Kansas Journal of Medicine, Volume 11 Issue 1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ID 2 | Issue No: 4.1 | Issue Date: 29.10.14 | Page: 1 of 24 © Crown Copyright 2014 Identification of Corynebacterium Species
UK Standards for Microbiology Investigations Identification of Corynebacterium species Issued by the Standards Unit, Microbiology Services, PHE Bacteriology – Identification | ID 2 | Issue no: 4.1 | Issue date: 29.10.14 | Page: 1 of 24 © Crown copyright 2014 Identification of Corynebacterium species Acknowledgments UK Standards for Microbiology Investigations (SMIs) are developed under the auspices of Public Health England (PHE) working in partnership with the National Health Service (NHS), Public Health Wales and with the professional organisations whose logos are displayed below and listed on the website https://www.gov.uk/uk- standards-for-microbiology-investigations-smi-quality-and-consistency-in-clinical- laboratories. SMIs are developed, reviewed and revised by various working groups which are overseen by a steering committee (see https://www.gov.uk/government/groups/standards-for-microbiology-investigations- steering-committee). The contributions of many individuals in clinical, specialist and reference laboratories who have provided information and comments during the development of this document are acknowledged. We are grateful to the Medical Editors for editing the medical content. For further information please contact us at: Standards Unit Microbiology Services Public Health England 61 Colindale Avenue London NW9 5EQ E-mail: [email protected] Website: https://www.gov.uk/uk-standards-for-microbiology-investigations-smi-quality- and-consistency-in-clinical-laboratories UK Standards for Microbiology Investigations are produced in association with: Logos correct at time of publishing. Bacteriology – Identification | ID 2 | Issue no: 4.1 | Issue date: 29.10.14 | Page: 2 of 24 UK Standards for Microbiology Investigations | Issued by the Standards Unit, Public Health England Identification of Corynebacterium species Contents ACKNOWLEDGMENTS ......................................................................................................... -

(Publication Only) Corynebacterium Spp. and Arcanobacterium Haemolyticum Identification
R2737 Abstract (publication only) Corynebacterium spp. and Arcanobacterium haemolyticum identification. Usefulness of the Vitek 2 ANC card R. Soloaga*, N. Carrion, C. Barberis, M. Almuzara, L. Guelfand, J. Pidone, C. Vay (Buenos Aires, AR) Introduction: Corynebacterium diphtheriae and C.ulcerans may be isolated from suspected cases of classical diphtheria, cutaneous diphtheria and very rarely from other clinical infections. Non-diphtheric corynebacteria are opportunistic pathogens, especially in nosocomial setting where they have been associated with endocarditis, pulmonary infection, medical devices infections and urinary tract infection. A. haemolyticum infection manifests as exudative pharyngitis and tonsillitis accompanied by cervical lymphadenopathy and less commonly, the organism causes deep-seated infections and skin and soft-tissue infections Objective: The aim of this study was to determine the Vitek 2 ANC card (bioMèrieux, Marcy l’Etoile, France) performance for identification of the most frequently clinical relevant Corynebacterium species and Arcanobacterium haemolyticum Methods: Sixty-two unique clinical isolates (2 C. diphtheriae, 7 C. jeikeium, 10 C. amycolatum, 15 C.striatum, 12 C.urealyticum, 1 C.minutissimum, 8 C. pseudodiphtheriticum, 1 C. ulcerans and 6 Arcanobacterium haemolyticum) represented the 9 taxa included in the Vitek 2 ANC database and 6 strains represented related species not included in the database were analyzed in this study. All the strains were identified using 16S rRNA gene sequencing (16S) as the reference method. For Vitek identification, all the strains were isolated in pure culture on Columbia blood agar. After 24-48 h incubation to 35ºC in ambient air, a bacterial suspension was made in 0.45% aqueous ClNa and adjusted to a McFarland of 2.7-3.2 with Vitekk 2 Densicheck instrument (bioMérieux).The inoculated card was loaded into the Vitek 2C automated identification system according to the manufacturer´s instruction. -

