Spinalis Origin • SP of the Upper Lumbar and Lower Thoracic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Structure and Function of Breathing
CHAPTERCONTENTS The structure-function continuum 1 Multiple Influences: biomechanical, biochemical and psychological 1 The structure and Homeostasis and heterostasis 2 OBJECTIVE AND METHODS 4 function of breathing NORMAL BREATHING 5 Respiratory benefits 5 Leon Chaitow The upper airway 5 Dinah Bradley Thenose 5 The oropharynx 13 The larynx 13 Pathological states affecting the airways 13 Normal posture and other structural THE STRUCTURE-FUNCTION considerations 14 Further structural considerations 15 CONTINUUM Kapandji's model 16 Nowhere in the body is the axiom of structure Structural features of breathing 16 governing function more apparent than in its Lung volumes and capacities 19 relation to respiration. This is also a region in Fascla and resplrstory function 20 which prolonged modifications of function - Thoracic spine and ribs 21 Discs 22 such as the inappropriate breathing pattern dis- Structural features of the ribs 22 played during hyperventilation - inevitably intercostal musculature 23 induce structural changes, for example involving Structural features of the sternum 23 Posterior thorax 23 accessory breathing muscles as well as the tho- Palpation landmarks 23 racic articulations. Ultimately, the self-perpetuat- NEURAL REGULATION OF BREATHING 24 ing cycle of functional change creating structural Chemical control of breathing 25 modification leading to reinforced dysfunctional Voluntary control of breathing 25 tendencies can become complete, from The autonomic nervous system 26 whichever direction dysfunction arrives, for Sympathetic division 27 Parasympathetic division 27 example: structural adaptations can prevent NANC system 28 normal breathing function, and abnormal breath- THE MUSCLES OF RESPIRATION 30 ing function ensures continued structural adap- Additional soft tissue influences and tational stresses leading to decompensation. -

Vertebral Column and Thorax
Introduction to Human Osteology Chapter 4: Vertebral Column and Thorax Roberta Hall Kenneth Beals Holm Neumann Georg Neumann Gwyn Madden Revised in 1978, 1984, and 2008 The Vertebral Column and Thorax Sternum Manubrium – bone that is trapezoidal in shape, makes up the superior aspect of the sternum. Jugular notch – concave notches on either side of the superior aspect of the manubrium, for articulation with the clavicles. Corpus or body – flat, rectangular bone making up the major portion of the sternum. The lateral aspects contain the notches for the true ribs, called the costal notches. Xiphoid process – variably shaped bone found at the inferior aspect of the corpus. Process may fuse late in life to the corpus. Clavicle Sternal end – rounded end, articulates with manubrium. Acromial end – flat end, articulates with scapula. Conoid tuberosity – muscle attachment located on the inferior aspect of the shaft, pointing posteriorly. Ribs Scapulae Head Ventral surface Neck Dorsal surface Tubercle Spine Shaft Coracoid process Costal groove Acromion Glenoid fossa Axillary margin Medial angle Vertebral margin Manubrium. Left anterior aspect, right posterior aspect. Sternum and Xyphoid Process. Left anterior aspect, right posterior aspect. Clavicle. Left side. Top superior and bottom inferior. First Rib. Left superior and right inferior. Second Rib. Left inferior and right superior. Typical Rib. Left inferior and right superior. Eleventh Rib. Left posterior view and left superior view. Twelfth Rib. Top shows anterior view and bottom shows posterior view. Scapula. Left side. Top anterior and bottom posterior. Scapula. Top lateral and bottom superior. Clavicle Sternum Scapula Ribs Vertebrae Body - Development of the vertebrae can be used in aging of individuals. -

