MUCC-Background
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Provincial-Program-Final.Pdf
Table of Contents Introduction .................................................................................................................................... 2 Voice .............................................................................................................................................. 10 Piano ............................................................................................................................................. 18 Strings ........................................................................................................................................... 26 Brass, Woodwind & Percussion .................................................................................................... 29 Musical Theatre ............................................................................................................................ 31 Speech Arts ................................................................................................................................... 36 Excellence ...................................................................................................................................... 38 Scholarships .................................................................................................................................. 50 1 Introduction 2 ESTABLISHED IN 1908 Incorporated under the Non-Profit Corporations Act HONORARY PATRONS His Honour the Honourable Russ Mirasty, Lieutenant Governor of Saskatchewan The Honourable Scott Moe, Premier of Saskatchewan -
West Michigan Pike Route but Is Most Visible Between Whitehall and Shelby
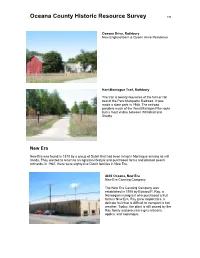
Oceana County Historic Resource Survey 198 Oceana Drive, Rothbury New England Barn & Queen Anne Residence Hart-Montague Trail, Rothbury The trail is twenty-two miles of the former rail bed of the Pere Marquette Railroad. It was made a state park in 1988. The railroad parallels much of the West Michigan Pike route but is most visible between Whitehall and Shelby. New Era New Era was found in 1878 by a group of Dutch that had been living in Montague serving as mill hands. They wanted to return to an agrarian lifestyle and purchased farms and planted peach orchards. In 1947, there were eighty-five Dutch families in New Era. 4856 Oceana, New Era New Era Canning Company The New Era Canning Company was established in 1910 by Edward P. Ray, a Norwegian immigrant who purchased a fruit farm in New Era. Ray grew raspberries, a delicate fruit that is difficult to transport in hot weather. Today, the plant is still owned by the Ray family and processes green beans, apples, and asparagus. Oceana County Historic Resource Survey 199 4775 First Street, New Era New Era Reformed Church 4736 First Street, New Era Veltman Hardware Store Concrete Block Buildings. New Era is characterized by a number of vernacular concrete block buildings. Prior to 1900, concrete was not a common building material for residential or commercial structures. Experimentation, testing and the development of standards for cement and additives in the late 19th century, led to the use of concrete a strong reliable building material after the turn of the century. Concrete was also considered to be fireproof, an important consideration as many communities suffered devastating fires that burned blocks of their wooden buildings Oceana County Historic Resource Survey 200 in the late nineteenth century. -

