Bleeds and Bruises in Children with Haemophilia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Skin Injuries – Can We Determine Timing and Mechanism?
Skin injuries – can we determine timing and mechanism? Jo Tully VFPMS Seminar 2016 What skin injuries do we need to consider? • Bruising • Commonest accidental and inflicted skin injury • Basic principles that can be applied when formulating opinion • Abrasions • Lacerations }we need to be able to tell the difference • Incisions • Stabs/chops • Bite marks – animal v human / inflicted v ‘accidental’ v self-inflicted Our role…. We are often/usually/always asked…………….. • “What type of injury is it?” • “When did this injury occur?” • “How did this injury occur?” • “Was this injury inflicted or accidental?” • IS THIS CHILD ABUSE? • To be able to answer these questions (if we can) we need knowledge of • Anatomy/physiology/healing - injury interpretation • Forces • Mechanisms in relation to development, plausibility • Current evidence Bruising – can we really tell which bruises are caused by abuse? Definitions – bruising • BLUNT FORCE TRAUMA • Bruise =bleeding beneath intact skin due to BFT • Contusion = bruise in deeper tissues • Haematoma - extravasated blood filling a cavity (or potential space). Usually associated with swelling • Petechiae =Pinpoint sized (0.1-2mm) hemorrhages into the skin due to acute rise in venous pressure • medical causes • direct forces • indirect forces Medical Direct Indirect causes mechanical mechanical forces forces Factors affecting development and appearance of a bruise • Properties of impacting object or surface • Force of impact • Duration of impact • Site - properties of body region impacted (blood supply, -
Immune Thrombocytopenia Purpura (ITP)
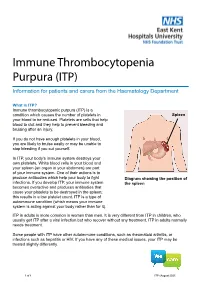
Immune Thrombocytopenia Purpura (ITP) Information for patients and carers from the Haematology Department What is ITP? Immune thrombocytopenic purpura (ITP) is a condition which causes the number of platelets in Spleen your blood to be reduced. Platelets are cells that help blood to clot and they help to prevent bleeding and bruising after an injury. If you do not have enough platelets in your blood, you are likely to bruise easily or may be unable to stop bleeding if you cut yourself. In ITP, your body’s immune system destroys your own platelets. White blood cells in your blood and your spleen (an organ in your abdomen) are part of your immune system. One of their actions is to produce antibodies which help your body to fight Diagram showing the position of infections. If you develop ITP, your immune system the spleen becomes overactive and produces antibodies that cause your platelets to be destroyed in the spleen; this results in a low platelet count. ITP is a type of autoimmune condition (which means your immune system is acting against your body rather than for it). ITP in adults is more common in women than men. It is very different from ITP in children, who usually get ITP after a viral infection but who recover without any treatment. ITP in adults normally needs treatment. Some people with ITP have other autoimmune conditions, such as rheumatoid arthritis, or infections such as hepatitis or HIV. If you have any of these medical issues, your ITP may be treated slightly differently. 1 of 8 ITP (August 2021) A normal platelet count is between 150 and 400 thousand million platelets per litre of blood. -

