Chronic Granulomatous Disease: a Review of the Infectious And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Virulence Determinants, Drug Resistance and Mobile Genetic
Lau et al. Cell & Bioscience 2011, 1:17 http://www.cellandbioscience.com/content/1/1/17 Cell & Bioscience RESEARCH Open Access Virulence determinants, drug resistance and mobile genetic elements of Laribacter hongkongensis: a genome-wide analysis Susanna KP Lau1,2,3,4*†, Gilman KM Wong4†, Alan KL Tsang4†, Jade LL Teng4, Rachel YY Fan4, Herman Tse1,2,3,4, Kwok-Yung Yuen1,2,3,4 and Patrick CY Woo1,2,3,4* Abstract Background: Laribacter hongkongensis is associated with community-acquired gastroenteritis and traveler’s diarrhea. In this study, we performed an in-depth annotation of the genes in its genome related to the various steps in the infective process, drug resistance and mobile genetic elements. Results: For acid and bile resistance, L. hongkongensis possessed a urease gene cassette, two arc gene clusters and bile salt efflux systems. For intestinal colonization, it possessed a putative adhesin of the autotransporter family homologous to those of diffusely adherent Escherichia coli (E. coli) and enterotoxigenic E. coli. To evade from host defense, it possessed superoxide dismutase and catalases. For lipopolysaccharide biosynthesis, it possessed the same set of genes that encode enzymes for synthesizing lipid A, two Kdo units and heptose units as E. coli, but different genes for its symmetrical acylation pattern, and nine genes for polysaccharide side chains biosynthesis. It contained a number of CDSs that encode putative cell surface acting (RTX toxin and hemolysins) and intracellular cytotoxins (patatin-like proteins) and enzymes for invasion (outer membrane phospholipase A). It contained a broad variety of antibiotic resistance-related genes, including genes related to b-lactam (n = 10) and multidrug efflux (n = 54). -

The Case for Lupus Nephritis
Journal of Clinical Medicine Review Expanding the Role of Complement Therapies: The Case for Lupus Nephritis Nicholas L. Li * , Daniel J. Birmingham and Brad H. Rovin Department of Internal Medicine, Division of Nephrology, The Ohio State University, Columbus, OH 43210, USA; [email protected] (D.J.B.); [email protected] (B.H.R.) * Correspondence: [email protected]; Tel.: +1-614-293-4997; Fax: +1-614-293-3073 Abstract: The complement system is an innate immune surveillance network that provides defense against microorganisms and clearance of immune complexes and cellular debris and bridges innate and adaptive immunity. In the context of autoimmune disease, activation and dysregulation of complement can lead to uncontrolled inflammation and organ damage, especially to the kidney. Systemic lupus erythematosus (SLE) is characterized by loss of tolerance, autoantibody production, and immune complex deposition in tissues including the kidney, with inflammatory consequences. Effective clearance of immune complexes and cellular waste by early complement components protects against the development of lupus nephritis, while uncontrolled activation of complement, especially the alternative pathway, promotes kidney damage in SLE. Therefore, complement plays a dual role in the pathogenesis of lupus nephritis. Improved understanding of the contribution of the various complement pathways to the development of kidney disease in SLE has created an opportunity to target the complement system with novel therapies to improve outcomes in lupus nephritis. In this review, we explore the interactions between complement and the kidney in SLE and their implications for the treatment of lupus nephritis. Keywords: lupus nephritis; complement; systemic lupus erythematosus; glomerulonephritis Citation: Li, N.L.; Birmingham, D.J.; Rovin, B.H. -

