An Investigation of the Morphology of the Petrotympanic Fissure Using Cone-Beam Computed Tomography
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -
1A. Internal Auditory Meatus
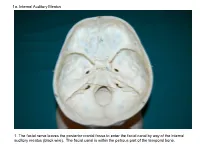
1a. Internal Auditory Meatus 1. The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). The facial canal is within the petrous part of the temporal bone. 1b. Internal Auditory Meatus The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). 2. Hiatus of the Canal and Groove for the Greater Superficial Petrosal Nerve The greater superficial petrosal nerve leaves the facial canal to enter the middle cranial fossa by way of the hiatus of the canal for the greater superficial petrosal nerve (black wire). 3. Pterygoid Canal at Anterior Lip of the Lacerate Foramen The greater superficial petrosal nerve is joined by the deep petrosal nerve to form the nerve of the pterygoid canal (black and red wire). This nerve leaves the middle cranial fossa to enter the pterygopalatine fossa by way of the pterygoid canal. The posterior opening of the pterygoid canal is at the anterior lip of the lacerate foramen. The greater superficial nerve and the deep petrosal nerve travel within the cavernous sinus. 4. Pterygopalatine Fossa Seen Through the Pterygomaxillary Fissure The anterior opening of the pterygoid canal is into the pterygopalatine fossa (black wire). The pterygopalatine fossa is located medial to the pterygomaxillary fissure and contains the pterygopalatine ganglion. 5. External Auditory Meatus The chorda tympani nerve leaves the facial canal and crosses the middle ear (black wire). It then leaves the middle ear to arrive in the infratemporal fossa by way of the petrotympanic fissure. -

Lab Manual Axial Skeleton Atla
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the axial skeleton, which consists of the bones that form the axis of the body. The axial skeleton includes bones in the skull, vertebrae, and thoracic cage, as well as the auditory ossicles and hyoid bone. In addition to learning about all the bones of the axial skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the axial skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. You may also find it helpful to palpate bones on yourself or make drawings of the bones with the bone markings labeled. -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina -

Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens After Decalcification
Hindawi Publishing Corporation International Journal of Otolaryngology Volume 2012, Article ID 418650, 7 pages doi:10.1155/2012/418650 Research Article Dissection and Exposure of the Whole Course of Deep Nerves in Human Head Specimens after Decalcification Longping Liu, Robin Arnold, and Marcus Robinson Discipline of Anatomy and Histology, University of Sydney, Anderson Stuart Building F13, Sydney, NSW 2006, Australia Correspondence should be addressed to Marcus Robinson, [email protected] Received 29 July 2011; Revised 10 November 2011; Accepted 12 December 2011 AcademicEditor:R.L.Doty Copyright © 2012 Longping Liu et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The whole course of the chorda tympani nerve, nerve of pterygoid canal, and facial nerves and their relationships with surrounding structures are complex. After reviewing the literature, it was found that details of the whole course of these deep nerves are rarely reported and specimens displaying these nerves are rarely seen in the dissecting room, anatomical museum, or atlases. Dissections were performed on 16 decalcified human head specimens, exposing the chorda tympani and the nerve connection between the geniculate and pterygopalatine ganglia. Measurements of nerve lengths, branching distances, and ganglia size were taken. The chorda tympani is a very fine nerve (0.44 mm in diameter within the tympanic cavity) and approximately 54 mm in length. The mean length of the facial nerve from opening of internal acoustic meatus to stylomastoid foramen was 52.5 mm. -
Traumatic Dislocation of the Mandibular Condyle Into the Middle Cranial Fossa Treated with Immediate Reconstruction: a Case Report Joseph E
CILLO, SINN, AND ELLIS 859 grafting in a patient with AIDS, acute myocardial infarction, fection and acquired immunodeficiency syndrome. Am J Surg and severe left main coronary artery disease. J Cardiovasc Surg 180:228, 2000 44:55, 2003 18. James J, Hofland HW, Borgstein ES, et al: The prevalence of HIV 15. van Marle J, Tudhope L, Weir G, et al: Vascular disease in infection among burn patients in a burns unit in Malawi and its HIV/AIDS patients. S Afr Med J 92:974, 2002 influence on outcome. Burns 29:55, 2003 16. Chambers AJ, Lord RS: Incidence of acquired immune defi- 19. Patton LL, Shugars DA, Bonito AJ: A systematic review of ciency syndrome (AIDS)-related disorders at laparatomy in pa- complication risks for HIV-positive patients undergoing inva- tients with AIDS. Br J Surg 88:294, 2001 sive dental procedures. J Am Dent Assoc 133:195, 2002 17. Tran HS, Moncure M, Tarnoff M, et al: Predictors of operative 20. Diz Dios P, Fernandez Feijoo J, Vazquez Garcia E: Tooth ex- outcome in patients with human immunodeficiency virus in- traction in HIV sero-positive patients. Int Dent J 49:317, 1999 J Oral Maxillofac Surg 63:859-865, 2005 Traumatic Dislocation of the Mandibular Condyle into the Middle Cranial Fossa Treated With Immediate Reconstruction: A Case Report Joseph E. Cillo, Jr, DMD,* Douglas P. Sinn, DDS,† and Edward Ellis III, DDS, MS‡ While fractures of the mandible condylar process are his chief complaints were right-sided jaw pain, limited common, accounting for 29% to 40% of mandibular mouth opening, and malocclusion with an anterior open trauma,1 dislocation of the mandibular condyle through bite. -

