A 1.35 Mb DNA Fragment Is Inserted Into the DHMN1 Locus on Chromosome 7Q34–Q36.2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Preclinical Research 2020 Sections
Sackler Faculty of Medicine Preclinical Research 2020 Sections Cancer and Molecular Therapies 8 Dental Health and Medicine 52 Diabetes, Metabolic and Endocrine Diseases 62 Genomics & Personalized Medicine 78 Hearing, Language & Speech Sciences and Disorders 98 Infectious Diseases 117 Inflammatory and Autoimmune Diseases 137 Medical Education and Ethics 147 Nervous System and Brain Disorders 154 Nursing, Occupational and Physical Therapy 200 Public Health 235 Reproduction, Development and Evolution 263 Stem Cells and Regenerative Medicine 280 Cover images (from bottom left, clockwise): Image 1: Human embryonic stem cell derived cardiomyocytes stained with fluorescent antibodies. The cardiac marker alpha-actinin (green), calcium channel modulator, Ahnak1 (red) – Shimrit Oz, Nathan Dascal. Image 2: Islet of Langerhans containing insulin-producing beta-cells (green) and glucagon- producing alpha-cells (red) – Daria Baer, Limor Landsman. Image 3: β-catenin in C. elegans vulva – Michal Caspi, Limor Broday, Rina Rosin-Arbesfeld. Image 4: Stereocilia of a sensory outer hair cell from a mouse inner ear – Shaked Shivatzki, Karen Avraham. Image 5: Electron scanning micrograph of middle ear ossicles from a mouse ear stained with pseudo colors – Shaked Shivatski, Karen Avraham. Image 6: Resistin-like molecule alpha (red), eosinophil major basic protein (green) and DAPI (blue) staining of asthmatic mice – Danielle Karo-Atar, Ariel Munitz. © All rights reserved Editor: Prof. Karen Avraham Graphic design: Michal Semo Kovetz, TAU Graphic Design Studio February 2020 Sackler Faculty of Medicine Research 2020 2 The Sackler Faculty of Medicine The Sackler Faculty of Medicine is Israel’s largest diabetes, neurodegenerative diseases, infectious medical research and training complex. The Sackler diseases and genetic diseases, including but not Faculty of Medicine of Tel Aviv University (TAU) was imited to Alzheimer’s disease, Parkinson’s disease founded in 1964 following the generous contributions and HIV/AIDS. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -

Gene Expression Analysis Reveals Novel Gene Signatures Between Young and Old Adults in Human Prefrontal Cortex
fnagi-10-00259 August 24, 2018 Time: 10:32 # 1 ORIGINAL RESEARCH published: 27 August 2018 doi: 10.3389/fnagi.2018.00259 Gene Expression Analysis Reveals Novel Gene Signatures Between Young and Old Adults in Human Prefrontal Cortex Yang Hu1,2,3, Junping Pan1, Yirong Xin1, Xiangnan Mi1, Jiahui Wang1, Qin Gao1 and Huanmin Luo1,3* 1 Department of Pharmacology, School of Medicine, Jinan University, Guangzhou, China, 2 Department of Pathology and Pathophysiology, School of Medicine, Jinan University, Guangzhou, China, 3 Institute of Brain Sciences, Jinan University, Guangzhou, China Human neurons function over an entire lifetime, yet the molecular mechanisms which perform their functions and protecting against neurodegenerative disease during aging are still elusive. Here, we conducted a systematic study on the human brain aging by using the weighted gene correlation network analysis (WGCNA) method to identify meaningful modules or representative biomarkers for human brain aging. Significantly, 19 distinct gene modules were detected based on the dataset GSE53890; among them, six modules related to the feature of brain aging were highly preserved in diverse independent datasets. Interestingly, network feature analysis confirmed that the blue modules demonstrated a remarkably correlation with human brain aging progress. Edited by: Panteleimon Giannakopoulos, Besides, the top hub genes including PPP3CB, CAMSAP1, ACTR3B, and GNG3 Université de Genève, Switzerland were identified and characterized by high connectivity, module membership, or gene Reviewed by: significance in the blue module. Furthermore, these genes were validated in mice of Suowen Xu, different ages. Mechanically, the potential regulators of blue module were investigated. University of Rochester, United States Maciej J. Lazarczyk, These findings highlight an important role of the blue module and its affiliated genes in Geneva University Hospitals (HUG), the control of normal brain aging, which may lead to potential therapeutic interventions Switzerland for brain aging by targeting the hub genes. -

