Skeletal Endocrinology: Where Evolutionary Advantage Meets Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
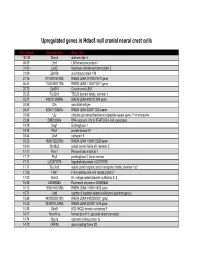
Supp Table 1.Pdf
Upregulated genes in Hdac8 null cranial neural crest cells fold change Gene Symbol Gene Title 134.39 Stmn4 stathmin-like 4 46.05 Lhx1 LIM homeobox protein 1 31.45 Lect2 leukocyte cell-derived chemotaxin 2 31.09 Zfp108 zinc finger protein 108 27.74 0710007G10Rik RIKEN cDNA 0710007G10 gene 26.31 1700019O17Rik RIKEN cDNA 1700019O17 gene 25.72 Cyb561 Cytochrome b-561 25.35 Tsc22d1 TSC22 domain family, member 1 25.27 4921513I08Rik RIKEN cDNA 4921513I08 gene 24.58 Ofa oncofetal antigen 24.47 B230112I24Rik RIKEN cDNA B230112I24 gene 23.86 Uty ubiquitously transcribed tetratricopeptide repeat gene, Y chromosome 22.84 D8Ertd268e DNA segment, Chr 8, ERATO Doi 268, expressed 19.78 Dag1 Dystroglycan 1 19.74 Pkn1 protein kinase N1 18.64 Cts8 cathepsin 8 18.23 1500012D20Rik RIKEN cDNA 1500012D20 gene 18.09 Slc43a2 solute carrier family 43, member 2 17.17 Pcm1 Pericentriolar material 1 17.17 Prg2 proteoglycan 2, bone marrow 17.11 LOC671579 hypothetical protein LOC671579 17.11 Slco1a5 solute carrier organic anion transporter family, member 1a5 17.02 Fbxl7 F-box and leucine-rich repeat protein 7 17.02 Kcns2 K+ voltage-gated channel, subfamily S, 2 16.93 AW493845 Expressed sequence AW493845 16.12 1600014K23Rik RIKEN cDNA 1600014K23 gene 15.71 Cst8 cystatin 8 (cystatin-related epididymal spermatogenic) 15.68 4922502D21Rik RIKEN cDNA 4922502D21 gene 15.32 2810011L19Rik RIKEN cDNA 2810011L19 gene 15.08 Btbd9 BTB (POZ) domain containing 9 14.77 Hoxa11os homeo box A11, opposite strand transcript 14.74 Obp1a odorant binding protein Ia 14.72 ORF28 open reading -

140503 IPF Signatures Supplement Withfigs Thorax
Supplementary material for Heterogeneous gene expression signatures correspond to distinct lung pathologies and biomarkers of disease severity in idiopathic pulmonary fibrosis Daryle J. DePianto1*, Sanjay Chandriani1⌘*, Alexander R. Abbas1, Guiquan Jia1, Elsa N. N’Diaye1, Patrick Caplazi1, Steven E. Kauder1, Sabyasachi Biswas1, Satyajit K. Karnik1#, Connie Ha1, Zora Modrusan1, Michael A. Matthay2, Jasleen Kukreja3, Harold R. Collard2, Jackson G. Egen1, Paul J. Wolters2§, and Joseph R. Arron1§ 1Genentech Research and Early Development, South San Francisco, CA 2Department of Medicine, University of California, San Francisco, CA 3Department of Surgery, University of California, San Francisco, CA ⌘Current address: Novartis Institutes for Biomedical Research, Emeryville, CA. #Current address: Gilead Sciences, Foster City, CA. *DJD and SC contributed equally to this manuscript §PJW and JRA co-directed this project Address correspondence to Paul J. Wolters, MD University of California, San Francisco Department of Medicine Box 0111 San Francisco, CA 94143-0111 [email protected] or Joseph R. Arron, MD, PhD Genentech, Inc. MS 231C 1 DNA Way South San Francisco, CA 94080 [email protected] 1 METHODS Human lung tissue samples Tissues were obtained at UCSF from clinical samples from IPF patients at the time of biopsy or lung transplantation. All patients were seen at UCSF and the diagnosis of IPF was established through multidisciplinary review of clinical, radiological, and pathological data according to criteria established by the consensus classification of the American Thoracic Society (ATS) and European Respiratory Society (ERS), Japanese Respiratory Society (JRS), and the Latin American Thoracic Association (ALAT) (ref. 5 in main text). Non-diseased normal lung tissues were procured from lungs not used by the Northern California Transplant Donor Network. -