Qdma's Whitetailreport 2020
DEER HARVEST TRENDS qdma ’s PART 1: WhitetailReport 2020 An annual report on the status of white-tailed deer – the foundation of the hunting industry in North America Compiled and Written by the QDMA Staff Field to Fork mentor Charles Evans (right) congratulates Andy Cunningham on his first deer. WhitetailReport Special thanks to all of these QDMA Sponsors, Partners and Supporters for helping enable our mission: ensuring the future of white-tailed deer, wildlife habitat and our hunting heritage. Please support these companies that support QDMA. For more information on how to become a corporate supporter of QDMA, call 800-209-3337. Sponsors Partners Rec onnect w ith Real F ood Supporters 2 • QDMA's Whitetail Report 2020 QDMA.com • 3 WhitetailReport QDMA MISSION: TABLE OF CONTENTS QDMA is dedicated to ensuring the future of white-tailed deer, wildlife PART 1: DEER HARVEST TRENDS PART 3: QDMA MISSION & ANNUAL REPORT habitat and our hunting heritage. Antlered Buck Harvest ....................................................6 QDMA: Ensuring the Future of Deer Hunting ................40 QDMA NATIONAL STAFF Age Structure of the Buck Harvest ..................................8 2019 QDMA Advocacy Update ......................................41 Antlerless Deer Harvest ................................................10 QDMA Mission: Progress Report ...................................42 Chief Executive Officer Age Structure of the Antlerless Harvest ........................12 QDMA Communications Update ...................................43 Brian -

El Visual Kei Como Producto Cultural Y Su Huella En La Cultura Popular
FACULTAD DE TRADUCCIÓN E INTERPRETACIÓN GRADO EN ESTUDIOS DE ASIA ORIENTAL TRABAJO DE FIN DE GRADO Curso 2015-2016 EL VISUAL KEI COMO PRODUCTO CULTURAL Y SU HUELLA EN LA CULTURA POPULAR Cecilia Isabel Sanz Martínez 1244795 TUTOR Roberto Figliulo Barcelona, junio de 2016 DATOS DEL TFG El Visual Kei como producto cultural y su huella en la cultura popular. El Visual Kei com a producte cultural i la seva empremta en la cultura popular. Visual Kei as a cultural product and its imprint on popular culture. Autor: Cecilia Isabel Sanz Martínez. Tutor: Roberto Figliulo. Centro: Facultad de Traducción e Interpretación. Universidad Autónoma de Barcelona. Estudios: Estudios de Asia Oriental. Curso Académico: 2015-2016 Palabras clave // Paraules clau // Key words Visual Kei, cultura popular, Japón, música, rock, metal // Visual Kei, cultura popular, Japó, música, rock, metal // Visual Kei, popular culture, Japan, music, rock, metal. Resumen del TFG El Visual Kei es una escena musical nacida en y casi exclusiva de Japón, cuya característica principal es que el componente visual o estético tiene tanto peso como el componente musical. Se trata de una escena muy activa y con mucha variedad tanto musical como estética. En este TFG se analiza el Visual Kei como producto cultural, siguiendo un esquema histórico. Empezando desde los movimientos musicales y culturales que han contribuido a su surgimiento como el heavy metal, el glam y el punk; observando la escena que sería su caldo de cultivo, hasta su nacimiento; y viendo las claves de cada etapa de su evolución, desde los años 90 hasta hoy. Además, se observa cuál ha sido el impacto del Visual Kei en la cultura popular japonesa, y cuál ha sido su recepción en el resto del mundo. -