Isolated Plantar Vein Thrombosis Resembling a Corn with a Bruise
JE Hahm, et al pISSN 1013-9087ㆍeISSN 2005-3894 Ann Dermatol Vol. 31, No. 1, 2019 https://doi.org/10.5021/ad.2019.31.1.66 CASE REPORT Isolated Plantar Vein Thrombosis Resembling a Corn with a Bruise Ji Eun Hahm, Kang Su Kim, Jae Won Ha, Chul Woo Kim, Sang Seok Kim Department of Dermatology, Kangdong Sacred Heart Hospital, College of Medicine, Hallym University, Seoul, Korea Plantar vein thrombosis, rarely-reported disease, is usually or callus, plantar fibromatosis, or plantar verruca1. Among accompanied by pain and tenderness in the plantar region laborers, they may develop from excess pressure on the and should be differentiated from other dermatological con- bony prominences of the feet, repetitive uneven friction ditions causing plantar pain, such as hemorrhagic corn/cal- from footwear, or gait abnormalities. Plantar vein throm- lus, plantar epidermal cyst, verruca, or plantar fibromatosis. bosis is a rare condition causing plantar pain. The exact A 52-year-old man presented with a violaceous tender sub- cause of plantar vein thrombosis is yet unclear, but predis- cutaneous nodule overlying a hyperkeratotic plaque on his posing conditions, such as prior trauma, surgery, paraneo- sole. Initially, he thought it was a corn and applied keratolytic plastic syndromes, or coagulation disorders have been agents, which failed to work. Sonography revealed a well-de- described. To date, there is no established treatment ex- marcated mass with increased peripheral vascularity. His cept surgical excision, but reportedly, nonsteroidal anti-in- pain was relieved after a complete wide excision, which con- flammatory drug or heparin with elastic bandage is known firmed the mass to be plantar vein thrombosis after histo- to be effective for symptomatic control2-5. -

Understanding Haemophilia
Understanding haemophilia Understanding haemophilia Contents Introduction 3 Haemophilia and your child 4 What is haemophilia? 5 What causes haemophilia? 5 Can females have haemophilia? 6 Carriers 8 Who is affected by haemophilia? 9 How severe is haemophilia? 9 Signs and symptoms of haemophilia 11 How is haemophilia diagnosed? 14 Diagnosis 14 Treatment 16 Port-a-cath 19 Managing joint bleeds with PRICE 19 Gene therapy 21 Possible complications of haemophilia 22 Inhibitors 22 Joint damage 22 Medical and dental treatment 23 Surgery Circumcision Dental care Medicines Vaccinations Bleeding disorder card Living with haemophilia 26 Sport and exercise 27 School, college and work 28 Travel 29 Pregnancy and haemophilia 30 Glossary of terms 32 About The Haemophilia Society 33 2 Understanding haemophilia Introduction This booklet is about haemophilia A and B. It gives a general overview of haemophilia and information on diagnosing, treating and living with the condition that we hope will answer your main questions. It has been written for people directly affected by haemophilia and for anyone interested in learning about haemophilia. If you are a parent and your child has recently been diagnosed with haemophilia you may be feeling quite overwhelmed. Remember, you’re not alone and many families are facing the same concerns and issues. Please do get in touch – we have lots of support and information available as well as services for parents and children. You can find out more via our website or Facebook pages, by emailing [email protected] or calling us on 020 7939 0780. The outlook is now the best it has ever been for people with haemophilia in the UK. -

EFFIENT Safely and Effectively
1 HIGHLIGHTS OF PRESCRIBING INFORMATION • Patients with unstable angina or, non-ST-elevation myocardial These highlights do not include all the information needed to use infarction (NSTEMI) (1.1). EFFIENT safely and effectively. See full prescribing information • Patients with ST-elevation myocardial infarction (STEMI) when for EFFIENT. managed with either primary or delayed PCI (1.1). EFFIENT (prasugrel) tablets, for oral use ------------------------ DOSAGE AND ADMINISTRATION ----------------------- Initial U.S. Approval: 2009 • Initiate treatment with a single 60-mg oral loading dose (2). • Continue at 10-mg once daily with or without food. Consider 5-mg WARNING: BLEEDING RISK once daily for patients <60 kg (2). See full prescribing information for complete boxed warning. • Patients should also take aspirin (75-mg to 325-mg) daily (2). • Effient can cause significant, sometimes fatal, bleeding (5.1, ---------------------- DOSAGE FORMS AND STRENGTHS --------------------- 5.2, 6.1). • Do not use Effient in patients with active pathological bleeding 5-mg and 10-mg tablets (3) or a history of transient ischemic attack or stroke (4.1, 4.2). ------------------------------- CONTRAINDICATIONS ------------------------------ • In patients ≥75 years of age, Effient is generally not • Active pathological bleeding (4.1) recommended, except in high-risk patients (diabetes or prior • Prior transient ischemic attack or stroke (4.2) MI), where its use may be considered (8.5). • Hypersensitivity to prasugrel or any component of the product • Do not start Effient in patients likely to undergo urgent (4.3) coronary artery bypass graft surgery (CABG). When possible, discontinue Effient at least 7 days prior to any surgery (5.2). ------------------------ WARNINGS AND PRECAUTIONS ----------------------- • Additional risk factors for bleeding include: body weight • CABG-related bleeding: Risk increases in patients receiving <60 kg; propensity to bleed; concomitant use of medications Effient who undergo CABG (5.2). -