Development and Validation of a Protein-Based Risk Score for Cardiovascular Outcomes Among Patients with Stable Coronary Heart Disease
Supplementary Online Content Ganz P, Heidecker B, Hveem K, et al. Development and validation of a protein-based risk score for cardiovascular outcomes among patients with stable coronary heart disease. JAMA. doi: 10.1001/jama.2016.5951 eTable 1. List of 1130 Proteins Measured by Somalogic’s Modified Aptamer-Based Proteomic Assay eTable 2. Coefficients for Weibull Recalibration Model Applied to 9-Protein Model eFigure 1. Median Protein Levels in Derivation and Validation Cohort eTable 3. Coefficients for the Recalibration Model Applied to Refit Framingham eFigure 2. Calibration Plots for the Refit Framingham Model eTable 4. List of 200 Proteins Associated With the Risk of MI, Stroke, Heart Failure, and Death eFigure 3. Hazard Ratios of Lasso Selected Proteins for Primary End Point of MI, Stroke, Heart Failure, and Death eFigure 4. 9-Protein Prognostic Model Hazard Ratios Adjusted for Framingham Variables eFigure 5. 9-Protein Risk Scores by Event Type This supplementary material has been provided by the authors to give readers additional information about their work. Downloaded From: https://jamanetwork.com/ on 10/02/2021 Supplemental Material Table of Contents 1 Study Design and Data Processing ......................................................................................................... 3 2 Table of 1130 Proteins Measured .......................................................................................................... 4 3 Variable Selection and Statistical Modeling ........................................................................................ -

Graded Elevation of C-Jun in Schwann Cells in Vivo: Gene Dosage Determines Effects on Development, Remyelination, Tumorigenesis, and Hypomyelination
The Journal of Neuroscience, December 13, 2017 • 37(50):12297–12313 • 12297 Development/Plasticity/Repair Graded Elevation of c-Jun in Schwann Cells In Vivo: Gene Dosage Determines Effects on Development, Remyelination, Tumorigenesis, and Hypomyelination Shaline V. Fazal,1* XJose A. Gomez-Sanchez,1* Laura J. Wagstaff,1 Nicolo Musner,2 XGeorg Otto,3 Martin Janz,4 Rhona Mirsky,1 and Kristján R. Jessen1 1Department of Cell and Developmental Biology, University College London, London WC1E 6BT, United Kingdom, 2Enzo Life Sciences, 4415 Lausen, Switzerland, 3University College London Great Ormond Street Institute of Child Health, London WC1N1EH, United Kingdom, and 4Max Delbru¨ck Center for Molecular Medicine and Charite´, University Hospital Berlin, Campus Benjamin Franklin, 13092 Berlin, Germany Schwann cell c-Jun is implicated in adaptive and maladaptive functions in peripheral nerves. In injured nerves, this transcription factor promotes the repair Schwann cell phenotype and regeneration and promotes Schwann-cell-mediated neurotrophic support in models of peripheral neuropathies. However, c-Jun is associated with tumor formation in some systems, potentially suppresses myelin genes, and has been implicated in demyelinating neuropathies. To clarify these issues and to determine how c-Jun levels determine its function, we have generated c-Jun OE/ϩ and c-Jun OE/OE mice with graded expression of c-Jun in Schwann cells and examined these lines during development, in adulthood, and after injury using RNA sequencing analysis, quantitative electron microscopic morphometry, Western blotting, and functional tests. Schwann cells are remarkably tolerant of elevated c-Jun because the nerves of c-Jun OE/ϩ mice, in which c-Jun is elevated ϳ6-fold, are normal with the exception of modestly reduced myelin thickness. -