Washtenaw County, Michigan
L A N D S C A P E S T E W A R D S H I P P L A N: Washtenaw County, Michigan PREPARED BY JACQUELINE COURTEAU THE STEWARDSHIP NETWORK DATE MARCH 2017 Landscape Stewardship Plan for Washtenaw County, Michigan This Landscape Stewardship Plan is funded in part through a Fiscal Year 2015 Landscape Scale Restoration grant for “Developing Nine Landscape Stewardship Plans in Michigan” (15-DG- 11420004-175). The United States Forest Service, State and Private Forestry granted $336,347 in federal funds to the Michigan Department of Natural Resources, Forest Resources Division which along with its partners provided $337,113 in matching non-federal funds. The Department of Natural Resources administered the grant in partnership with The Nature Conservancy, Huron Pines, The Stewardship Network and the Remote Environmental Assessment Laboratory. In accordance with Federal law and the U.S. Department of Agriculture policy, this institution is prohibited from discriminating on the basis of race, color, national origin, sex, age, or disability. Acknowledgements We would like to thank the United States Forest Service for funding the project and the DNR Forest Stewardship staff (especially Mike Smalligan) for coordination. We are grateful for the information provided by many private landowners, public agencies, and nonprofit organization staff. Josh Liesen from Huron Pines provided much of the material for the Project Introduction section of this document, and all the individuals who shared their stories with us. Cover photo by Steve Parrish Author Contact: Jacqueline Corteau The Stewardship Network 416 Longshore Drive Ann Arbor, MI 48825 (734) 395-4483 [email protected] www.stewardshipnetwork.org | 2 Table of Contents 1. -

Rage in Eden Records, Po Box 17, 78-210 Bialogard 2, Poland [email protected]
RAGE IN EDEN RECORDS, PO BOX 17, 78-210 BIALOGARD 2, POLAND [email protected], WWW.RAGEINEDEN.ORG Artist Title Label HAUSCHKA ROOM TO EXPAND 130701/FAT CAT CD RICHTER, MAX BLUE NOTEBOOKS, THE 130701/FAT CAT CD RICHTER, MAX SONGS FROM BEFORE 130701/FAT CAT CD ASCENSION OF THE WAT NUMINOSUM 13TH PLANET RECORDS CD MINISTRY COVER UP 13TH PLANET RECORDS CD MINISTRY LAST SUCKER, THE 13TH PLANET RECORDS CD MINISTRY LAST SUCKER, THE 13TH PLANET RECORDS LTD MINISTRY RIO GRANDE BLOOD 13TH PLANET RECORDS CD MINISTRY RIO GRANDE DUB YA 13TH PLANET RECORDS CD PRONG POWER OF THE DAMAGER 13TH PLANET RECORDS CD REVOLTING COCKS COCKED AND LOADED 13TH PLANET RECORDS CD REVOLTING COCKS COCKTAIL MIXXX 13TH PLANET RECORDS CD BERNOCCHI, ERALDO/FE MANUAL 21ST RECORDS CD BOTTO & BRUNO/THE FA BOTTO & BRUNO/THE FAMILY 21ST RECORDS CD FLOWERS OF NOW INTUITIVE MUSIC LIVE IN COLOGNE 21ST RECORDS CD LOST SIGNAL EVISCERATE 23DB RECORDS CD SEVENDUST ALPHA 7 BROS RECORDS CD SEVENDUST CHAPTER VII: HOPE & SORROW 7 BROS RECORDS CD A BLUE OCEAN DREAM COLD A DIFFERENT DRUM MCD A BLUE OCEAN DREAM ON THE ROAD TO WISDOM A DIFFERENT DRUM CD B!MACHINE ALTERNATES AND REMIXES A DIFFERENT DRUM CD B!MACHINE EVENING BELL, THE A DIFFERENT DRUM CD B!MACHINE FALLING STAR, THE A DIFFERENT DRUM CD B!MACHINE MACHINE BOX A DIFFERENT DRUM BOX BLUE OCTOBER ONE DAY SILVER, ONE DAY GOLD A DIFFERENT DRUM CD BLUE OCTOBER UK INCOMING 10th A DIFFERENT DRUM 2CD CAPSIZE A PERFECT WRECK A DIFFERENT DRUM CD COSMIC ALLY TWIN SUN A DIFFERENT DRUM CD COSMICITY ESCAPE POD FOR TWO A DIFFERENT DRUM CD DIGNITY -