Arcanobacterium Haemolyticum Type Strain (11018)
Lawrence Berkeley National Laboratory Recent Work Title Complete genome sequence of Arcanobacterium haemolyticum type strain (11018). Permalink https://escholarship.org/uc/item/03f632gf Journal Standards in genomic sciences, 3(2) ISSN 1944-3277 Authors Yasawong, Montri Teshima, Hazuki Lapidus, Alla et al. Publication Date 2010-09-28 DOI 10.4056/sigs.1123072 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Standards in Genomic Sciences (2010) 3:126-135 DOI:10.4056/sigs.1123072 Complete genome sequence of Arcanobacterium T haemolyticum type strain (11018 ) Montri Yasawong1, Hazuki Teshima2,3, Alla Lapidus2, Matt Nolan2, Susan Lucas2, Tijana Glavina Del Rio2, Hope Tice2, Jan-Fang Cheng2, David Bruce2,3, Chris Detter2,3, Roxanne Tapia2,3, Cliff Han2,3, Lynne Goodwin2,3, Sam Pitluck2, Konstantinos Liolios2, Natalia Ivanova2, Konstantinos Mavromatis2, Natalia Mikhailova2, Amrita Pati2, Amy Chen4, Krishna Palaniappan4, Miriam Land2,5, Loren Hauser2,5, Yun-Juan Chang2,5, Cynthia D. Jeffries2,5, Manfred Rohde1, Johannes Sikorski6, Rüdiger Pukall6, Markus Göker6, Tanja Woyke2, James Bristow2, Jonathan A. Eisen2,7, Victor Markowitz4, Philip Hugenholtz2, Nikos C. Kyrpides2, and Hans-Peter Klenk6* 1 HZI – Helmholtz Centre for Infection Research, Braunschweig, Germany 2 DOE Joint Genome Institute, Walnut Creek, California, USA 3 Los Alamos National Laboratory, Bioscience Division, Los Alamos, New Mexico, USA 4 Biological Data Management and Technology Center, Lawrence Berkeley National Laboratory, Berkeley, California, USA 5 Oak Ridge National Laboratory, Oak Ridge, Tennessee, USA 6 DSMZ - German Collection of Microorganisms and Cell Cultures GmbH, Braunschweig, Germany 7 University of California Davis Genome Center, Davis, California, USA *Corresponding author: Hans-Peter Klenk Keywords: obligate parasite, human pathogen, pharyngeal lesions, skin lesions, facultative anaerobe, Actinomycetaceae, Actinobacteria, GEBA Arcanobacterium haemolyticum (ex MacLean et al. -

Evaluation Ofapi Coryne System for Identifying Coryneform Bacteria
756 Y Clin Pathol 1994;47:756-759 Evaluation of API Coryne system for identifying coryneform bacteria J Clin Pathol: first published as 10.1136/jcp.47.8.756 on 1 August 1994. Downloaded from A Soto, J Zapardiel, F Soriano Abstract that are aerobe or facultatively aerobe, non- Aim-To identify rapidly and accurately spore forming organisms of the following gen- coryneform bacteria, using a commercial era: Corynebacterium, Listeria, Actinomyces, strip system. Arcanobacterium, Erysipelothrix, Oerskovia, Methods-Ninety eight strains of Cory- Brevibacterium and Rhodococcus. It also per- nebacterium species and 62 additional mits the identification of Gardnerella vaginalis strains belonging to genera Erysipelorix, which often has a diphtheroid appearance and Oerskovia, Rhodococcus, Actinomyces, a variable Gram stain. Archanobacterium, Gardnerella and We studied 160 organisms in total from dif- Listeria were studied. Bacteria were ferent species of the Corynebacterium genus, as identified using conventional biochemi- well as from other morphological related gen- cal tests and a commercial system (API- era or groups, some of them not included in Coryne, BioMerieux, France). Fresh rab- the API Coryne database. bit serum was added to fermentation tubes for Gardnerella vaginalis isolates. Results-One hundred and five out ofthe Methods 160 (65.7%) organisms studied were cor- The study was carried out on Gram positive rectly and completely identified by the bacilli belonging to the genera Coryne- API Coryne system. Thirty five (21.8%) bacterium, Erysipelothrix, Oerskovia, Rhodococcus, more were correctly identified with addi- Actinomyces, Arcanobacterium, Gardnerella and tional tests. Seventeen (10-6%) organisms Listeria included in the API Coryne database were not identified by the system and (table 1). -

Diversity and Prevalence of ANTAR Rnas Across Actinobacteria
bioRxiv preprint doi: https://doi.org/10.1101/2020.10.11.335034; this version posted October 11, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Diversity and prevalence of ANTAR RNAs across actinobacteria Dolly Mehta1,2 and Arati Ramesh1,+ 1National Centre for Biological Sciences, Tata Institute of Fundamental Research, GKVK Campus, Bellary Road, Bangalore, India 560065. 2SASTRA University, Tirumalaisamudram, Thanjavur – 613401. +Corresponding Author: Arati Ramesh National Centre for Biological Sciences GKVK Campus, Bellary Road Bangalore, 560065 Tel. 91-80-23666930 e-mail: [email protected] Running title: Identification of ANTAR RNAs across Actinobacteria Keywords: ANTAR protein:RNA regulatory system, structured RNA, actinobacteria 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.10.11.335034; this version posted October 11, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. ABSTRACT Computational approaches are often used to predict regulatory RNAs in bacteria, but their success is limited to RNAs that are highly conserved across phyla, in sequence and structure. The ANTAR regulatory system consists of a family of RNAs (the ANTAR-target RNAs) that selectively recruit ANTAR proteins. This protein-RNA complex together regulates genes at the level of translation or transcriptional elongation. -

