Meningitis, Encephalitis and Neonatal Sepsis 1 GBD 2017 1 WHO
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
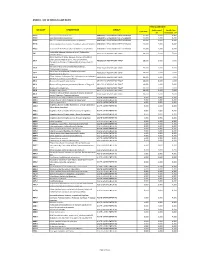
Annex 1: List of Medical Case Rates
ANNEX 1. LIST OF MEDICAL CASE RATES FIRST CASE RATE ICD CODE DESCRIPTION GROUP Professional Health Care Case Rate Fee Institution Fee P91.3 Neonatal cerebral irritability ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.4 Neonatal cerebral depression ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.6 Hypoxic ischemic encephalopathy of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.8 Other specified disturbances of cerebral status of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.9 Disturbance of cerebral status of newborn, unspecified ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 Peritonsillar abscess; Abscess of tonsil; Peritonsillar J36 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 cellulitis; Quinsy Other diseases of larynx; Abscess of larynx; Cellulitis of larynx; Disease NOS of larynx; Necrosis of larynx; J38.7 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Pachyderma of larynx; Perichondritis of larynx; Ulcer of larynx Retropharyngeal and parapharyngeal abscess; J39.0 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Peripharyngeal abscess Other abscess of pharynx; Cellulitis of pharynx; J39.1 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Nasopharyngeal abscess Other diseases of pharynx; Cyst of pharynx or nasopharynx; J39.2 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Oedema of pharynx or nasopharynx J85.1 Abscess of lung with pneumonia ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 J85.2 Abscess of lung without pneumonia; Abscess of lung NOS ABSCESS OF RESPIRATORY -

Supplementary Appendix
Supplementary appendix Sipilä PN, Heikkilä N, Lindbohm JV, Hakulinen C, Vahtera J, Elovainio M, Suominen S, Väänänen A, Koskinen A, Nyberg ST, Pentti J, Strandberg TE, Kivimäki M. Hospital-treated infectious diseases and the risk of incident dementia: multicohort study with replication in the UK Biobank CONTENTS eFigure 1. Selection of participants in the study............................................................................... 2 eMethods 1. Study cohorts and data collection ................................................................................ 3 The Finnish Public Sector study (FPS)......................................................................................... 3 The Health and Social Support study (HeSSup) ........................................................................... 4 The Still Working study (STW) ................................................................................................... 5 The UK Biobank ......................................................................................................................... 5 eMethods 2. Proportionality of hazards ........................................................................................... 7 eFigure 2. Visualisation of hazard ratios over time using exponentiated scaled Schoenfeld residuals ....................................................................................................................................................... 8 eFigure 3. Dementia follow-up ..................................................................................................... -

Ten Leading Causes of Death by Age Group,Race/Ethnicity, and Gender
Ten Leading Causes of Death by Age Group, Race/Ethnicity, and Gender Suburban Cook County 2006-2008 Suggested Citation: Cook County Department of Public Health. (2013). Ten Leading Causes of Death Tables 2008. Oak Forest, IL: Community Epidemiology and Health Planning Unit Table of Contents All Suburban Cook County: All Deaths By Gender: Females Males By Race/Ethnicity and Gender: Hispanic Hispanic Females Hispanic Males Non Hispanic Asian/Pacific Islander Non Hispanic Asian/Pacific Islander Females Non Hispanic Asian/Pacific Islander Males Non Hispanic Black Non Hispanic Black Females Non Hispanic Black Males Non Hispanic White Non Hispanic White Females Non Hispanic White Males By District: Cook County Department of Public Health Jurisdiction North District West District Southwest District South District Resources: District Map Rankable Causes of Death Rankable Causes of Infant Death 10 Leading Causes of Death by Age Group, Suburban Cook County, 2006-2008 (Counts/Percent of Total Deaths) All Deaths Rank <1 1-4 5-17 18-24 25-34 35-44 45-54 55-64 65+ Total Unintentional Unintentional Unintentional Unintentional Malignant Malignant Malignant Short Gestation Heart Disease Heart Disease 1 Injury Injury Injury Injury Neoplasms Neoplasms Neoplasms 170 24.9% 24 23.8% 57 24.6% 196 37.0% 281 34.4% 300 19.2% 1,251 31.7% 2,489 38.9% 13,422 28.2% 16,345 26.4% Congenital Congenital Unintentional Malignant Malignant Homicide Homicide Homicide Heart Disease Heart Disease 2 Anomalies Anomalies Injury Neoplasms Neoplasms 127 18.6% 9 8.9% 44 19.0% 135 -