Are Complement Deficiencies Really Rare?
G Model MIMM-4432; No. of Pages 8 ARTICLE IN PRESS Molecular Immunology xxx (2014) xxx–xxx Contents lists available at ScienceDirect Molecular Immunology j ournal homepage: www.elsevier.com/locate/molimm Review Are complement deficiencies really rare? Overview on prevalence, ଝ clinical importance and modern diagnostic approach a,∗ b Anete Sevciovic Grumach , Michael Kirschfink a Faculty of Medicine ABC, Santo Andre, SP, Brazil b Institute of Immunology, University of Heidelberg, Heidelberg, Germany a r a t b i c s t l e i n f o r a c t Article history: Complement deficiencies comprise between 1 and 10% of all primary immunodeficiencies (PIDs) accord- Received 29 May 2014 ing to national and supranational registries. They are still considered rare and even of less clinical Received in revised form 18 June 2014 importance. This not only reflects (as in all PIDs) a great lack of awareness among clinicians and gen- Accepted 23 June 2014 eral practitioners but is also due to the fact that only few centers worldwide provide a comprehensive Available online xxx laboratory complement analysis. To enable early identification, our aim is to present warning signs for complement deficiencies and recommendations for diagnostic approach. The genetic deficiency of any Keywords: early component of the classical pathway (C1q, C1r/s, C2, C4) is often associated with autoimmune dis- Complement deficiencies eases whereas individuals, deficient of properdin or of the terminal pathway components (C5 to C9), are Warning signs Prevalence highly susceptible to meningococcal disease. Deficiency of C1 Inhibitor (hereditary angioedema, HAE) Meningitis results in episodic angioedema, which in a considerable number of patients with identical symptoms Infections also occurs in factor XII mutations. -

Practice Parameter for the Diagnosis and Management of Primary Immunodeficiency
Practice parameter Practice parameter for the diagnosis and management of primary immunodeficiency Francisco A. Bonilla, MD, PhD, David A. Khan, MD, Zuhair K. Ballas, MD, Javier Chinen, MD, PhD, Michael M. Frank, MD, Joyce T. Hsu, MD, Michael Keller, MD, Lisa J. Kobrynski, MD, Hirsh D. Komarow, MD, Bruce Mazer, MD, Robert P. Nelson, Jr, MD, Jordan S. Orange, MD, PhD, John M. Routes, MD, William T. Shearer, MD, PhD, Ricardo U. Sorensen, MD, James W. Verbsky, MD, PhD, David I. Bernstein, MD, Joann Blessing-Moore, MD, David Lang, MD, Richard A. Nicklas, MD, John Oppenheimer, MD, Jay M. Portnoy, MD, Christopher R. Randolph, MD, Diane Schuller, MD, Sheldon L. Spector, MD, Stephen Tilles, MD, Dana Wallace, MD Chief Editor: Francisco A. Bonilla, MD, PhD Co-Editor: David A. Khan, MD Members of the Joint Task Force on Practice Parameters: David I. Bernstein, MD, Joann Blessing-Moore, MD, David Khan, MD, David Lang, MD, Richard A. Nicklas, MD, John Oppenheimer, MD, Jay M. Portnoy, MD, Christopher R. Randolph, MD, Diane Schuller, MD, Sheldon L. Spector, MD, Stephen Tilles, MD, Dana Wallace, MD Primary Immunodeficiency Workgroup: Chairman: Francisco A. Bonilla, MD, PhD Members: Zuhair K. Ballas, MD, Javier Chinen, MD, PhD, Michael M. Frank, MD, Joyce T. Hsu, MD, Michael Keller, MD, Lisa J. Kobrynski, MD, Hirsh D. Komarow, MD, Bruce Mazer, MD, Robert P. Nelson, Jr, MD, Jordan S. Orange, MD, PhD, John M. Routes, MD, William T. Shearer, MD, PhD, Ricardo U. Sorensen, MD, James W. Verbsky, MD, PhD GlaxoSmithKline, Merck, and Aerocrine; has received payment for lectures from Genentech/ These parameters were developed by the Joint Task Force on Practice Parameters, representing Novartis, GlaxoSmithKline, and Merck; and has received research support from Genentech/ the American Academy of Allergy, Asthma & Immunology; the American College of Novartis and Merck. -

List of the Pathogens Intended to Be Controlled Under Section 18 B.E
(Unofficial Translation) NOTIFICATION OF THE MINISTRY OF PUBLIC HEALTH RE: LIST OF THE PATHOGENS INTENDED TO BE CONTROLLED UNDER SECTION 18 B.E. 2561 (2018) By virtue of the provision pursuant to Section 5 paragraph one, Section 6 (1) and Section 18 of Pathogens and Animal Toxins Act, B.E. 2558 (2015), the Minister of Public Health, with the advice of the Pathogens and Animal Toxins Committee, has therefore issued this notification as follows: Clause 1 This notification is called “Notification of the Ministry of Public Health Re: list of the pathogens intended to be controlled under Section 18, B.E. 2561 (2018).” Clause 2 This Notification shall come into force as from the following date of its publication in the Government Gazette. Clause 3 The Notification of Ministry of Public Health Re: list of the pathogens intended to be controlled under Section 18, B.E. 2560 (2017) shall be cancelled. Clause 4 Define the pathogens codes and such codes shall have the following sequences: (1) English alphabets that used for indicating the type of pathogens are as follows: B stands for Bacteria F stands for fungus V stands for Virus P stands for Parasites T stands for Biological substances that are not Prion R stands for Prion (2) Pathogen risk group (3) Number indicating the sequence of each type of pathogens Clause 5 Pathogens intended to be controlled under Section 18, shall proceed as follows: (1) In the case of being the pathogens that are utilized and subjected to other law, such law shall be complied. (2) Apart from (1), the law on pathogens and animal toxin shall be complied. -