2 Stadtmagazin Hameln Und Weserbergland
Stadtmagazin Hameln und Weserbergland Kostenlos Ausgabe Mai 2009 2 1 Beratung 1 Einbau 1 Service car akustik Hameln Hastenbecker Weg 33 31785 Hameln 1 Tel.: 0 51 51 / 80 80 Mail: [email protected] 31.05.09. www.car-akustik.hm 31.05.09. Stadtmagazin Hameln und Weserbergland Kostenlos Ausgabe Mai 2009 2 3 Jahre Bahnhof Hameln Große Jubiläumsparty Fashion Heiße Tipps für den Jeanskauf Honky Tonk Fotos vom Kneipenfestival SOLsnap MEETS VENEDIG 2 !" # " "$ #$ "# % &' 4 www.solsnap.com 2 VORWORT Liebe Leser, Looking forward Kopf hoch - da ist sie die lang erwartete Meldung: Ab Mai geht es wieder auf- Im nächsten Magazin: wärts! Nicht nur die Temperaturen sind gemeint – nein auch die Wirtschaft, insbesondere die Antriebstechnik. Und das sagt immerhin einer der es wissen SOLsnap meets BERLIN muss, nämlich Hannes Hesse vom schwer gebeutelten Branchenverband der deutschen Maschinenbauer. Wollen wir hoffen, dass er mit seiner vorsichtig po- Das nächste sitiven Einschätzung der Wirtschaftslage im Rahmen der Hannover Messe Recht SOLsnap Magazin erscheint behält und „Made in Germany“ wieder exportiert wird. am 2.6.2009 Redaktions- und Anzeigenschluss Es würde zumindest die Stimmung im Hamelner Feierjahr 2009 aufhellen. Nach ist der 22.05.2009, 12 Uhr der Auftaktveranstaltung Mystica Hamelon, geht es Schlag auf Schlag. Bereits Anfang Mai rückt die Altstadt in den Fokus der Feierlichkeiten - der Hamelner Ver- fügung folgt bald ein Event der Extraklasse. Zum Tag der Niedersachsen werden in Hameln 300.000 Gäste erwartet! Und da wäre eine trübe Stimmung sicher keine positive Werbung der Stadt des Lächelns - auch wenn das Marketing zum Jubiläumsjahr bewusst auf den düsteren Hintergrund der Sage setzt. -

World Bank Document
Public Disclosure Authorized Public Disclosure Authorized [ue: I Perspectives on Religion, Education and Social Cohesion Public Disclosure Authorized THE WORLD BANK Public Disclosure Authorized Asian Interfaith Dialogue: Perspectives on Religion, Education and Social Cohesion Edited by Syed Farid Alatas Lim Teck Ghee Kazuhide Kuroda H THE WORLD BANK Copyright 0 2003 by Centre for Research on Islamic and Malay Affairs (RIMA) and The World Bank Centre for Research on Islamic and Malay Affairs (RIMA) 150 Changi Road #04-06/07 Guthrie Building Singapore 419972 The World Bank 1818 H Street, N.W. Washington, D.C. 20433, USA All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, ~ ~ mechanical, photocopying, recording or otherwise, without the prior consent of the Centre for Research on Islamic and Malay Affairs (RIMA) and The World Bank. The responsibility for facts and opinions expressed in this publication rests exclusively with the contributors and their interpretations do not necessarily reflect the views or the policy of the publishers or their supporters. ISBN: 981-04-9475-0 Cover Design by Wee Hong Loong, Temasek Polytechnic. Printed in Singapore by COS Printers Pte Ltd. CONTENTS Foreword iv .. Preface Vlll Abbreviations and Acronyms X Introduction xii Syed Farid Alatas Addresses Chiang Chie Foo Permanent Secretarj Ministry of Education (Guest-of-Honour) Darke M. Sani Chairman, Centre for Research on Islamic and Malay Afairs (RTMA) Lim Teck -

PDF // Visual Kei Artists » Read