Thoracic and Lumbar Spine Anatomy
ThoracicThoracic andand LumbarLumbar SpineSpine AnatomyAnatomy www.fisiokinesiterapia.biz ThoracicThoracic VertebraeVertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature – Costal Fovea T1 T2-T8 T9-12 ThoracicThoracic VertebraeVertebrae andand RibRib JunctionJunction FunctionsFunctions ofof ThoracicThoracic SpineSpine – Costovertebral Joint – Costotransverse Joint MotionsMotions – All available – Flexion and extension limited – T7-T12 LumbarLumbar SpineSpine BodiesBodies PediclesPedicles LaminaeLaminae TransverseTransverse ProcessProcess SpinousSpinous ProcessProcess ArticularArticular FacetsFacets LumbarLumbar SpineSpine ThoracolumbarThoracolumbar FasciaFascia LumbarLumbar SpineSpine IliolumbarIliolumbar LigamentsLigaments FunctionsFunctions ofof LumbarLumbar SpineSpine – Resistance of anterior translation – Resisting Rotation – Weight Support – Motion IntervertebralIntervertebral DisksDisks RatioRatio betweenbetween diskdisk thicknessthickness andand vertebralvertebral bodybody heightheight DiskDisk CompositionComposition – Nucleus pulposis – Annulus Fibrosis SpinalSpinal LigamentsLigaments AnteriorAnterior LongitudinalLongitudinal PosteriorPosterior LongitudinalLongitudinal LigamentumLigamentum FlavumFlavum InterspinousInterspinous LigamentsLigaments SupraspinousSupraspinous LigamentsLigaments IntertransverseIntertransverse LigamentsLigaments SpinalSpinal CurvesCurves PosteriorPosterior ViewView SagittalSagittal ViewView – Primary – Secondary -

Indications and Treatment of Myofascial Pain
2/25/2017 Indications and Treatment of Myofascial Pain Lisa DeStefano, DO Associate Professor and Chair Department of Osteopathic Manipulative Medicine College of Osteopathic Medicine Michigan State University Common Myofascial Pain Syndromes 1 2/25/2017 2 2/25/2017 Greater Occipital Nerve Impingement Sites . 1: Origin of the third occipital nerve and proximal connection with the greater occipital nerve. 2: Greater occipital nerve as it courses inferior to the inferior oblique muscle. 3: Greater occipital nerve coursing through the semispinalis capitis muscle. 4: Greater occipital nerve exiting the aponeurosis of the trapezius muscle. 5: Greater occipital nerve traveling with the occipital artery. 6: Origin of the greater occipital nerve and relationship to the descending branch of the occipital artery. 7: Suboccipital nerve relation to the vertebral artery and the descending branch of the occipital artery and this nerves interconnection to the greater occipital nerve. 8: Relationship between the third occipital nerve and the C2‐C3 joint complex. Common Treatment Approaches • MFR • MET • Soft Tissue Release • Counterstain • HVLA Etiology of Head and Neck Myofascial Pain Syndromes • Overuse • Posture –Head over the pelvis • Posture – Scapular function • Occlusion –how the teeth control for the proper placement of the mandibular condyle. 3 2/25/2017 Stabilization of the torsobegins with spinotransverse muscle transmission of force onto the epaxial fascia or vertebral aponeurosis. 4 2/25/2017 This then transmits tension into the serratus posterior superior and inferior, which then lifts the upper four ribs and sternum and lowers the lower ribs respectively. In response a force‐ couple is generated between the serratus posterior inferior fascia, external oblique fascia, and the rectus sheath. -

Skeletal System? Skeletal System Chapters 6 & 7 Skeletal System = Bones, Joints, Cartilages, Ligaments
Warm-Up Activity • Fill in the names of the bones in the skeleton diagram. Warm-Up 1. What are the 4 types of bones? Give an example of each. 2. Give 3 ways you can tell a female skeleton from a male skeleton. 3. What hormones are involved in the skeletal system? Skeletal System Chapters 6 & 7 Skeletal System = bones, joints, cartilages, ligaments • Axial skeleton: long axis (skull, vertebral column, rib cage) • Appendicular skeleton: limbs and girdles Appendicular Axial Skeleton Skeleton • Cranium (skull) • Clavicle (collarbone) • Mandible (jaw) • Scapula (shoulder blade) • Vertebral column (spine) • Coxal (pelvic girdle) ▫ Cervical vertebrae • Humerus (arm) ▫ Thoracic vertebrae • Radius, ulna (forearm) ▫ Lumbar vertebrae • Carpals (wrist) • Metacarpals (hand) ▫ Sacrum • Phalanges (fingers, toes) ▫ Coccyx • Femur (thigh) • Sternum (breastbone) • Tibia, fibula (leg) • Ribs • Tarsal, metatarsals (foot) • Calcaneus (heel) • Patella (knee) Functions of the Bones • Support body and cradle soft organs • Protect vital organs • Movement: muscles move bones • Storage of minerals (calcium, phosphorus) & growth factors • Blood cell formation in bone marrow • Triglyceride (fat) storage Classification of Bones 1. Long bones ▫ Longer than they are wide (eg. femur, metacarpels) 2. Short bones ▫ Cube-shaped bones (eg. wrist and ankle) ▫ Sesamoid bones (within tendons – eg. patella) 3. Flat bones ▫ Thin, flat, slightly curved (eg. sternum, skull) 4. Irregular bones ▫ Complicated shapes (eg. vertebrae, hips) Figure 6.2 • Adult = 206 bones • Types of bone -