Genetic and Functional Studies of the Mip Protein of Legionella
t1.ì. Genetic and Functional Studies of the Mip Protein of Legionella Rodney Mark Ratcliff, BSc (Hons)' MASM Infectious Diseases Laboratories Institute of Medical and Veterinary Science and Department of Microbiology and Immunology UniversitY of Adelaide. Adelaide, South Australia A thesis submitted to the University of Adelaide for the degree of I)octor of Philosophy 15'h March 2000 amended 14th June 2000 Colonies of several Legionella strains on charcoal yeast extract agar (CYE) after 4 days incubation at 37"C in air. Various magnifications show typical ground-glass opalescent appearance. Some pure strains exhibit pleomorphic growth or colour. The top two photographs demonstrate typical red (LH) and blue-white (RH) fluorescence exhibited by some species when illuminated by a Woods (IJV) Lamp. * t Table of Contents .1 Chapter One: Introduction .1 Background .............'. .2 Morphology and TaxonomY J Legionellosis ............. 5 Mode of transmission "..'....'. 7 Environmental habitat 8 Interactions between Legionella and phagocytic hosts 9 Attachment 11 Engulfment and internalisation.'.. 13 Intracellular processing 13 Intracellular replication of legionellae .. " "' " "' 15 Host cell death and bacterial release 18 Virulence (the Genetic factors involved with intracellular multiplication and host cell killing .20 icm/dot system) Legiolysin .25 Msp (Znn* metaloprotease) ...'..... .25 .28 Lipopolysaccharide .29 The association of flagella with disease.. .30 Type IV fimbriae.... .31 Major outer membrane proteins....'.......'. JJ Heat shock proteins'.'. .34 Macrophage infectivity potentiator (Mip) protein Virulenceiraits of Legionella species other than L. pneumophila..........' .39 phylogeny .41 Chapter One (continued): Introduction to bacterial classification and .41 Identificati on of Legionella...'.,..'.. .46 Phylogeny .52 Methods of phylogenetic analysis' .53 Parsimony methods.'.. .55 Distance methods UPGMA cluster analYsis.'.'... -

WO 2014/176636 A9 6 November 2014 (06.11.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) CORRECTED VERSION (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/176636 A9 6 November 2014 (06.11.2014) P O P C T (51) International Patent C I 1/40 Moira Street, Adamstown, New South Wales 2289 C07C 279/02 (2006.01) C07C 275/68 (2006.01) (AU). C07C 241/04 (2006.01) A61K 31/4045 (2006.01) (74) Agent: WRAYS; 56 Ord Street, West Perth, Western Aus C07C 281/08 (2006.01) A61K 31/155 (2006.01) tralia 6005 (AU). C07C 337/08 (2006.01) A61K 31/4192 (2006.01) C07C 281/18 (2006.01) A61K 31/341 (2006.01) (81) Designated States (unless otherwise indicated, for every C07C 249/14 (2006.01) A61K 31/381 (2006.01) kind of national protection available): AE, AG, AL, AM, C07D 407/12 (2006.01) A61K 31/498 (2006.01) AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, C07D 403/12 (2006.01) A61K 31/44 (2006.01) BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, C07D 409/12 (2006.01) A61K 31/12 (2006.01) DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, C07D 401/12 (2006.01) A61P 31/04 (2006.01) HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, (21) International Application Number: MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, PCT/AU20 14/000483 OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (22) International Filing Date: SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, 1 May 2014 (01 .05.2014) TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. -