QF3YUFXVVI \ Visual kei artists « eBook Visual kei artists By Source Reference Series Books LLC Apr 2013, 2013. Taschenbuch. Book Condition: Neu. 246x189x7 mm. Neuware - Source: Wikipedia. Pages: 121. Chapters: X Japan, Buck-Tick, Dir En Grey, Alice Nine, Miyavi, Hide, Nightmare, The Gazette, Glacier, Merry, Luna Sea, Ayabie, Rentrer en Soi, Versailles, D'espairsRay, Malice Mizer, Girugamesh, Psycho le Cému, An Cafe, Penicillin, Laputa, Vidoll, Phantasmagoria, Mucc, Plastic Tree, Onmyo-Za, Panic Channel, Blood, The Piass, Megamasso, Tinc, Kagerou, Sid, Uchuu Sentai NOIZ, Fanatic Crisis, Moi dix Mois, Pierrot, Zi:Kill, Kagrra, Doremidan, Anti Feminism, Eight, Sug, Kuroyume, 12012, LM.C, Sadie, Baiser, Strawberry song orchestra, Unsraw, Charlotte, Dué le Quartz, Baroque, Silver Ash, Schwarz Stein, Inugami Circus-dan, Cali Gari, GPKism, Guniw Tools, Luci'fer Luscious Violenoue, Mix Speakers, Inc, Aion, Lareine, Ghost, Luis-Mary, Raphael, Vistlip, Deathgaze, Duel Jewel, El Dorado, Skin, Exist Trace, Cascade, The Dead Pop Stars, D'erlanger, The Candy Spooky Theater, Aliene Ma'riage, Matenrou Opera, Blam Honey, Kra, Fairy Fore, BIS, Lynch, Shazna, Die in Cries, Color, D=Out, By-Sexual, Rice, Dio - Distraught Overlord, Kaya, Jealkb, Genkaku Allergy, Karma Shenjing, L'luvia, Devil Kitty, Nheira. Excerpt: X Japan Ekkusu Japan ) is a Japanese heavy metal band founded in 1982 by Toshimitsu 'Toshi' Deyama and Yoshiki Hayashi. Originally named X ( ), the... READ ONLINE [ 2.39 MB ] Reviews This ebook can be worthy of a read, and much better than other. I have read and i am certain that i am going to planning to go through again once again in the future. You may like just how the writer compose this book. -

Beria Purge Held As Start Tha Houra Wul Be from 1 to 9 P
■■ ' ■ 'Vi \ • / v,-'\T b ■ . ■ ■ »■■ THURSDAY. JULY 9 , 19BS ■'I- Mmrlfwter ^Etif Manchmjfer Day^f^bValue Contm , .-V <* = ■'4' < Mias Ruth Steinmuallsr, aiaaist- Avtimia Dolly Nat Praaa Run TheWaathtr ant Chfldren’a librarian at the Attending Cxinp Planners Slate Pafaaaat at I). R. Waathav Rumaa AbbiutTowti Mary Cheney Ubrary, ia PW 'Nm Wm A Rneea-- her vaeatloik visiting her Irrenf- M y i . 1888 CIrar. raatto i^ eaal taaIgM. Tirk U . Or**ory M. Pltonl*k et parenta and other relatives In Open Session racksvUl*. Pa.. who«® wife. Tv«tt«, , ,, .... .. -p . , -- - 10,707 M r, littto rhaaga to Imiiparatara UVM at n EUnbeth drivf, haa ! ' ■ ^ ' 1 ( natarday, \ baen awardad tha bronia atar Mias Jacqueline R. McHugh of CommiBBion SchedulcB / imaMr af Mw AneH medal for maritorioiia aar>dca In 622 North Main street will « • »' rMM al arepNONw Manchester— A City of VUlage Charm ried Ibon In New T«»«'*J„Clty H e a r in g at 8 ip. m . in Korea. ^ Foster B. Stough of '12 Sisson street, East Hartford. Mias Mc ■ -.V. Municipal Building /Av/^; Beginnlnr Uila week and every "'^-'"^'’^''^iilbtoaaUlae AevartMag aa Pabt 14) MANCHESTER, CONN„ FRIDAY, JULY 10, 1933 (SIXTEEN PAGES) PRICE FIVE CBNIS week thereafter until after Labor Hugh, a hattve of Norwalk, la the VOL. LXXn, NO. 238 Day both the Mary Cheney and daughter of John T. and Sarah ^ A public hearing will he held by . WhiUm llbrariea will cloae at 12 Sheehan McHugh. the. Town Planning Oommiaslon o'clock noon on Saturdaya. The '-’ •'.■fc'inV, tonight.at 8 o'clock to the hearing I Need At HALE’S Self Serve aummer achedule of the Mary Mias Terry Ivaniskl, who has room of the .Municipal Building to Cheney Library will be from • a. -