Glossary of Basic Orthotic & Prosthetic Terminology
Glossary Abduction Moving away from midline. Abductor Muscle involved in active abduction. Acetabulum Socket in pelvis, which receives head of femur. Achilles Tendon Prominent cord at posterior aspect of ankle. Adduction Move toward midline. The position of the components of a prosthesis or orthosis in space Alignment relative to each other and to the patient. Reference position of the body permitting description of location and movements. The individual is standing erect. Head facing forward. Arms Anatomic Position Parallel to the trunk, straight at the sides. Forearms and hands positioned so the palms face forward. Legs straight. Feet parallel to each other. Anterior Toward the front. Not symmetrical; denoting a lack of symmetry between two or more like Asymmetrical parts. The degeneration, or shrinking of a muscle due to lack of use, such as Atrophy in an amputation. Axis Imaginary line passing through center of joint; pivot point. Assembly and alignment of the components of a prosthesis or orthosis Bench alignment using only previously acquired data regarding the patient. Two sides; used to describe an amputee missing both left and right Bilateral extremities. A shell composed of two separate parts that open and shut; used to Bi-valve describe many braces that have two halves; clamshell. Light bulb shaped; circumference small on one end growing larger at Bulbous the bulbous end. CG Center of Gravity. Calcaneus Heel bone Calcification Building up of calcium deposits; bone. Callus Thickening of skin. Carpal The wrist bones and their associated soft parts. Process of modifying the positive model obtained by filling an Cast modification impression in order to obtain a shape which specifies the whole, or part, of the form of the final prosthesis or orthosis. -

Vertebral Column
Vertebral Column • Backbone consists of Cervical 26 vertebrae. • Five vertebral regions – Cervical vertebrae (7) Thoracic in the neck. – Thoracic vertebrae (12) in the thorax. – Lumbar vertebrae (5) in the lower back. Lumbar – Sacrum (5, fused). – Coccyx (4, fused). Sacrum Coccyx Scoliosis Lordosis Kyphosis Atlas (C1) Posterior tubercle Vertebral foramen Tubercle for transverse ligament Superior articular facet Transverse Transverse process foramen Facet for dens Anterior tubercle • Atlas- ring of bone, superior facets for occipital condyles. – Nodding movement signifies “yes”. Axis (C2) Spinous process Lamina Vertebral foramen Transverse foramen Transverse process Superior articular facet Odontoid process (dens) •Axis- dens or odontoid process is body of atlas. – Pivotal movement signifies “no”. Typical Cervical Vertebra (C3-C7) • Smaller bodies • Larger spinal canal • Transverse processes –Shorter – Transverse foramen for vertebral artery • Spinous processes of C2 to C6 often bifid • 1st and 2nd cervical vertebrae are unique – Atlas & axis Typical Cervical Vertebra Spinous process (bifid) Lamina Vertebral foramen Inferior articular process Superior articular process Transverse foramen Pedicle Transverse process Body Thoracic Vertebrae (T1-T12) • Larger and stronger bodies • Longer transverse & spinous processes • Demifacets on body for head of rib • Facets on transverse processes (T1-T10) for tubercle of rib Thoracic Vertebra- superior view Spinous process Transverse process Facet for tubercle of rib Lamina Superior articular process -