Signature Redacted Harvard-MIT Program in Health Sciences and Technology September 1St, 2015
THE ROLE OF OSTEOCYTES IN DISUSE AND MICROGRAVITY-INDUCED BONE LOSS byMASCUETINTTT AFTCHNOG Jordan Matthew Spatz B.S., M.S. University of Colorado at Boulder SEP 2 4 2015 Submitted to the LIBRARIES Harvard-MIT Program in Health Sciences and Technology in Partial Fulfillment of the Requirements for the Degree of I DOCTOR OF PHILOSOPHY IN HEALTH SCIENCES AND TECHNOLOGY at the MASSACHUSETTS INSTITUTE OF TECHNOLOGY September 2015 2015 Massachusetts Institute of Technology. All rights reserved. Signature of Author: Signature redacted Harvard-MIT Program in Health Sciences and Technology September 1st, 2015 Certified by: Signature redacted Mary L. Bouxsein, Ph.D. Associate Professor of Orthopedic Surgery, Harvard Medical School Thesis Supervisor A A Certified by: Signature redacted ___ i aola Divieti Pajevic, MD, Ph.D. Ass ciate Professor of Iolecular and Cell, Boston University Thesiy Supervisor Signature redacted Accepted byr. Emery N. Brown, MD, Ph.D. Director, Harv d-MIT Program in Health Sciences and Technology Professor of Computational Neuroscience & Health Sciences and Technology 2 The Role of Osteocytes in Disuse and Microgravity-Induced Bone Loss by Jordan Matthew Spatz B.S., M.S. University of Colorado at Boulder Submitted to the Harvard-MIT Health Sciences and Technology September 2015, in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Health Sciences and Technology Abstract A human mission to Mars will be physically demanding and presents a variety of medical risks to crewmembers. It has been recognized for over a century that loading is fundamental for bone health, and that reduced loading, as in prolonged bed rest or space flight, leads to bone loss. -

The Structure, Function and Evolution of the Extracellular Matrix: a Systems-Level Analysis
The Structure, Function and Evolution of the Extracellular Matrix: A Systems-Level Analysis by Graham L. Cromar A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Department of Molecular Genetics University of Toronto © Copyright by Graham L. Cromar 2014 ii The Structure, Function and Evolution of the Extracellular Matrix: A Systems-Level Analysis Graham L. Cromar Doctor of Philosophy Department of Molecular Genetics University of Toronto 2014 Abstract The extracellular matrix (ECM) is a three-dimensional meshwork of proteins, proteoglycans and polysaccharides imparting structure and mechanical stability to tissues. ECM dysfunction has been implicated in a number of debilitating conditions including cancer, atherosclerosis, asthma, fibrosis and arthritis. Identifying the components that comprise the ECM and understanding how they are organised within the matrix is key to uncovering its role in health and disease. This study defines a rigorous protocol for the rapid categorization of proteins comprising a biological system. Beginning with over 2000 candidate extracellular proteins, 357 core ECM genes and 524 functionally related (non-ECM) genes are identified. A network of high quality protein-protein interactions constructed from these core genes reveals the ECM is organised into biologically relevant functional modules whose components exhibit a mosaic of expression and conservation patterns. This suggests module innovations were widespread and evolved in parallel to convey tissue specific functionality on otherwise broadly expressed modules. Phylogenetic profiles of ECM proteins highlight components restricted and/or expanded in metazoans, vertebrates and mammals, indicating taxon-specific tissue innovations. Modules enriched for medical subject headings illustrate the potential for systems based analyses to predict new functional and disease associations on the basis of network topology. -