European Society for Immunodeficiencies (ESID)
Journal of Clinical Immunology https://doi.org/10.1007/s10875-020-00754-1 ORIGINAL ARTICLE European Society for Immunodeficiencies (ESID) and European Reference Network on Rare Primary Immunodeficiency, Autoinflammatory and Autoimmune Diseases (ERN RITA) Complement Guideline: Deficiencies, Diagnosis, and Management Nicholas Brodszki1 & Ashley Frazer-Abel2 & Anete S. Grumach3 & Michael Kirschfink4 & Jiri Litzman5 & Elena Perez6 & Mikko R. J. Seppänen7 & Kathleen E. Sullivan8 & Stephen Jolles9 Received: 5 June 2019 /Accepted: 20 January 2020 # The Author(s) 2020 Abstract This guideline aims to describe the complement system and the functions of the constituent pathways, with particular focus on primary immunodeficiencies (PIDs) and their diagnosis and management. The complement system is a crucial part of the innate immune system, with multiple membrane-bound and soluble components. There are three distinct enzymatic cascade pathways within the complement system, the classical, alternative and lectin pathways, which converge with the cleavage of central C3. Complement deficiencies account for ~5% of PIDs. The clinical consequences of inherited defects in the complement system are protean and include increased susceptibility to infection, autoimmune diseases (e.g., systemic lupus erythematosus), age-related macular degeneration, renal disorders (e.g., atypical hemolytic uremic syndrome) and angioedema. Modern complement analysis allows an in-depth insight into the functional and molecular basis of nearly all complement deficiencies. However, therapeutic options remain relatively limited for the majority of complement deficiencies with the exception of hereditary angioedema and inhibition of an overactivated complement system in regulation defects. Current management strategies for complement disor- ders associated with infection include education, family testing, vaccinations, antibiotics and emergency planning. Keywords Complement . -

ESID Registry – Working Definitions for Clinical Diagnosis of PID
ESID Registry – Working Definitions for Clinical Diagnosis of PID These criteria are only for patients with no genetic diagnosis*. *Exceptions: Atypical SCID, DiGeorge syndrome – a known genetic defect and confirmation of criteria is mandatory. Available entries (Please click on an entry to see the criteria.) Page Acquired angioedema .................................................................................................................................................................. 4 Agammaglobulinemia .................................................................................................................................................................. 4 Asplenia syndrome (Ivemark syndrome) ................................................................................................................................... 4 Ataxia telangiectasia (ATM) ......................................................................................................................................................... 4 Atypical Severe Combined Immunodeficiency (Atypical SCID) ............................................................................................... 5 Autoimmune lymphoproliferative syndrome (ALPS) ................................................................................................................ 5 APECED / APS1 with CMC - Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy (APECED) .................. 5 Barth syndrome ........................................................................................................................................................................... -