The Porcine Nasal Microbiota with Particular Attention to Livestock-Associated Methicillin-Resistant Staphylococcus Aureus in Germany—A Culturomic Approach
microorganisms Article The Porcine Nasal Microbiota with Particular Attention to Livestock-Associated Methicillin-Resistant Staphylococcus aureus in Germany—A Culturomic Approach Andreas Schlattmann 1, Knut von Lützau 1, Ursula Kaspar 1,2 and Karsten Becker 1,3,* 1 Institute of Medical Microbiology, University Hospital Münster, 48149 Münster, Germany; [email protected] (A.S.); [email protected] (K.v.L.); [email protected] (U.K.) 2 Landeszentrum Gesundheit Nordrhein-Westfalen, Fachgruppe Infektiologie und Hygiene, 44801 Bochum, Germany 3 Friedrich Loeffler-Institute of Medical Microbiology, University Medicine Greifswald, 17475 Greifswald, Germany * Correspondence: [email protected]; Tel.: +49-3834-86-5560 Received: 17 March 2020; Accepted: 2 April 2020; Published: 4 April 2020 Abstract: Livestock-associated methicillin-resistant Staphylococcus aureus (LA-MRSA) remains a serious public health threat. Porcine nasal cavities are predominant habitats of LA-MRSA. Hence, components of their microbiota might be of interest as putative antagonistically acting competitors. Here, an extensive culturomics approach has been applied including 27 healthy pigs from seven different farms; five were treated with antibiotics prior to sampling. Overall, 314 different species with standing in nomenclature and 51 isolates representing novel bacterial taxa were detected. Staphylococcus aureus was isolated from pigs on all seven farms sampled, comprising ten different spa types with t899 (n = 15, 29.4%) and t337 (n = 10, 19.6%) being most frequently isolated. Twenty-six MRSA (mostly t899) were detected on five out of the seven farms. Positive correlations between MRSA colonization and age and colonization with Streptococcus hyovaginalis, and a negative correlation between colonization with MRSA and Citrobacter spp. -
C O N F E R E N C E 25 1 May 2019
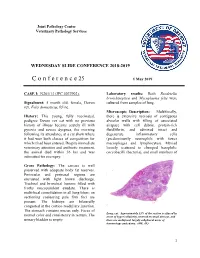
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2018-2019 C o n f e r e n c e 25 1 May 2019 CASE I: N261/13 (JPC 4037902). Laboratory results: Both Bordetella bronchiseptica and Mycoplasma felis were Signalment: 5 month old, female, Devon cultured from samples of lung. rex, Felis domesticus, feline. Microscopic Description: Multifocally, History: This young, fully vaccinated, there is extensive necrosis of contiguous pedigree Devon rex cat with no previous alveolar walls with filling of associated history of illness became acutely ill with airspace with cell debris, protein-rich pyrexia and severe dyspnea, the morning fluid/fibrin, and admixed intact and following its attendance at a cat show where degenerate inflammatory cells it had won both classes of competition for (predominantly neutrophils with fewer which it had been entered. Despite immediate macrophages and lymphocytes). Myriad veterinary attention and antibiotic treatment, loosely scattered to clumped basophilic the animal died within 36 hrs and was coccobacilli (bacteria), and small numbers of submitted for necropsy. Gross Pathology: The carcass is well preserved with adequate body fat reserves. Periocular and perinasal regions are encrusted with light brown discharge. Tracheal and bronchial lumens filled with frothy mucopurulent exudate. There is multifocal consolidation in all lung lobes: on sectioning coalescing pale firm foci are present. The kidneys are bilaterally congested at the cortico-medullary junction. The stomach contains mucus only. Feces of Lung, cat. Approximately 33% of the section is effaced by normal color and consistency in rectum. The areas of hyper\cellularity centered on small airways, and urinary bladder is empty. -