Cytotoxicity and Genome-Wide Microarray Analysis of Intestinal Smooth Muscle Cells in Response to Hexavalent Chromium Induction
Zoological Research 34 (E3): E93−E100 DOI:10.11813/j.issn.0254-5853.2013.E3.E93 Cytotoxicity and genome-wide microarray analysis of intestinal smooth muscle cells in response to hexavalent chromium induction Li-Fang JIN, Yuan-Yuan WANG, Zi-Dong ZHANG, Yi-Meng YUAN, Yi-Rui HU, Yang-Feng WEI, * Jian NI College of Life Science of Shaoxing University, Shaoxing Zhejiang 312000, China Abstract: Chronic ingestion of high concentrations of hexavalent chromium [Cr(VI)] in drinking water induces intestinal tumors in mice; however, information on its toxicity on intestinal smooth muscle cells is limited. The present study aimed to assess the in vitro and in vivo toxicological effects of Cr(VI) on intestinal smooth muscle cells. Human intestinal smooth muscle cells (HISM cells) were cultured with different concentrations of Cr(VI) to evaluate effects on cell proliferation ability, oxidative stress levels, and antioxidant system. Furthermore, tissue sections in Cr(VI) exposed rabbits were analyzed to evaluate toxicity on intestinal muscle cells in vivo. Gene chips were utilized to assess differential gene expression profiles at the genome-wide level in 1 μmol/L Cr(VI) treated cells. Intestinal tissue biopsy results showed that Cr(VI) increased the incidences of diffuse epithelial hyperplasia in intestinal jejunum but caused no obvious damage to the structure of the muscularis. Cell proliferation analysis revealed that high concentrations (≥64 μmol/L) but not low concentrations of Cr(VI) (≤16 μmol/L) significantly inhibited the growth of HISM cells. For oxidative stress levels, the expression of reactive oxygen species (ROS) and nitric oxide (NO) was elevated at high concentrations (≥64 μmol/L) but not at low concentrations of Cr(VI) (≤16 μmol/L). -

Whole Exome Sequencing in Families at High Risk for Hodgkin Lymphoma: Identification of a Predisposing Mutation in the KDR Gene
Hodgkin Lymphoma SUPPLEMENTARY APPENDIX Whole exome sequencing in families at high risk for Hodgkin lymphoma: identification of a predisposing mutation in the KDR gene Melissa Rotunno, 1 Mary L. McMaster, 1 Joseph Boland, 2 Sara Bass, 2 Xijun Zhang, 2 Laurie Burdett, 2 Belynda Hicks, 2 Sarangan Ravichandran, 3 Brian T. Luke, 3 Meredith Yeager, 2 Laura Fontaine, 4 Paula L. Hyland, 1 Alisa M. Goldstein, 1 NCI DCEG Cancer Sequencing Working Group, NCI DCEG Cancer Genomics Research Laboratory, Stephen J. Chanock, 5 Neil E. Caporaso, 1 Margaret A. Tucker, 6 and Lynn R. Goldin 1 1Genetic Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 2Cancer Genomics Research Laboratory, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 3Ad - vanced Biomedical Computing Center, Leidos Biomedical Research Inc.; Frederick National Laboratory for Cancer Research, Frederick, MD; 4Westat, Inc., Rockville MD; 5Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; and 6Human Genetics Program, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD, USA ©2016 Ferrata Storti Foundation. This is an open-access paper. doi:10.3324/haematol.2015.135475 Received: August 19, 2015. Accepted: January 7, 2016. Pre-published: June 13, 2016. Correspondence: [email protected] Supplemental Author Information: NCI DCEG Cancer Sequencing Working Group: Mark H. Greene, Allan Hildesheim, Nan Hu, Maria Theresa Landi, Jennifer Loud, Phuong Mai, Lisa Mirabello, Lindsay Morton, Dilys Parry, Anand Pathak, Douglas R. Stewart, Philip R. Taylor, Geoffrey S. Tobias, Xiaohong R. Yang, Guoqin Yu NCI DCEG Cancer Genomics Research Laboratory: Salma Chowdhury, Michael Cullen, Casey Dagnall, Herbert Higson, Amy A. -