Effect of Latissimus Dorsi Muscle Strengthening in Mechanical Low Back Pain
International Journal of Science and Research (IJSR) ISSN: 2319-7064 ResearchGate Impact Factor (2018): 0.28 | SJIF (2019): 7.583 Effect of Latissimus Dorsi Muscle Strengthening in Mechanical Low Back Pain 1 2 Vishakha Vishwakarma , Dr. P. R. Suresh 1, 2PCPS & RC, People’s University, Bhopal (M.P.), India Abstract: Mechanical low back pain (MLBP) is one of the most common musculoskeletal pain syndromes, affecting up to 80% of people at some point during their lifetime. Sources of back pain are numerous, usually sought in as lesion of disc or facet joints at L4- L5 and L5-S1 levels. Studies have shown that 40% of all back pain is of thoracolumbar origin. The term meachnical low back pain also gives reassurance that there is no damage to the nerves or spinal pathology. The clinical presentation of mechanical low back pain usually the ages 18-55 years is in the lumbo sacral region. A study was conducted to evaluate the designed to check the effectiveness of Conventional Exercises alone in Mechanical low back pain and along with the latissimus dorsi muscle strengthening, data was collected from People’s hospital, Bhopal (age group-30-45 yr both male and female randomly) Keywords: Visual analog scale, Assessment chart, Treatment table, Data collection sheets, Essential stationery materials, Computer, SPSS Software etc. 1. Introduction Back pain is a primary to seek medical advice considering 80% of people suffering from back pain. Mechanical low back pain is defined as a result of minor intervertebral dysfunction and referred pain in the low back The latissimus dorsi is a large, flat muscle on the back that and hip region, and can often be confused with the other stretches to the sides, behind the arm, and is partly covered pathologies that may cause these symptoms.18 by the trapezius on the back near the midline, the word latissimus dorsi comes from Latin and its means, broadest muscle of the back dorsum means back. -
Muscles of Mastication Muscles That Move the Head
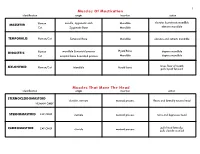
1 Muscles Of Mastication identification origin insertion action maxilla, zygomatic arch Mandible elevates & protracts mandible MASSETER Human Cat Zygomatic Bone Mandible elevates mandible TEMPORALIS Human/Cat Temporal Bone Mandible elevates and retracts mandible Hyoid Bone DIGASTRIC Human mandible & mastoid process depress mandible Cat occipital bone & mastoid process Mandible depress mandible raises floor of mouth; MYLOHYOID Human/Cat Mandible Hyoid bone pulls hyoid forward Muscles That Move The Head identification origin insertion action STERNOCLEIDOMAStoID clavicle, sternum mastoid process flexes and laterally rotates head HUMAN ONLY STERNOMAStoID CAT ONLY sternum mastoid process turns and depresses head pulls head laterally; CLEIDOMAStoID CAT ONLY clavicle mastoid process pulls clavicle craniad 2 Muscles Of The Hyoid, Larynx And Tongue identification origin insertion action Human Sternum Hyoid depresses hyoid bone STERNOHYOID Cat costal cartilage 1st rib Hyoid pulls hyoid caudally; raises ribs and sternum sternum Throid cartilage of larynx Human depresses thyroid cartilage STERNothYROID Cat costal cartilage 1st rib Throid cartilage of larynx pulls larynx caudad elevates thyroid cartilage and Human thyroid cartilage of larynx Hyoid THYROHYOID depresses hyoid bone Cat thyroid cartilage of larynx Hyoid raises larynx GENIOHYOID Human/Cat Mandible Hyoid pulls hyoid craniad 3 Muscles That Attach Pectoral Appendages To Vertebral Column identification origin insertion action Human Occipital bone; Thoracic and Cervical raises clavicle; adducts, -

The Erector Spinae Group Is a Group of 3 Sets of Muscles—Spinalis, Longissimus, and Iliocostalis
The Erector Spinae Group is a group of 3 sets of muscles—spinalis, longissimus, and iliocostalis. The spinalis group are located off of the spinous processes of the vertebrae. The longissimus group are located off of the transverse processes of the vertebrae and the iliocostalis group are located off of the ribs. By knowing these regions we can see that the spinalis group is the most medial and the iliocostalis group is most lateral. 1 During full flexion the erector spinae are relaxed. When standing upright the muscles are active and extension is initiated by the hamstrings—so when you lift a load from the bent over position it causes injury to the erector spinae group. Always lift with a straight back, not when you are hunched over. 2 3 The interspinalis muscles are very tiny muscles that connect from one spinous process to another. The intertransversarii muscles connect between each transverse process. The multifidus lies deep to the erector spinae muscles and it connects from one transverse process to the next spinous process. 4 The rotatores differs from the multifidus by going from 1 transverse process to 2 spinous processes. 5 The external obliques are the most superficial of the oblique muscles. Notice the fibers angle downward and medially, which allows for lateral flexion to same side and rotation to the opposite side. What other muscle does that (neck muscle)?? Once again it takes both sides to contract to cause trunk flexion to occur and only 1 side to cause the rotation and lateral flexion. Now the internal obliques have the fibers directed more horizontally which allows for rotation to the same side when 1 side contracts unlike the external obliques. -