Cyclin D1: Mechanism and Consequence of Androgen Receptor Co-Repressor Activity in Prostatic Adenocarcinoma
UNIVERSITY OF CINCINNATI Date: April 1st, 2004 I, __________________Christin E. Petre_________________________, hereby submit this work as part of the requirements for the degree of: Doctor of Philosophy in: Cell and Molecular Biology It is entitled: Cyclin D1: Mechanism and Consequence of Androgen Receptor Co-repressor Activity in Prostatic Adenocarcinoma This work and its defense approved by: Chair: Karen E. Knudsen, Ph.D. Sohaib Khan, Ph.D. Kenji Fukasawa, Ph.D. Alvaro Puga, Ph.D. Linda Parysek, Ph.D. J. Alan Diehl, Ph.D. Robert Hennigan, Ph.D. CYCLIN D1: MECHANISM AND CONSEQUENCE OF ANDROGEN RECEPTOR CO-REPRESSOR ACTIVITY IN PROSTATIC ADENOCARCINOMA A dissertation submitted to the Division of Research and Advanced Studies of the University of Cincinnati in partial fulfillment of the requirements for the degree of DOCTORATE OF PHILOSOPHY (Ph.D.) in the Department of Cell Biology, Neurobiology, and Anatomy of the College of Medicine 2004 by Christin E. Petre B.A., Miami University, 2000 Committee Chair: Karen E. Knudsen, Ph.D. ABSTRACT It is increasingly evident that androgen receptor (AR) regulation plays a critical role in the development and progression of prostate cancer. We show that induction of cyclin D1 occurs upon ligand stimulation in androgen dependent prostatic adenocarcinoma (LNCaP) cells. Such induction results in the formation of active cyclin dependent kinase (CDK)-cyclin D1 complexes, phosphorylation of the rentinoblastoma tumor suppressor protein, and concomitant cell cycle progression. In addition, we find that cyclin D1 harbors a second cell cycle independent function responsible for restraining AR transactivation. We illustrate that cyclin D1 co-repressor activity is extremely potent, inhibiting receptor transactivation independently of cellular background, promoter context, co-activator over expression, ligand/non-ligand activators, and cancer predisposing AR mutations/polymorphisms. -

DMP1 Is a Target of Let-7 in Dental Pulp Cells
INTERNATIONAL JOURNAL OF MOLECULAR MEDICINE 30: 295-301, 2012 DMP1 is a target of let-7 in dental pulp cells JING YUE, BULING WU, JIE GAO, XIN HUANG, CHANGXIA LI, DANDAN MA and FUCHUN FANG Department of Stomatology, Nanfang Hospital, College of Stomatology, Southern Medical University, Guangzhou, P.R. China Received February 2, 2012; Accepted April 5, 2012 DOI: 10.3892/ijmm.2012.982 Abstract. Members of the let-7 family have been shown to play nant disorder of dentin formation, has been also mapped to a critical role in cell differentiation and tumorigenesis. However, the same region of the genome, indicating that DMP1 expres- potential targets of let-7 are still unclear. In the current study, sion is tightly linked genetically to its disease phenotype (9). we used bioinformatic analysis combined with DNA sequence Accordingly, DMP1 has been shown to play a prime role in analysis to identify potential let-7 targets. We discovered that dentin mineralization (10,11). Dentin and bone extracellular dentin matrix protein 1 (DMP1), which is a non-collagenous matrix (ECM) were shown to contain both the full length protein essential in the mineralization of dentin and bone, has DMP1 as well as its processed N-terminal (N-ter) (37 kDa) a let-7 binding site in its 3'-untranslated region. Furthermore, and C-terminal (C-ter) (57 kDa) fragments. It was shown to reporter assays demonstrated that the DMP1 3'-untranslated regulate the transcription of DSPP during early odontoblast region can be regulated directly by the members of let-7. Gene differentiation through binding of the promoter region through expression levels of let-7 and DMP1 were validated by qRT-PCR its carboxyl end (residues 420-489) and was implicated in of dental pulp cells cultured in a mineralizing medium. -