Os Temporale (Halántékcsont)
CRANIOFACIAL AND MAXILLOFACIAL ASPECTS OF THE SKULL PhD., Dr. Dávid Lendvai / Dr. Gábor Baksa Semmelweis University Anatomy, Histology and Embryogy Institute Budapest 2018 MAIN PARTS OF THE SKULL •Constitute by 22 bones: •neurocranium (8) – UNPAIRED: frontal, occipital, sphenoid, ethmoid bones PAIRED: temporal, parietal bones •viscerocranium (14) -UNPAIRED: mandibule, vomer. PAIRED: nasal, maxilla, zygomatic, lacrimal, palatine, inferior nasal concha Their role – formation of cavities, protect viscera, voice formation, initial portions of the gastrointerstinal and respiratory systems, insertion of muscles (mascication, head movements) Cavities: - Cranial cavity, - Nasal cavity, - Paranasal sinuses - Oral cavity, - Orbit, - (Tympanic cavity, Inner ear) Cranium cerebrale 1. calvaria 2. Skull base: •Basis cranii int. •Basis cranii ext. Protub. occip. ext. → linea nuchae sup. → beginning of the linea temp. → zygomatic arch → infratemp. crest → ala major → zygomatic process → supraorbital margin → nasofrontalis suture External skull base Braus Internal skull base Braus Why do we need the neuroanatomy? Picture: Peter Claesz – Vanitas (still-life, 1630.) www.hydrocephalus.inf o ? www.totalhealth.co.u k Aesculap - B Braun Todoro w Physiologically volume and pressure are balanced within the skull A minimally disturbed balance can be already compensated Over the normal range of this compensation ability minimal changes in the volume lead to a disproportionally high elevation of intracranial pressure (ICP) (for further see in physiology the Monroe -

Inferior View of Skull
human anatomy 2016 lecture sixth Dr meethak ali ahmed neurosurgeon Inferior View Of Skull the anterior part of this aspect of skull is seen to be formed by the hard palate.The palatal process of the maxilla and horizontal plate of the palatine bones can be identified . in the midline anteriorly is the incisive fossa & foramen . posterolaterlly are greater & lesser palatine foramena. Above the posterior edge of the hard palate are the choanae(posterior nasal apertures ) . these are separated from each other by the posterior margin of the vomer & bounded laterally by the medial pterygoid plate of sphenoid bone . the inferior end of the medial pterygoid plate is prolonged as a curved spike of bone , the pterygoid hamulus. the superior end widens to form the scaphoid fossa . posterolateral to the lateral pterygoid plate the greater wing of the sphenoid is pieced by the large foramen ovale & small foramen spinosum . posterolateral to the foramen spinosum is spine of the sphenoid . Above the medial border of the scaphoid fossa , the sphenoid bone is pierced by pterygoid canal . Behind the spine of the sphenoid , in the interval between the greater wing of the sphenoid and the petrous part of the temporal bone , there is agroove for the cartilaginous part of the auditory tube. The opening of the bony part of the tube can be identified. The mandibular fossa of the temporal bone & the articular tubercle form the upper articular surfaces for the temporomandibular joint . separating the mandibular fossa from the tympanic plate posteriorly is the squamotympanic fissure, through the medial end of which (petrotympanic fissure ) the chorda tympani exits from the tympanic cavity .The styloid process of the temporal bone projects downward & forward from its inferior aspect. -

