBruyn, Cassandra de Kanter, Ken Pawlik, Nick Greenwood Philippe Desroches, Tad Rudnicki, Lee McAndrew, Noah Hall, Charles Simpson, Andrew Krause, Evan Chase Davis, David Rosenberg, Lucas Maruk, Toast "Theta" Proctor Jacob P, Steven K. Watkins, Matthew Peters, Robert H. Mitchell Jr., Nathan Beal, Graham Cartography Stanton, Jhereth Jax, Caoimhe Ora Snow, Timothy Lewry, Maura Cowie, Nicholas Stroffolino, Kris Knives, Jeremy Simmons Baker, Steven Kimberley, Shawn Surber, Spazninmov, Peter Engebos, Koen Casier, Trevor Reid, Kary "Realm Peter Perkins, Tavern Keeper, Robert Rittenhouse, C.