Modulates Plant Cell-Wall Composition
Arabidopsis Response Regulator 6 (ARR6) Modulates Plant Cell-Wall Composition and Disease Resistance Laura Bacete, Hugo Mélida, Gemma López, Patrick Dabos, Dominique Tremousaygue, Nicolas Denancé, Eva Miedes, Vincent Bulone, Deborah Goffner, Antonio Molina To cite this version: Laura Bacete, Hugo Mélida, Gemma López, Patrick Dabos, Dominique Tremousaygue, et al.. Ara- bidopsis Response Regulator 6 (ARR6) Modulates Plant Cell-Wall Composition and Disease Re- sistance. Molecular Plant-Microbe Interactions, American Phytopathological Society, 2020, 33 (5), pp.767-780. 10.1094/MPMI-12-19-0341-R. hal-03023355 HAL Id: hal-03023355 https://hal.archives-ouvertes.fr/hal-03023355 Submitted on 27 Nov 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Page 1 of 119 Molecular Plant-Microbe Interactions Laura Bacete et al. 1 Arabidopsis Response Regulator 6 (ARR6) modulates plant 2 cell wall composition and disease resistance 3 Laura Bacete1,2,#, Hugo Mélida1, Gemma López1, Patrick Dabos3, Dominique 4 Tremousaygue3, Nicolas Denancé3,4,†, Eva Miedes1,2, Vincent Bulone5,6, Deborah 5 Goffner4, and Antonio Molina1,2* 6 1Centro de Biotecnología y Genómica de Plantas, Universidad Politécnica de Madrid 7 (UPM)-Instituto Nacional de Investigación y Tecnología Agraria y Alimentaria (INIA), 8 Campus Montegancedo-UPM, 28223-Pozuelo de Alarcón (Madrid), Spain. -

Emerging Roles of DMP1 in Lung Cancer
Review Emerging Roles of DMP1 in Lung Cancer Kazushi Inoue,1,2 Takayuki Sugiyama,1,2 Pankaj Taneja,1,2 Rachel L. Morgan,1,2 and Donna P. Frazier1,2 Departments of 1Pathology and 2Cancer Biology, Wake Forest University Health Sciences, Medical Center Boulevard, Winston-Salem, North Carolina Abstract whereas in K-rasLA1, only the upstream copy of exon 1 is mutant (6). K-rasLA–mediated lung carcinogenesis was strikingly acceler- The Ras-activated transcription factor DMP1 can stimulate Arf À À À ated in mice of both p53+/ and p53 / backgrounds, reflecting the transcription to promote p53-dependent cell arrest. One LA recent study deepens the pathophysiologic significance of this frequent alteration of p53 in K-ras lung tumors and human lung DMP1 cancers (3, 6, 7). On the other hand, the Ink4a/Arf locus is not pathway in cancer,first,by identifying losses in human LA ARF/p53 frequently altered in these K-ras lung cancer models, and the lung cancers that lack mutations,and second,by LA demonstrating that Dmp1 deletions in the mouse are sufficient results of crossing K-ras transgenic mice with Arf and/or Ink4a- to promote K-ras–induced lung tumorigenesis via mechanisms null mice had not been previously reported. consistent with a disruption of Arf/p53 suppressor function. These findings prompt further investigations of the prognostic value of DMP1 alterations in human cancers and the Signaling Pathways Involving Dmp1 oncogenic events that can cooperate with DMP1 inactivation Cyclin D binding myb-like protein-1 (Dmp1; also called Dmtf1, to drive tumorigenesis. [Cancer Res 2008;68(12):4487–90] cyclin D binding myb-like transcription factor 1) was originally isolated in a yeast two-hybrid screen of a murine T-lymphocyte Genetic Alterations in Human Lung Cancer library with cyclin D2 as bait (8). -