Approach to Bleeding Diathesi
Approach to Bleeding Diathesis Dr.Nalini K Pati MD, DNB, DCH (Syd), FRCPA Paediatric Haematologist Royal Children’s Hospital Melbourne Australia Objectives Objectives - I I. Clinical aspects of bleeding Clinical aspects of bleeding II. Hematologic disorders causing bleeding • Coagulation factor disorders • Platelet disorders III. Approach to acquired bleeding disorders • Hemostasis in liver disease • Surgical patients • Warfarin toxicity IV. Approach to laboratory abnormalities • Diagnosis and management of thrombocytopenia V. Drugs and blood products used for bleeding Clinical Features of Bleeding Disorders Petechiae Platelet Coagulation (typical of platelet disorders) disorders factor disorders Site of bleeding Skin Deep in soft tissues Mucous membranes (joints, muscles) (epistaxis, gum, vaginal, GI tract) Petechiae Yes No Ecchymoses (“bruises”) Small, superficial Large, deep Hemarthrosis / muscle bleeding Extremely rare Common Do not blanch with pressure Bleeding after cuts & scratches Yes No (cf. angiomas) Bleeding after surgery or trauma Immediate, Delayed (1-2 days), usually mild often severe Not palpable (cf. vasculitis) Ecchymoses (typical of coagulation factor disorders) Objectives - II Hematologic disorders causing bleeding – Coagulation factor disorders – Platelet disorders Coagulation factor disorders Hemophilia A and B Inherited bleeding Acquired bleeding Hemophilia A Hemophilia B disorders disorders Coagulation factor deficiency Factor VIII Factor IX – Hemophilia A and B – Liver disease – vonWillebrands disease – Vitamin K Inheritance X-linked X-linked recessive recessive – Other factor deficiencies deficiency/warfarin overdose Incidence 1/10,000 males 1/50,000 males –DIC Severity Related to factor level <1% - Severe - spontaneous bleeding 1-5% - Moderate - bleeding with mild injury 5-25% - Mild - bleeding with surgery or trauma Complications Soft tissue bleeding Hemarthrosis (acute) Hemophilia Clinical manifestations (hemophilia A & B are indistinguishable) Hemarthrosis (most common) Fixed joints Soft tissue hematomas (e. -

Blood Clot 13 .Indd
MECHANICAL DEVICES PLEASE NOTE: GRADUATED COMPRESSION STOCKINGS (GCS) How long should I keep using the anticoagu- lant drug? These are tight stockings that squeeze your lower legs. They help keep the blood fl owing through the What should I do if I can’t give myself the shot? veins in your legs. Your legs will be measured to If you have any questions about the drugs used REDUCING fi t the stockings properly. Wear them all the time, to prevent a clot, please ask your doctor, nurse except when washing or showering until you re- or pharmacist. Your Risk of turn to your normal level of daily activity. Let your If you were given graduated compression doctor or nurse know if your skin changes color or BLOOD CLOTS stockings, they should be worn until you return if you develop blisters or pain from the stockings. to your usual level of activity. OR VTES And make sure the stockings don’t roll down to the space behind your kneecap. If you develop any symptoms of possible Deep Vein Thrombosis or Pulmonary Embolus at SEQUENTIAL COMPRESSION DEVICES (SCD) home in the days and weeks after hospitaliza- These are infl atable sleeves that are placed on tion, then seek medical advice immediately, your legs. They will squeeze your legs on and off either from your doctor or your nearest hospital during the day. Take them off before you get out of emergency department. bed because they can cause you to trip and fall. Reproduced with permission from Hotel-Dieu Be sure to ask for the sleeves to be put back on. -