Arcanobacterium Pyogenes Sepsis in Farmer, Brazil
LETTERS Arcanobacterium g/dL, alanine aminotransferase 108 this grouping supported the phenotyp- U/L, and total bilirubin 2.57 mg/dL. ic identification. pyogenes Sepsis Blood and the ear secretion were sub- During the 7 days after admis- in Farmer, Brazil mitted for culture. Cefepime was pre- sion, the patient’s condition worsened, scribed, 2 g/twice a day. cefepime was withdrawn, and am- To the Editor: Arcanobacterium Three blood cultures grew gram- picillin 6 g/day plus gentamicin 240 pyogenes is a normal inhabitant of positive bacilli, initially identified mg/day were prescribed. The patient the mucous membranes of domestic as Corynebacterium spp., sensitive became afebrile, gradually recovered, animals, such as cattle, sheep, swine, to penicillin, ampicillin, ceftriaxone, and was discharged after 28 days of and goats (1). Diseases caused by this gentamicin, clindamycin, vancomycin, therapy. agent have been reported for persons and resistant to erythromycin, as deter- Our patient had otitis media that who live in rural areas and have un- mined by disk-diffusion test. Ear dis- progressed to sepsis, which was di- derlying illnesses such as cancer and charge culture grew Proteus mirabilis, agnosed by clinical, laboratory, and diabetes (2–4). A recent literature sensitive to β-lactams, cephalosporins, imaging findings. The causative agent review (3), elicited by a case of A. and aminoglycosides. Subcultures may have been undetectable in ear pyogenes endocarditis, found 13 un- of the gram-positive bacilli on sheep discharge if it was overshadowed by equivocal cases of human infection blood agar grew pinpointed, grayish, a strain of P. mirabilis, a fastidious with this agent; many patients had a β-hemolytic colonies, identified as A. -

The First Study of the Ovine Foot 16S Rrna-Based Microbiome
The ISME Journal (2011) 5, 1426–1437 & 2011 International Society for Microbial Ecology All rights reserved 1751-7362/11 www.nature.com/ismej ORIGINAL ARTICLE Ovine pedomics: the first study of the ovine foot 16S rRNA-based microbiome Leo A Calvo-Bado1, Brian B Oakley2,5, Scot E Dowd3, Laura E Green1,5, Graham F Medley1, Atiya Ul-Hassan1, Vicky Bateman1, William Gaze1, Luci Witcomb1, Rose Grogono-Thomas4, Jasmeet Kaler1, Claire L Russell4 and Elizabeth MH Wellington1 1School of Life Sciences, University of Warwick, Coventry, UK; 2USDA ARS, Richard Russell Research Center, 950 College Station Rd Athens, GA, USA; 3Research and Testing Laboratory, Lubbock, TX, USA and 4School of Clinical Veterinary, University of Bristol, Langford, UK We report the first study of the bacterial microbiome of ovine interdigital skin based on 16S rRNA by pyrosequencing and conventional cloning with Sanger-sequencing. Three flocks were selected, one a flock with no signs of footrot or interdigital dermatitis, a second flock with interdigital dermatitis alone and a third flock with both interdigital dermatitis and footrot. The sheep were classified as having either healthy interdigital skin (H) and interdigital dermatitis (ID) or virulent footrot (VFR). The ovine interdigital skin bacterial community varied significantly by flock and clinical condition. The diversity and richness of operational taxonomic units was greater in tissue from sheep with ID than H or VFR-affected sheep. Actinobacteria, Bacteriodetes, Firmicutes and Proteobacteria were the most abundant phyla comprising 25 genera. Peptostreptococcus, Corynebacterium and Staphylococcus were associated with H, ID and VFR, respectively. Sequences of Dichelobacter nodosus, the causal agent of ovine footrot, were not amplified because of mismatches in the 16S rRNA universal forward primer (27F). -

Septic Arthritis Due to Arcanobacterium Haemolyticum
Indian Journal of Medical Microbiology, (2005) 23 (1):63-65 Case Report SEPTIC ARTHRITIS DUE TO ARCANOBACTERIUM HAEMOLYTICUM R Goyal, *NP Singh, M Mathur Abstract Diphtheroids or “coryneform” bacilli are usually considered to be nonpathogenic “normal flora” of human skin and mucous membranes. Because bacterial cultures are frequently contaminated with these organisms the correct diagnosis and treatment may be delayed by the failure to recognize serious infections caused by them. Few confirmed cases of orthopaedic infections due to Arcanobacterium haemolyticum infection have been reported, partly because of inadequate identification of this bacterium. We report a case of septic arthritis due to A. haemolyticum. Key words: Arcanobacterium haemolyticum, septic arthritis Arcanobacterium haemolyticum, formerly known as left knee with decreased range of motion. The peripheral Corynebacterium haemolyticum was first isolated from blood leukocyte count was 12,000/mm3 with 84% nasopharynx and skin of American soldiers in the south neutrophils and 16% monocytes. ESR (69 mm/hour) and pacific in 1946. It was elevated to the genus CRP (8.9 mg/dL) values were elevated. Knee radiograph Arcanobacterium on the basis of genetic analysis in showed soft tissue swelling with joint narrowing and 1982, and has been associated with pharyngitis, osteophyte formation. Synovial fluid aspirated from the recurrent throat infections, wound infections, affected joint revealed total leukocyte count of 98,000/ septicaemia, endocarditis and osteomyelitis.1 Although mm3 with 98% segmented neutrophils and 2% it is the etiological agent of distinct human infections, monocytes. Gram stain of the aspirated fluid showed the organism is frequently overlooked, probably because gram positive bacilli along with pus cells. -