Deep Multiomics Profiling of Brain Tumors Identifies Signaling Networks
ARTICLE https://doi.org/10.1038/s41467-019-11661-4 OPEN Deep multiomics profiling of brain tumors identifies signaling networks downstream of cancer driver genes Hong Wang 1,2,3, Alexander K. Diaz3,4, Timothy I. Shaw2,5, Yuxin Li1,2,4, Mingming Niu1,4, Ji-Hoon Cho2, Barbara S. Paugh4, Yang Zhang6, Jeffrey Sifford1,4, Bing Bai1,4,10, Zhiping Wu1,4, Haiyan Tan2, Suiping Zhou2, Laura D. Hover4, Heather S. Tillman 7, Abbas Shirinifard8, Suresh Thiagarajan9, Andras Sablauer 8, Vishwajeeth Pagala2, Anthony A. High2, Xusheng Wang 2, Chunliang Li 6, Suzanne J. Baker4 & Junmin Peng 1,2,4 1234567890():,; High throughput omics approaches provide an unprecedented opportunity for dissecting molecular mechanisms in cancer biology. Here we present deep profiling of whole proteome, phosphoproteome and transcriptome in two high-grade glioma (HGG) mouse models driven by mutated RTK oncogenes, PDGFRA and NTRK1, analyzing 13,860 proteins and 30,431 phosphosites by mass spectrometry. Systems biology approaches identify numerous master regulators, including 41 kinases and 23 transcription factors. Pathway activity computation and mouse survival indicate the NTRK1 mutation induces a higher activation of AKT down- stream targets including MYC and JUN, drives a positive feedback loop to up-regulate multiple other RTKs, and confers higher oncogenic potency than the PDGFRA mutation. A mini-gRNA library CRISPR-Cas9 validation screening shows 56% of tested master regulators are important for the viability of NTRK-driven HGG cells, including TFs (Myc and Jun) and metabolic kinases (AMPKa1 and AMPKa2), confirming the validity of the multiomics inte- grative approaches, and providing novel tumor vulnerabilities. -
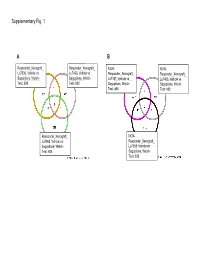
Supplementary Data
Supplementary Fig. 1 A B Responder_Xenograft_ Responder_Xenograft_ NON- NON- Lu7336, Vehicle vs Lu7466, Vehicle vs Responder_Xenograft_ Responder_Xenograft_ Sagopilone, Welch- Sagopilone, Welch- Lu7187, Vehicle vs Lu7406, Vehicle vs Test: 638 Test: 600 Sagopilone, Welch- Sagopilone, Welch- Test: 468 Test: 482 Responder_Xenograft_ NON- Lu7860, Vehicle vs Responder_Xenograft_ Sagopilone, Welch - Lu7558, Vehicle vs Test: 605 Sagopilone, Welch- Test: 333 Supplementary Fig. 2 Supplementary Fig. 3 Supplementary Figure S1. Venn diagrams comparing probe sets regulated by Sagopilone treatment (10mg/kg for 24h) between individual models (Welsh Test ellipse p-value<0.001 or 5-fold change). A Sagopilone responder models, B Sagopilone non-responder models. Supplementary Figure S2. Pathway analysis of genes regulated by Sagopilone treatment in responder xenograft models 24h after Sagopilone treatment by GeneGo Metacore; the most significant pathway map representing cell cycle/spindle assembly and chromosome separation is shown, genes upregulated by Sagopilone treatment are marked with red thermometers. Supplementary Figure S3. GeneGo Metacore pathway analysis of genes differentially expressed between Sagopilone Responder and Non-Responder models displaying –log(p-Values) of most significant pathway maps. Supplementary Tables Supplementary Table 1. Response and activity in 22 non-small-cell lung cancer (NSCLC) xenograft models after treatment with Sagopilone and other cytotoxic agents commonly used in the management of NSCLC Tumor Model Response type -