Mmp2-Cleavage of Dmp1 Generates a Bioactive Peptide Promoting Differentiation of Dental Pulp Stem/Progenitor Cells
CEuropean Chaussain Cells et al.and Materials Vol. 18 2009 (pages 84-95) DOI: 10.22203/eCM.v018a08MMP-2 cleavage of DMP1 and dentin ISSN regeneratio 1473-2262n MMP2-CLEAVAGE OF DMP1 GENERATES A BIOACTIVE PEPTIDE PROMOTING DIFFERENTIATION OF DENTAL PULP STEM/PROGENITOR CELLS Catherine Chaussain1,2,3*, Asha Sarah Eapen1, Eric Huet4, Caroline Floris2,3, Sriram Ravindran1, Jianjun Hao1, Suzanne Menashi4, and Anne George1 1Department of Oral Biology, University of Illinois, Chicago, IL 60612, USA 2EA 2496, Université Paris Descartes, Paris, France 3 Assistance Publique-Hôpitaux de Paris, Hôpital Bretonneau, Odontology Department, Paris, France 4 Laboratoire CRRET, Université Paris Est, CNRS, Créteil, France Abstract Introduction Dentin Matrix Protein 1 (DMP1) plays a regulatory role in Dentin Matrix Protein 1 (DMP1) has been shown to play dentin mineralization and can also function as a signaling a central role in dentin mineralization (He and George molecule. MMP-2 (matrix metalloproteinase-2) is a 2004, He et al., 2003). Its carboxy-terminal domain rich predominant protease in the dentin matrix that plays a in aspartic acid and serine (ASARM; residues 408 to 429) prominent role in tooth formation and a potential role during may be responsible for the nucleation of hydroxyapatite the carious process. The possibility that MMP-2 can cleave (Gajjeraman et al., 2007, Rowe et al., 2000). DMP1 was DMP1 to release biologically active peptides was shown to be transported to the nuclear compartment and investigated in this study. DMP1, both in the recombinant was implicated in signaling functions (Narayanan et al., form and in its native state within the dentin matrix, was 2003). -

Supplementary Material Study Sample the Vervets Used in This
Supplementary Material Study sample The vervets used in this study are part of a pedigreed research colony that has included more than 2,000 monkeys since its founding. Briefly, the Vervet Research Colony (VRC) was established at UCLA during the 1970’s and 1980’s from 57 founder animals captured from wild populations on the adjacent Caribbean islands of St. Kitts and Nevis; Europeans brought the founders of these populations to the Caribbean from West Africa in the 17th Century 1. The breeding strategy of the VRC has emphasized the promotion of diversity, the preservation of the founding matrilines, and providing all females and most of the males an opportunity to breed. The colony design modeled natural vervet social groups to facilitate behavioral investigations in semi-natural conditions. Social groups were housed in large outdoor enclosures with adjacent indoor shelters. Each enclosure had chain link siding that provided visual access to the outside, with one or two large sitting platforms and numerous shelves, climbing structures and enrichments devices. The monkeys studied were members of 16 different social matrilineal groups, containing from 15 to 46 members per group. In 2008 the VRC was moved to Wake Forest School of Medicine’s Center for Comparative Medicine Research, however the samples for gene expression measurements in Dataset 1 (see below) and the MRI assessments used in this study occurred when the colony was at UCLA. Gene expression phenotypes Two sets of gene expression measurements were collected. Dataset 1 used RNA obtained from whole blood in 347 vervets, assayed by microarray (Illumina HumanRef-8 v2); Dataset 2 assayed gene expression by RNA-Seq, in RNA obtained from 58 animals, with seven tissues (adrenal, blood, Brodmann area 46 [BA46], caudate, fibroblast, hippocampus and pituitary) measured in each animal.