TRANSCULTURAL SPACES in SUBCULTURE: an Examination of Multicultural Dynamics in the Japanese Visual Kei Movement
TRANSCULTURAL SPACES IN SUBCULTURE: An examination of multicultural dynamics in the Japanese visual kei movement Hayley Maxime Bhola 5615A031-9 January 10, 2017 A master’s thesis submitted to the Graduate School of International Culture and Communication Studies Waseda University in partial fulfillment of the requirements for the degree of Master of Arts TRANSCULTURAL SPACES IN SUBCULTURE 2 Abstract of the Dissertation The purpose of this dissertation was to examine Japanese visual kei subculture through the theoretical lens of transculturation. Visual kei (ヴィジュアル系) is a music based subculture that formed in the late 1980’s in Japan with bands like X Japan, COLOR and Glay. Bands are recognized by their flamboyant (often androgynous appearances) as well as their theatrical per- formances. Transculturation is a term originally coined by ethnographer Fernando Ortiz in re- sponse to the cultural exchange that took place during the era of colonization in Cuba. It de- scribes the process of cultural exchange in a way that implies mutual action and a more even dis- tribution of power and control over the process itself. This thesis looked at transculturation as it relates to visual kei in two main parts. The first was expositional: looking at visual kei and the musicians that fall under the genre as a product of transculturation between Japanese and non- Japanese culture. The second part was an effort to label visual kei as a transcultural space that is able to continue the process of transculturation by fostering cultural exchange and development among members within the subculture in Japan. Chapter 1 gave a brief overview of the thesis and explains the motivation behind conduct- ing the research. -
Numero Kansi Arvostelut Artikkelit / Esittelyt Mielipiteet Muuta 1 (1/2005
Numero Kansi Arvostelut Artikkelit / esittelyt Mielipiteet Muuta -Full Metal Panic (PAN Vision) (Mauno Joukamaa) -DNAngel (ADV) (Kyuu Eturautti) -Final Fantasy Unlimited (PAN Vision) (Jukka Simola) -Kissankorvanteko-ohjeet (Einar -Neon Genesis Evangelion, 2s (Pekka Wallendahl) - Pääkirjoitus: Olennainen osa animen ja -Jin-Roh (Future Film) (Mauno Joukamaa) Karttunen) -Gainax, 1s (?, oletettavasti Pekka Wallendahl) mangan suosiota on hahmokulttuuri (Jari -Manga! Manga! The world of Japanese comics (Kodansha) (Mauno Joukamaa) -Idän ihmeitä: Natto (Jari Lehtinen) 1 -Megumi Hayashibara, 1s (?, oletettavasti Pekka Wallendahl) Lehtinen, Kyuu Eturautti) -Salapoliisi Conan (Egmont) (Mauno Joukamaa) -Kotimaan katsaus: Animeunioni, -Makoto Shinkai, 2s (Jari Lehtinen) - Kolumni: Anime- ja mangakulttuuri elää (1/2005) -Saint Tail (Tokyopop) (Jari Lehtinen) MAY -Final Fantasy VII: Advent Children, 1s (Miika Huttunen) murrosvaihetta, saa nähdä tuleeko siitä -Duel Masters (korttipeli) (Erica Christensen) -Fennomanga-palsta alkaa -Kuukauden klassikko: Saiyuki, 2s (Jari Lehtinen) valtavirta vai floppi (Pekka Wallendahl) -Duel Masters: Sempai Legends (Erica Christensen) -Animea TV:ssä alkaa -International Ragnarök Online (Jukka Simola) -Star Ocean: Till The End Of Time (Kyuu Eturautti) -Star Ocean EX (Geneon) (Kyuu Eturautti) -Neon Genesis Evangelion (PAN Vision) (Mikko Lammi) - Pääkirjoitus: Cosplay on harrastajan -Spiral (Funimation) (Kyuu Eturautti) -Cosplay, 4s (Sefie Rosenlund) rakkaudenosoitus (Mauno Joukamaa) -Hopeanuoli (Future Film) (Jari Lehtinen)