Cervical Vertebrae 1 Cervical Vertebrae
Cervical vertebrae 1 Cervical vertebrae Cervical vertebrae or Cervilar Position of human cervical vertebrae (shown in red). It consists of 7 bones, from top to bottom, C1, C2, C3, C4, C5, C6 and C7. A human cervical vertebra Latin Vertebrae cervicales [1] Gray's p.97 [2] MeSH Cervical+vertebrae [3] TA A02.2.02.001 [4] FMA FMA:72063 In vertebrates, cervical vertebrae (singular: vertebra) are those vertebrae immediately inferior to the skull. Thoracic vertebrae in all mammalian species are defined as those vertebrae that also carry a pair of ribs, and lie caudal to the cervical vertebrae. Further caudally follow the lumbar vertebrae, which also belong to the trunk, but do not carry ribs. In reptiles, all trunk vertebrae carry ribs and are called dorsal vertebrae. In many species, though not in mammals, the cervical vertebrae bear ribs. In many other groups, such as lizards and saurischian dinosaurs, the cervical ribs are large; in birds, they are small and completely fused to the vertebrae. The transverse processes of mammals are homologous to the cervical ribs of other amniotes. Cervical vertebrae 2 In humans, cervical vertebrae are the smallest of the true vertebrae, and can be readily distinguished from those of the thoracic or lumbar regions by the presence of a foramen (hole) in each transverse process, through which passes the vertebral artery. The remainder of this article focuses upon human anatomy. Structure By convention, the cervical vertebrae are numbered, with the first one (C1) located closest to the skull and higher numbered vertebrae (C2-C7) proceeding away from the skull and down the spine. -

Lumbar Muscle Function and Dysfunction in Low Back Pain - Markku Kankaanpää
PHYSIOLOGY AND MAINTENANCE – Vol. IV - Lumbar Muscle Function and Dysfunction in Low Back Pain - Markku Kankaanpää LUMBAR MUSCLE FUNCTION AND DYSFUNCTION IN LOW BACK PAIN Markku Kankaanpää Department of Physical Medicine and Rehabilitation, Kuopio University Hospital, and Department of Physiology, University of Kuopio, Finland Keywords: Low back pain, trunk muscles, muscle coordination, dysfunction, biomechanics, deconditioning syndrome. Contents 1. Anatomy and Function of the Trunk Extensor and Flexor Muscles 1.1. Functional Properties of Lumbar Spine 1.2. Anatomy of Lumbar and Abdominal Muscles 1.3. Control Properties of Lumbar and Abdominal Muscles 2. Epidemiological Aspects of LBP 2.1. Physical Risk Factors of LBP 3. Structural and Pathophysiological Aspects in LBP 4. Lumbar Muscle Dysfunction in LBP 4.1. Loss of Strength 4.2. Excessive Lumbar Muscle Fatigue 4.3. Loss of Co-ordination and Muscle Control 4.4. Active Rehabilitation and Back Extensor Muscle Functional Assessment Glossary Bibliography Biographical Sketch Summary Low back pain is one of the most common health problems. The reason for back pain is most often unknown. Some of the models that help in explaining the origin of low back pain are introduced. The lumbar structure and muscle functions and dysfunctions in relation to low back pain are reviewed. Complex central and peripheral elements control the biomechanics of the lumbar spine and ensure optimal spinal loading in normal everyday life situations.UNESCO Low back pain leads to acute – and EOLSS chronic changes in paraspinal muscles and their control mechanisms. Acute changes are observed as impaired reflexive functions of paraspinal muscles. Pain in spinal structures results from reflexive activities that protect the spine from excessiveSAMPLE and harmful loading.