Mccartney, Karen M. (2015)
THE ROLE OF PEROXISOME PROLIFERATOR ACTIVATED RECEPTOR ALPHA (PPARα) IN THE EFFECT OF PIROXICAM ON COLON CANCER KAREN MARIE McCARTNEY BSc. (Hons), MSc. Thesis submitted to the University of Nottingham for the degree of Doctor of Philosophy April 2015 Abstract Studies with APCMin/+ mice and APCMin/+ PPARα-/- mice were undertaken to investigate whether polyp development in the mouse gut was mediated by PPARα. Additionally, the effect of piroxicam treatment dependency on PPARα was assessed. Results showed the number of polyps in the colon was significantly higher in APCMin/+ PPARα-/- mice than in APCMin/+ mice, whilst in the small bowel the difference was not significant. Analysis of gene expression in the colon with Affymetrix® microarrays demonstrated the largest source of variation was between tumour and normal tissue. Deletion of PPARα had little effect on gene expression in normal tissue but appeared to have more effect in tumour tissue. Ingenuity pathway analysis of these data showed the top biological processes were growth & proliferation and colorectal cancer. Collectively, these data may indicate that deletion of PPARα exacerbates the existing APCMin/+ mutation to promote tumorigenesis in the colon. 95 genes from Affymetrix® microarray data were selected for further analysis on Taqman® low density arrays. There was good correlation of expression levels between the two array types. Expression data of two genes proved particularly interesting; Onecut homeobox 2 (Onecut2) and Apolipoprotein B DNA dC dU - editing enzyme, catalytic polypeptide 3 (Apobec3). Onecut2 was highly up-regulated in tumour tissue. Apobec3 was up-regulated in APCMin/+ PPARα-/- mice only; suggesting expression was mediated via PPARα. There was a striking increase in survival accompanied by a marked reduction in small intestinal polyp numbers in mice of either genotype that received piroxicam. -

Mechanisms Underlying Phenotypic Heterogeneity in Simplex Autism Spectrum Disorders
Mechanisms Underlying Phenotypic Heterogeneity in Simplex Autism Spectrum Disorders Andrew H. Chiang Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy under the Executive Committee of the Graduate School of Arts and Sciences COLUMBIA UNIVERSITY 2021 © 2021 Andrew H. Chiang All Rights Reserved Abstract Mechanisms Underlying Phenotypic Heterogeneity in Simplex Autism Spectrum Disorders Andrew H. Chiang Autism spectrum disorders (ASD) are a group of related neurodevelopmental diseases displaying significant genetic and phenotypic heterogeneity. Despite recent progress in ASD genetics, the nature of phenotypic heterogeneity across probands is not well understood. Notably, likely gene- disrupting (LGD) de novo mutations affecting the same gene often result in substantially different ASD phenotypes. We find that truncating mutations in a gene can result in a range of relatively mild decreases (15-30%) in gene expression due to nonsense-mediated decay (NMD), and show that more severe autism phenotypes are associated with greater decreases in expression. We also find that each gene with recurrent ASD mutations can be described by a parameter, phenotype dosage sensitivity (PDS), which characteriZes the relationship between changes in a gene’s dosage and changes in a given phenotype. Using simple linear models, we show that changes in gene dosage account for a substantial fraction of phenotypic variability in ASD. We further observe that LGD mutations affecting the same exon frequently lead to strikingly similar phenotypes in unrelated ASD probands. These patterns are observed for two independent proband cohorts and multiple important ASD-associated phenotypes. The observed phenotypic similarities are likely mediated by similar changes in gene dosage and similar perturbations to the relative expression of splicing isoforms. -

Population Genomics in a Disease Targeted Primary Cell Model
Downloaded from genome.cshlp.org on October 8, 2021 - Published by Cold Spring Harbor Laboratory Press Letter Population genomics in a disease targeted primary cell model Elin Grundberg,1,2,12 Tony Kwan,1,2,12 Bing Ge,2 Kevin C.L. Lam,2 Vonda Koka,2 Andreas Kindmark,3 Hans Mallmin,4 Joana Dias,2 Dominique J. Verlaan,1,2,5 Manon Ouimet,5 Daniel Sinnett,5,6 Fernando Rivadeneira,7,8 Karol Estrada,7 Albert Hofman,8 Joyce M. van Meurs,7 Andre´ Uitterlinden,7,8 Patrick Beaulieu,5 Alexandru Graziani,5 Eef Harmsen,2 O¨ sten Ljunggren,3 Claes Ohlsson,9 Dan Mellstro¨m,9 Magnus K. Karlsson,10 Olle Nilsson,4 and Tomi Pastinen1,2,11,13 1Department of Human Genetics, McGill University, Montre´al H3A 1B1, Canada; 2McGill University and Genome Que´bec Innovation Centre, Montre´al H3A 1A4, Canada; 3Department of Medical Sciences, Uppsala University, Uppsala 75185, Sweden; 4Department of Surgical Sciences, Uppsala University, Uppsala 75185, Sweden; 5Sainte-Justine University Health Center, Montre´al H3T 1C5, Canada; 6Department of Pediatrics, University of Montre´al, Montre´al H3T 1C5, Canada; 7Department of Internal Medicine, Erasmus MC, Rotterdam 3015GE, The Netherlands; 8Department of Epidemiology, Erasmus MC, Rotterdam 3015GE, The Netherlands; 9Center for Bone Research at the Sahlgrenska Academy, Department of Internal Medicine, Go¨teborg University, Gothenburg 41345, Sweden; 10Clinical and Molecular Osteoporosis Research Unit, Department of Clinical Science, Lund University and Department of Orthopaedics, Malmo¨University Hospital, Malmo¨20502, Sweden; 11Department of Medical Genetics, McGill University, Montre´al H3H 1P3, Canada The common genetic variants associated with complex traits typically lie in noncoding DNA and may alter gene regu- lation in a cell type-specific manner. -