Philippine Clinical Practice Guidelines on the Diagnosis And
Pediatric Infectious Diseases Society of the Philippines Journal Vol 16 No.2 pp 2-42 Jul-Dec 2015 PIDSP and CNSP Bacterial Meningitis TWG, Acute Bacterial Meningitis CPG 2015 PHILIPPINE CLINICAL PRACTICE GUIDELINES ON THE DIAGNOSIS AND MANAGEMENT OF ACUTE BACTERIAL MENINGITIS IN INFANTS AND CHILDREN Copyright 2015 A joint project of the Pediatric Infectious Disease Society of the Philippines (PIDSP) and Child Neurology Society of the Philippines (CNSP) 2 Pediatric Infectious Diseases Society of the Philippines Journal Vol 16 No.2 pp.2-42 Jul-Dec 2015 PIDSP and CNSP Bacterial Meningitis TWG, Acute Bacterial Meningitis CPG 2015 TABLE OF CONTENTS Page I. Introduction A. History of the guideline 5 B. Target users of the guideline 5 C. Forming the guideline 5 D. PIDSP/CNSP Steering Committee 6 E. Criteria for Assessment of Strength of Evidence and Recommendation 6 II. Recommendations A. Diagnosis of Acute Bacterial Meningitis 1. What are the signs and symptoms to suspect acute bacterial meningitis? 7 2. What is the definitive test for bacterial meningitis? 8 3. How do we differentiate acute bacterial meningitis from other CNS infections? 9 4. What are the contraindications to lumbar puncture? 9 5. What are the ancillary tests in the diagnosis of bacterial m eningitis? What is the value of each diagnostic test? a. Complete blo od count (CBC) 10 b. Blood culture 11 c. C-reactive protein (CRP) 11 d. Polymerase chain reaction (PCR) 13 e. Latex Agglutination Test (LAT) 13 f. Procalcitonin 14 6. What is the role of imaging tests in the diagnosis of bacterial meningitis? 15 B. -

Helping Mothers Defend Their Decision to Breastfeed
University of Central Florida STARS Electronic Theses and Dissertations, 2004-2019 2015 Helping Mothers Defend their Decision to Breastfeed Kandis Natoli University of Central Florida Part of the Nursing Commons Find similar works at: https://stars.library.ucf.edu/etd University of Central Florida Libraries http://library.ucf.edu This Doctoral Dissertation (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and Dissertations, 2004-2019 by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Natoli, Kandis, "Helping Mothers Defend their Decision to Breastfeed" (2015). Electronic Theses and Dissertations, 2004-2019. 1392. https://stars.library.ucf.edu/etd/1392 HELPING MOTHERS DEFEND THEIR DECISION TO BREASTFEED by KANDIS M. NATOLI M.S.N. University of Central Florida, 2006 B.S.N. University of Central Florida, 2005 A dissertation submitted in partial fulfillment of the requirements for the Degree of Doctor of Philosophy in Nursing in the College of Nursing at the University of Central Florida Orlando Florida Fall Term 2015 Major Professor: Karen Arioan © 2015 Kandis M. Natoli ii ABSTRACT The United States has established breastfeeding as an important health indicator within the Healthy People agenda. Healthy People target goals for breastfeeding initiation, duration, and exclusivity remain unmet. The US Surgeon General’s Office reports that lack of knowledge and widespread misinformation about breastfeeding are barriers to meeting Healthy People goals. Breastfeeding mothers are vulnerable to messages that cast doubt on their ability to breastfeed. Very little research has examined specific approaches to help people resist negative messages about health beliefs and behaviors. -

General Medical Microbiology and Infectious Disease BMS 6301
General Medical David L. Balkwill, Ph.D., Course Microbiology Director and Infectious Disease [email protected] BMS 6301 (850) 644-9219 2004 – 2005 Course Syllabus x Click here for the schedule Description: This course provides learning opportunities in the basic principles of medical microbiology and infectious disease. It covers mechanisms of infectious disease transmission, principles of aseptic practice, and the role of the human body’s normal microflora. The biology of bacterial, viral, fungal, and parasitic pathogens and the diseases they cause are covered. Relevant clinical examples are provided. The course provides the conceptual basis for understanding pathogenic microorganisms and the mechanisms by which they cause disease in the human body. It also provides opportunities to develop informatics and diagnostic skills, including the use and interpretation of laboratory tests in the diagnosis of infectious diseases. Format: Combination of 1-hour lecture/case-based class sessions and 2-hour case-based discussion/demo lab sessions with small groups (see topical syllabus, below). Course Director: David L. Balkwill, Ph.D. Office: Room 526 Office Hours: Open – students are welcome to stop by anytime. Phone: 644-9219 [email protected] Other Instructors: Lecture: Myra Hurt, Ph.D. Small Group Facilitation: Curtis Altmann, Ph.D., Susanne Cappendijk, Ph.D., Trent Clarke, Ph.D., Edward Klatt, M.D., Graham Patrick, Ph.D., and Yanchang Wang, Ph.D. Required Text: Medical Microbiology, 4th Ed. (2002) Murray, Rosenthal, Kobayashi, and Pfaller, Mosby-Year Book, ISBN: 0323012132. Recommended Texts: Mechanisms of Microbial Disease, 3rd Ed. (1998) Schaechter, Engelberg, Eisenstein, and Medoff, Lippincott, ISBN: 0683076051. -