Deep Vein Thrombosis (DVT)
Diseases and Conditions Deep vein thrombosis (DVT) By Mayo Clinic Staff Deep vein thrombosis (DVT) occurs when a blood clot (thrombus) forms in one or more of the deep veins in your body, usually in your legs. Deep vein thrombosis can cause leg pain or swelling, but may occur without any symptoms. Deep vein thrombosis can develop if you have certain medical conditions that affect how your blood clots. Deep vein thrombosis can also happen if you don't move for a long time, such as after surgery, following an accident, or when you are confined to a hospital or nursing home bed. Deep vein thrombosis is a serious condition because blood clots in your veins can break loose, travel through your bloodstream and lodge in your lungs, blocking blood flow (pulmonary embolism). Deep vein thrombosis signs and symptoms can include: Swelling in the affected leg. Rarely, there may be swelling in both legs. Pain in your leg. The pain often starts in your calf and can feel like cramping or a soreness. Deep vein thrombosis may sometimes occur without any noticeable symptoms. When to see a doctor If you develop signs or symptoms of deep vein thrombosis, contact your doctor for guidance. If you develop signs or symptoms of a pulmonary embolism — a life-threatening complication of deep vein thrombosis — seek medical attention immediately. The warning signs of a pulmonary embolism include: Unexplained sudden onset of shortness of breath Chest pain or discomfort that worsens when you take a deep breath or when you cough Feeling lightheaded or dizzy, or fainting Rapid pulse Coughing up blood Deep vein thrombosis occurs when a blood clot forms in the veins that are deep in your body, often in your legs. -

An Approach to Investigation of Easy Bruising
488 Arch Dis Child 2001;84:488–491 PERSONAL PRACTICE Arch Dis Child: first published as 10.1136/adc.84.6.488 on 1 June 2001. Downloaded from An approach to investigation of easy bruising A Vora, M Makris Easy bruising presents several investigative its absence excludes significant abnormality. dilemmas in primary and secondary practice, Steroid inhaler or non-steroidal anti- not least because it raises the spectre of physi- inflammatory drug (NSAID) use, current or cal abuse. When, and to what extent, should previous, should be excluded in those cases general paediatricians investigate before refer- where an abnormal pattern of bruising is the ral to a specialist? When can it be safely sole cause for concern. Long term use of high concluded that an underlying bleeding disor- dose inhaled steroids, and even a single dose of der has been excluded, so that further investi- NSAIDs, can predispose to easy bruising that gations can focus on ruling out suspected non- persists for weeks to months after cessation. accidental injury? When, despite an abnormal Other drugs, such as anticonvulsants, may also clotting test, should the latter investigations be a cause of easy bruising and a comprehen- still be pursued? sive drug history should be an important part The intention of this review is to attempt to of the initial assessment. answer these questions from the perspective of The target of further investigation should routine practice without recourse to a compre- therefore be patients with bruising over the hensive review of bleeding disorders or non- trunk, neck, or face, irrespective of limb or accidental injury. -