Microbiology Division – Milwaukee Health
MICROBIOLOGY SECTION – MILWAUKEE HEALTH DEPARTMENT M O N T H L Y R E P O R T FEBRUARY 2007 Vol. 12, No. 2 Ajaib Singh, D.V.M., Ph. D. MICROBIOLOGY REPORT: The February 2007 issue of Microbiology Monthly Report, Volume 12, presents the laboratory diagnosis of some of the infectious diseases, the reference microbiology work done in this laboratory during January 2007 and new cases of syphilis in Milwaukee during December 2006. Information on the laboratory diagnosed mycobacterial infections in Wisconsin during December is also included. Legionnaires Disease (January 2007) No positive case detected. Pertussis (Whooping cough) January 2007 No positive case detected. Syphilis (January 2007) Test Number Positive Test Number Positive RPR 1 TP-PA 9 VDRL 22 DARKFIELD 0 New Cases of Syphilis The Wisconsin Division of Health has reported 9 new cases (early stages) of syphilis during December, 2006 in Milwaukee. The median age of early syphilis cases is 34.0 years (range: 17-59 years). Morbidity distributions of the disease reported in this and the corresponding month of the previous year are as follows: New Cases of Syphilis (December 2006 and December 2005) Number of Cases Stage December 2006 December 2005 Primary syphilis 2 1 Secondary syphilis 2 2 Early latent 5 0 Late latent 0 0 Total 9 3 Gonorrhea (January 2007) Number Decreased Susceptibility (DS) / Resistance (R) Antibiotics Tested Ciprofloxacin Ceftriaxone Spectinomycin Azithromycin 60 7 (R) 0 0 0 Gonorrhea from Other Sources (Aurora Consolidated Labs) January 2007 Number Decreased Susceptibility (DS) / Resistance (R) Antibiotics Tested Ciprofloxacin Ceftriaxone Spectinomycin Azithromycin 5 3 (R) 0 0 0 Isolates Other Than N. -

Arcanobacterium Haemolyticum
P.O. Box 131375, Bryanston, 2074 Ground Floor, Block 5 Bryanston Gate, 170 Curzon Road Bryanston, Johannesburg, South Africa www.thistle.co.za Tel: +27 (011) 463 3260 Fax: +27 (011) 463 3036 Fax to Email: + 27 (0) 86-557-2232 e-mail : [email protected] Please read this section first The HPCSA and the Med Tech Society have confirmed that this clinical case study, plus your routine review of your EQA reports from Thistle QA, should be documented as a “Journal Club” activity. This means that you must record those attending for CEU purposes. Thistle will not issue a certificate to cover these activities, nor send out “correct” answers to the CEU questions at the end of this case study. The Thistle QA CEU No is: MT-2015/009. Each attendee should claim THREE CEU points for completing this Quality Control Journal Club exercise, and retain a copy of the relevant Thistle QA Participation Certificate as proof of registration on a Thistle QA EQA. MICROBIOLOGY LEGEND CYCLE 38 ORGANISM 1 Arcanobacterium haemolyticum Arcanobacterium haemolyticum was first described by MacLean et al. in 1946 as a pathogen in cases of exudative pharyngitis and soft-tissue infections. In 1982 the previously named Corynebacterium haemolyticum was included in a new genus to reflect major differences in cell wall components and chemotaxonomic characters, the genus Arcanobacterium. Currently, there are nine identified species within this genus of which A. haemolyticum, A. pyogenes and A. bernardiae have been recovered from clinical specimens. It is a catalase-negative, aerobic, beta-haemolytic, nonmotile, irregular gram-positive to gram-variable rod that may be misidentified as Streptococcus species, Corynebacterium species, or A.