Skull / Cranium
Important! 1. Memorizing these pages only does not guarantee the succesfull passing of the midterm test or the semifinal exam. 2. The handout has not been supervised, and I can not guarantee, that these pages are absolutely free from mistakes. If you find any, please, report to me! SKULL / CRANIUM BONES OF THE NEUROCRANIUM (7) Occipital bone (1) Sphenoid bone (1) Temporal bone (2) Frontal bone (1) Parietal bone (2) BONES OF THE VISCEROCRANIUM (15) Ethmoid bone (1) Maxilla (2) Mandible (1) Zygomatic bone (2) Nasal bone (2) Lacrimal bone (2) Inferior nasalis concha (2) Vomer (1) Palatine bone (2) Compiled by: Dr. Czigner Andrea 1 FRONTAL BONE MAIN PARTS: FRONTAL SQUAMA ORBITAL PARTS NASAL PART FRONTAL SQUAMA Parietal margin Sphenoid margin Supraorbital margin External surface Frontal tubercle Temporal surface Superciliary arch Zygomatic process Glabella Supraorbital margin Frontal notch Supraorbital foramen Internal surface Frontal crest Sulcus for superior sagittal sinus Foramen caecum ORBITAL PARTS Ethmoidal notch Cerebral surface impresiones digitatae Orbital surface Fossa for lacrimal gland Trochlear notch / fovea Anterior ethmoidal foramen Posterior ethmoidal foramen NASAL PART nasal spine nasal margin frontal sinus Compiled by: Dr. Czigner Andrea 2 SPHENOID BONE MAIN PARTS: CORPUS / BODY GREATER WINGS LESSER WINGS PTERYGOID PROCESSES CORPUS / BODY Sphenoid sinus Septum of sphenoid sinus Sphenoidal crest Sphenoidal concha Apertura sinus sphenoidalis / Opening of sphenoid sinus Sella turcica Hypophyseal fossa Dorsum sellae Posterior clinoid process Praechiasmatic sulcus Carotid sulcus GREATER WINGS Cerebral surface • Foramen rotundum • Framen ovale • Foramen spinosum Temporal surface Infratemporalis crest Infratemporal surface Orbital surface Maxillary surface LESSER WINGS Anterior clinoid process Superior orbital fissure Optic canal PTERYGOID PROCESSES Lateral plate Medial plate Pterygoid hamulus Pterygoid fossa Pterygoid sulcus Scaphoid fossa Pterygoid notch Pterygoid canal (Vidian canal) Compiled by: Dr. -

Mandibular Fossa of Homo Erectus
THEANATOMICALRECORD266:142–145(2002) DOI10.1002/ar.10053 BoneBits MandibularFossaofHomoerectus: AResponsetoDurband 1,2 3–6 4–7 KENMOWBRAY, *SAMUELMA´ RQUEZ, ANDERICDELSON 1DivisionofAnthropology,AmericanMuseumofNaturalHistory, NewYork,NewYork 2DepartmentofAnthropology,RutgersUniversity,NewBrunswick,NewJersey 3CenterofAnatomyandFunctionalMorphology,MountSinaiSchoolofMedicine, NewYork,NewYork 4DepartmentofAnthropology,LehmanCollege/CUNY,Bronx,NewYork 5Ph.D.PrograminAnthropology,CUNYGraduateCenter,NewYork,NewYork 6NewYorkConsortiuminEvolutionaryPrimatology,CityUniversityofNewYork, NewYork,NewYork 7DivisionofPaleontology,AmericanMuseumofNaturalHistory, NewYork,NewYork Durband(2002)hascriticizedourrecentanalysisof WT15000alsoshowsaflatandlongfossa,butthe Sambungmacan3(Delsonetal.,2001)withregardtothe squamotympanicfissurecoursesinitsdeepestpor- implicationsofthesquamotympanicfissure(SQF)andthe tion.However,itisnotedagainthatgrowthhasnot postglenoidtubercle(PGT)forgroupingHomoerectusfos- beencompletedinthisspecimen(seeabove).Finally, sils.Hiscriticismisbasedupontwoabstractsandan OH9presentsamandibularfossathatissimilarboth unpublished masters thesis (Durband 1997, 1998; initsshapeandinthepositionofthesquamotym- DurbandandKidder,2000)anddependsoninterpretation panicfissuretotheNgandongandotherIndonesian oftheobservedmorphologyaswellasthetaxonomic specimens.ItappearsthatthistraitunitestheIndo- “weight”ofthesecharacters.Herewetaketheopportunity nesianH.erectusspecimenstotheexclusionofthe tobrieflyrespondtohisqueriesandprovideobservations otherAsianandAfricanones,withtheexceptionof -