Interactions Between Activated Platelets and the Complement System
REVIEW published: 10 July 2019 doi: 10.3389/fimmu.2019.01590 The Human Platelet as an Innate Immune Cell: Interactions Between Activated Platelets and the Complement System Oskar Eriksson 1, Camilla Mohlin 2, Bo Nilsson 1 and Kristina N. Ekdahl 1,2* 1 Department of Immunology, Genetics and Pathology, Uppsala University, Uppsala, Sweden, 2 Linnaeus Center of Biomaterials Chemistry, Linnaeus University, Kalmar, Sweden Platelets play an essential role in maintaining homeostasis in the circulatory system after an injury by forming a platelet thrombus, but they also occupy a central node in the intravascular innate immune system. This concept is supported by their extensive interactions with immune cells and the cascade systems of the blood. In this review we discuss the close relationship between platelets and the complement system and the role of these interactions during thromboinflammation. Platelets are protected Edited by: from complement-mediated damage by soluble and membrane-expressed complement Benoît Ho-Tin-Noé, regulators, but they bind several complement components on their surfaces and Institut National de la Santé et de la Recherche Médicale trigger complement activation in the fluid phase. Furthermore, localized complement (INSERM), France activation may enhance the procoagulant responses of platelets through the generation Reviewed by: of procoagulant microparticles by insertion of sublytic amounts of C5b9 into the platelet Craig Norman Morrell, University of Rochester, United States membrane. We also highlight the role of post-translational protein modifications in Viviana P. Ferreira, regulating the complement system and the critical role of platelets in driving these University of Toledo, United States reactions. In particular, modification of disulfide bonds by thiol isomerases and protein Kerstin Jurk, Johannes Gutenberg University phosphorylation by extracellular kinases have emerged as important mechanisms to Mainz, Germany fine-tune complement activity in the platelet microenvironment. -
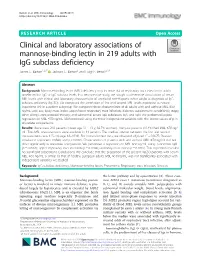
Clinical and Laboratory Associations of Mannose-Binding Lectin in 219 Adults with Igg Subclass Deficiency James C
Barton et al. BMC Immunology (2019) 20:15 https://doi.org/10.1186/s12865-019-0296-x RESEARCHARTICLE Open Access Clinical and laboratory associations of mannose-binding lectin in 219 adults with IgG subclass deficiency James C. Barton1,2,3* , Jackson C. Barton2 and Luigi F. Bertoli2,3,4 Abstract Background: Mannose-binding lectin (MBL) deficiency may increase risk of respiratory tract infection in adults unselected for IgG or IgG subclass levels. In a retrospective study, we sought to determine associations of serum MBL levels with clinical and laboratory characteristics of unrelated non-Hispanic white adults at diagnosis of IgG subclass deficiency (IgGSD). We computed the correlation of first and second MBL levels expressed as natural logarithms (ln) in a patient subgroup. We compared these characteristics of all adults with and without MBL ≤50 ng/mL: age; sex; body mass index; upper/lower respiratory tract infection; diabetes; autoimmune condition(s); atopy; other allergy; corticosteroid therapy; and subnormal serum IgG subclasses, IgA, and IgM. We performed logistic regression on MBL ≤50 ng/mL (dichotomous) using the three independent variables with the lowest values of p in univariate comparisons. Results: There were 219 patients (mean age 51 ± 13 y; 82.5% women). Thirty-six patients (16.4%) had MBL ≤50 ng/ mL. Two MBL measurements were available in 14 patients. The median interval between the first and second measurements was 125 d (range 18–1031). For ln-transformed data, we observed adjusted r2 = 0.9675; Pearson correlation coefficient 0.9849; and p < 0.0001. Characteristics of patients with and without MBL ≤50 ng/mL did not differ significantly in univariate comparisons. -
2. Drinking Water Systems in Buildings
g e n liviC tnm apeD apeD r apeD r r nemt nemt t nemt t o t o f o f C f C i C v i v i v l i l i l gnE gnE i gnE i i een een r een r i r i i gn gn gn .sroodni emit rieht fo tsom dneps snamuH snamuH snamuH dneps dneps dneps tsom tsom tsom fo fo fo rieht rieht rieht emit emit emit .sroodni .sroodni .sroodni - o- t o t l aA l aA smetsys st i ht iw tnemnor ivne t l iub er i tne ehT ehT ehT tne i tne i tne er i er er iub l iub t l iub t l t ivne ivne ivne tnemnor tnemnor tnemnor iw iw ht iw ht ht i i st i st st smetsys smetsys smetsys - o t l aA DD DD DD MMicrobiologicalMicrobiologicalicrobiological effectseffectseffects ofofof yaw a ni detarepo dna dengised eb dluohs dluohs dluohs eb eb eb dengised dengised dengised dna dna dna detarepo detarepo detarepo ni ni ni a a a yaw yaw yaw 681 681 681 / / .efas yl lacigoloiborcim si t i taht taht i taht t i t i t si si si lacigoloiborcim lacigoloiborcim yl lacigoloiborcim yl yl .efas .efas .efas / nen inen knI i knI i nneJ i nneJ nen i knI i nneJ 8102 8102 8102 ccoppercopperopper andandand otherotherother abioticabioticabiotic euqinu eht no sesucof siseht sihT sihT sihT siseht siseht siseht sesucof sesucof sesucof no no no eht eht eht euqinu euqinu euqinu n ea nkidf ecnlcgliocim im im lacigoloiborc lacigoloiborc lacigoloiborc sehcin sehcin sehcin fo fo fo gniknird gniknird gniknird retaw retaw retaw dna dna dna gniz i l i tu stnemnor ivne roodni ecaf rus hcuot hcuot hcuot rus rus rus ecaf ecaf ecaf roodni roodni roodni ivne ivne ivne stnemnor stnemnor stnemnor tu i tu l i tu i l i i l i gniz gniz gniz