Gunmen Free Two Hostages
W - MANCHESTER HERALD, Friday. June 20, 1986 SPORTS WEEKEND PLUS About Town Orioles blow out WVIT’s Crispino Cedars set potiuck additional fees for materials. Also for preschool children, will board of governors of the Univer cruise, Noank. Bus leaves at 10; 15 leaves Cheney Hall at 7:30 a.m. The student season will open be Lunch at Lutz from July 1 to 3 sity of Michigan Club of Hartford a.m. Nov. 21 — Culinary Institute and Tall Cedars, Nutmeg Forest 116, with two classes running from from 11 a.m. to 12:30 p.m. Oiildren at the recent annual meeting. Both Aug. 12 — Statue of Liberty. New Roosevelt mansion, Hyde Fark, first-place Bosox on his T V career will have its annual potiuck with July 1 to 3. They are a robot will bring a lunch, hear stories and received bachelor’s and master's York City. Bus leaves at 7;30 a.m. N.Y. Dec. 4 to 5 — Christmastime in strawberry shortcake on Monday . creation class for children who play games. The cost wilt be $15 for degrees at the university. Sept. 9 — Housatonlc railroad page 9 ... magazine Inside at 6 p.m. at the Masonic Temple, 25 have just completed Grades 2 to 4 members and $18 for non tour, Canaan Union Depot to the Brandywine Valley at the E. Center St. Bernie Bentley will and a nature exlorer class for members. AARP plans trips Cornwall. Bus leaves at 8 a.m. Pennsylvania-Delaware border. play his banjo. The event is open to children who have just completed For more information on these Sept. -

Contraindications for Massage Therapy
Contraindications for Massage Therapy Contraindications are certain conditions that a person may have that could be aggravated by the application of Massage Therapy. Although certain conditions may be absolute contraindications, there may be cases where massage can be applied, provided a doctor’s approval has been attained and the massage treatment has been adjusted. Often Cautions are included under contraindications. In these cases, the type of massage may need to be adjusted, certain parts may best be avoided or special client care may be attended to. Quite often in these cases specific massage techniques may assist the client with the condition. A Doctor’s approval is not necessarily required for conditions listed as ‘cautions’. -Abnormal body temperature A normal body temperature is 37 Degrees Celsius (+ or – 0.6) If a client has a fever, massage could increase it. A fever may be caused by vaccinations or early signs of the flu -Acute Inflammatory Conditions (rheumatoid arthritis, bursitis, tendonitis) The signs of inflammation are redness, heat, pain, swelling and reduced function. The area that is inflamed will only be made worse with massage because more blood will travel to the area. Rheumatoid Arthritis: If joints are actively inflamed they need to be avoided. However if the condition is chronic, massage can be of assistance Tendonitis: Avoid in the acute stages Bursitis: Avoid totally Injuries (sprains, strains, broken bones): At least 48 hours after injury Bacterial Infections: Can often present with pustules-needs to be avoided as can lead to systemic infection -Acute Infectious Conditions Massage will only intensify the illness. Examples include Hepatitis A, food poisoning, influenza, immunisation. -
System Specific Trauma
MODULE 3 System Specific Trauma | Emergency and Essential Surgical Care (EESC) programme 1 www.who.int/surgery OBJECTIVES FOR MODULE 3 To learn specific management strategies for trauma • Head • Spine and spinal cord • Chest • Abdomen • Female genitalia • Musculoskeletal system | Emergency and Essential Surgical Care (EESC) programme 2 www.who.int/surgery Head Injury | Emergency and Essential Surgical Care (EESC) programme 3 www.who.int/surgery HEAD INJURY • Altered level of consciousness is a hallmark of acute cerebral trauma • Never assume that substances (alcohol or drugs) are causes of drowsiness • Frequent clinical mistakes: – Incomplete ABC's, priority management – Incomplete primary, secondary surveys – Incomplete baseline neurologic examination – No reassessment of neurologic status | Emergency and Essential Surgical Care (EESC) programme 4 www.who.int/surgery HEAD INJURY Basal skull fractures – Periorbital ecchymosis (racoon eyes) – Mastoid ecchymosis (Battle's sign) – Cerebrospinal fluid leak from ears or nose Depressed skull fracture – Fragments of skull may penetrate dura, brain Cerebral concussion – Variable temporary altered consciousness | Emergency and Essential Surgical Care (EESC) programme 5 www.who.int/surgery HEAD INJURY Intracerebral hematoma – Caused by acute injury or delayed, progressive bleeding originating from contusion Clinical features of increased intracranial pressure: – Decreased level of consciousness – Bradycardia – Unequal or dilated pupils – Seizures – Focal neurologic deficit | Emergency and Essential