The Tympanic Region of the Mammalian Skull by P. N. Van Kampen*
The tympanic region of the mammalian skull by P. N. van Kampen* [p.466] VI. Tubulidentata Wall of the middle ear The tympanic bone of Orycteropus (Fig. 31) contributes neither to the construction of the wall of the middle ear cavity nor to the wall of the external ear tube. The tympanic has the form of a slightly slanted, large, thick, and dorsally incomplete ring. The anterior crus broadens into a plate whose lateral margin ends ventrally with a short process. The point of the posterior crus is very thin and at its end bent into a hook-shape. Except for the Processus Folii, the tympanic bone is not fused with any bone. It also lies entirely free, the ends of the two crurae excepted. The anterior crus immediately behind the glenoid fossa abuts with the squamosal; the posterior crus covers the tympanohyal laterally, but remains separate from the squamosal. The tympanic and the ear drum form the external wall of the middle ear cavity. The inner wall is entirely formed of the promontorium, which ends in a sharp crest. Between the tympanic an petrosal there remains an additional open fissure, which according to Hyrtyl is closed during life only by a membrane. An ossified tympanic tube is thereby not distinct on the skull. The alisphenoid extends between petrosal and tympanic and forms the anterodorsal wall of the middle ear cavity. Arterial course Hyrtyl (1850) describes a stapedial artery, “which reaches the drum-cavity through a hole in the posterior wall in the middle ear bone; it rises onto the promontorium towards the stapes via a fairly deep groove, moving to the upper wall of the ear cavity, and ultimately into the braincase, between the crurae of the stapes.” The groove for this artery lies orally from the fenestra cochleae; the foramen spinosum, through which the artery leaves the middle ear cavity, is probably the small opening, which is evident on the border between the tegmen tympani and squamosal (see fig. -

Spring Quarter Lawrence M. Witmer, Phd Life Sciences Building, Room 123
Skull PCC I: Spring Quarter Lawrence M. Witmer, PhD Life Sciences Building, Room 123 READINGS: Moore & Dalley’s text: 832–850; Moore & Persaud’s Embryology text: 414–419, 216–230 LAB READING: Dissector: 221–223; this handout provides the major source for the lab reading— BRING THIS HANDOUT TO LAB I. General Terms A. Skull: may or may not include mandible (i.e., sources vary) B. Cranium (= neurocranium): that part enclosing the brain 1. Calvaria: superior part 2. Cranial base (= basicranium): inferior part 3. Includes: parietals, temporals, frontal, occipital, sphenoid, ethmoid 4. Calotte: the “skull cap” sawed off for autopsies & dissection C. Facial skeleton 1. The rest of the head skeleton 2. Includes: maxillae, zygomatics, palatines, lacrimals, nasals, inferior nasal conchae, vomer, ethmoid, mandible D. Sutures: junctures between the individual skull bones II. Embryology & Development A. Organization 1. Portions of the skull a. Neurocranium: surrounding the brain b. Viscerocranium: the jaw apparatus and associated structures 2. Types of ossification a. Endochondral ossification: bones are ossified from cartilaginous precursors b. Intramembranous ossification: bones are ossified directly from mesenchyme investing various structures (e.g., the brain, cartilaginous structures) B. Developmental origins of the skull 1. Cartilaginous neurocranium (= chondrocranium) a. Forms from fusion of several primordial cartilages b. Forms structures in skull base via endochondral ossification Witmer – Skull – Spring Quarter – 1 c. Adult bones: occipital, petromastoid part of temporal bone, sphenoid, ethmoid 2. Membranous neurocranium a. Forms bones around the brain via intramembranous ossification b. Adult bones: frontal, parietal 3. Cartilaginous viscerocranium a. Forms from the cartilages of the first two branchial arches via endochondral ossification b.