Molecular Correlates of Metastasis by Systematic Pan-Cancer Analysis Across the Cancer Genome Atlas
Author Manuscript Published OnlineFirst on November 6, 2018; DOI: 10.1158/1541-7786.MCR-18-0601 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Molecular correlates of metastasis by systematic pan-cancer analysis across The Cancer Genome Atlas Fengju Chen1*, Yiqun Zhang1*, Sooryanarayana Varambally2,3, Chad J. Creighton1,4,5,6 1. Dan L. Duncan Comprehensive Cancer Center Division of Biostatistics, Baylor College of Medicine, Houston, TX, USA. 2. Comprehensive Cancer Center, University of Alabama at Birmingham, Birmingham, AL 35233, USA 3. Molecular and Cellular Pathology, Department of Pathology, University of Alabama at Birmingham, Birmingham, AL 35233, USA 4. Department of Bioinformatics and Computational Biology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA 5. Human Genome Sequencing Center, Baylor College of Medicine, Houston, TX 77030, USA 6. Department of Medicine, Baylor College of Medicine, Houston, TX, USA * co-first authors Running title: Pan-cancer metastasis correlates Abbreviations: TCGA, The Cancer Genome Atlas; RNA-seq, RNA sequencing; RPPA, reverse- phase protein arrays Correspondence to: Chad J. Creighton ([email protected]) One Baylor Plaza, MS305 Houston, TX 77030 Disclosure of potential conflicts of interest: The authors have no conflicts of interest. 1 Downloaded from mcr.aacrjournals.org on September 28, 2021. © 2018 American Association for Cancer Research. Author Manuscript Published OnlineFirst on November 6, 2018; DOI: 10.1158/1541-7786.MCR-18-0601 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Abstract Tumor metastasis is a major contributor to cancer patient mortality, but the process remains poorly understood. -

UBE3B Is a Mitochondria-Associated E3 Ubiquitin Ligase Whose Activity Is Modulated by Its Interaction with Calmodulin to Respond to Oxidative Stress
UBE3B is a mitochondria-associated E3 ubiquitin ligase whose activity is modulated by its interaction with Calmodulin to respond to oxidative stress by Andrea Catherine Braganza B.S. Biotechnology, Rochester Institute of Technology, 2008 Submitted to the Graduate Faculty of University of Pittsburgh School of Medicine in partial fulfillment of the requirements for the degree of Doctor of Philosophy University of Pittsburgh 2015 UNIVERSITY OF PITTSBURGH SCHOOL OF MEDICINE-MOLECULAR PHARMACOLOGY This dissertation was presented by Andrea Catherine Braganza It was defended on August 21st, 2015 and approved by Chairperson: Sruti Shiva, Ph.D., Associate Professor, Department of Pharmacology and Chemical Biology Bruce Freeman, Ph.D., Professor and Chair, Department of Pharmacology and Chemical Biology Jing Hu, M.D., Ph.D., Assistant Professor, Department of Pharmacology and Chemical Biology Jeffrey Brodsky, Ph.D., Professor, Department of Biological Sciences Sarah Berman, M.D., Ph.D., Assistant Professor, Department of Neurology Dissertation Advisor: Robert W. Sobol, Ph.D., Associate Professor, Department of Pharmacology and Chemical Biology ii Copyright © by Andrea Catherine Braganza 2015 iii UBE3B is a mitochondria-associated E3 ubiquitin ligase whose activity is modulated by its interaction with Calmodulin to respond to oxidative stress Andrea Catherine Braganza, Ph.D. University of Pittsburgh, 2015 Recent genome-wide studies found that patients with hypotonia, developmental delay, intellectual disability, congenital anomalies, characteristic facial dysmorphic features, and low cholesterol levels suffer from Kaufman oculocerebrofacial syndrome (also reported as blepharophimosis-ptosis-intellectual disability syndrome). The primary cause of Kaufman oculocerebrofacial syndrome (KOS) is autosomal recessive mutations in the gene UBE3B. However, to date, there are no studies that determine the cellular or enzymatic function of UBE3B.