XI. COMPLICATIONS of PREGNANCY, Childbffith and the PUERPERIUM 630 Hydatidiform Mole Trophoblastic Disease NOS Vesicular Mole Ex
XI. COMPLICATIONS OF PREGNANCY, CHILDBffiTH AND THE PUERPERIUM PREGNANCY WITH ABORTIVE OUTCOME (630-639) 630 Hydatidiform mole Trophoblastic disease NOS Vesicular mole Excludes: chorionepithelioma (181) 631 Other abnormal product of conception Blighted ovum Mole: NOS carneous fleshy Excludes: with mention of conditions in 630 (630) 632 Missed abortion Early fetal death with retention of dead fetus Retained products of conception, not following spontaneous or induced abortion or delivery Excludes: failed induced abortion (638) missed delivery (656.4) with abnormal product of conception (630, 631) 633 Ectopic pregnancy Includes: ruptured ectopic pregnancy 633.0 Abdominal pregnancy 633.1 Tubalpregnancy Fallopian pregnancy Rupture of (fallopian) tube due to pregnancy Tubal abortion 633.2 Ovarian pregnancy 633.8 Other ectopic pregnancy Pregnancy: Pregnancy: cervical intraligamentous combined mesometric cornual mural - 355- 356 TABULAR LIST 633.9 Unspecified The following fourth-digit subdivisions are for use with categories 634-638: .0 Complicated by genital tract and pelvic infection [any condition listed in 639.0] .1 Complicated by delayed or excessive haemorrhage [any condition listed in 639.1] .2 Complicated by damage to pelvic organs and tissues [any condi- tion listed in 639.2] .3 Complicated by renal failure [any condition listed in 639.3] .4 Complicated by metabolic disorder [any condition listed in 639.4] .5 Complicated by shock [any condition listed in 639.5] .6 Complicated by embolism [any condition listed in 639.6] .7 With other -

February 1, 2008 May 1, 2010 ABSCESS Staphyloccus Aureus
Winnipeg Regional Health Authority Infection Prevention & Control Manual Clinical Presentation, Type of Infective Material Route of Incubation Period of Duration of Comments Microorganism, Infectious Precautions Transmission Communicability Precautions Disease ABSCESS Minor: Pus Direct & indirect Variable Duration of drainage Duration of Minor: Drainage is contained by Staphyloccus aureus Routine contact drainage dressing. Group A Streptococcus Major: Drainage not contained by Major: Other bacteria dressing. Contact ACQUIRED IMMUNE DEFICIENCY Routine Blood, body fluids Mucosal or Weeks to From onset of For life Follow the WRHA Post Exposure SYNDROME containing visible percutaneous years infection Blood & Body Fluid Post Exposure AIDS, ARC, or HIV blood, CSF, pleural exposure to Protocol Management Policy. Report an exposure to infective Antibody Positive, peritoneal, infective pericardial, amniotic material material e.g., needle-stick or blood Suspected Human fluids, semen, & Breastmilk spill/splash immediately to the Immunodeficiency vaginal secretions ingestion Occupational Health Department. Virus (HIV) Infection Refer to Specific Disease Protocol: AIDS/HIV. ACTINOMYCOSIS Routine Not person to Normal flora: infection usually Actinomyces species person secondary to trauma. ADENOVIRUS Routine Eye drainage Direct & indirect 2-14 days Until symptoms Duration of Different strains can be responsible for Conjunctivitis Children <6 yrs: contact cease illness respiratory and gastrointestinal disease. Contact Minimize exposure of immunocompromised -

Author Section
AUTHOR SECTION patients with new onset of fever, demographic, clinical, and laborato- Mycoplasma spp. Overall, the spectrum of antibacterial activity indi- ry variables were obtained during the 2 days after inclusion, while cates a potential role for this combination in the treatment of diffi- microbiological results for a follow-up period of 7 days were collect- cult-to-treat Gram-positive infections, including those caused by ed. Patients were followed up for survival or death, up to a maximum multidrug-resistant organisms. Since this activity extends to Gram- of 28 days after inclusion. MEASUREMENTS AND RESULTS: Of negative respiratory bacteria, quinupristin/dalfopristin may also find all patients, 95% had SIRS, 44% had sepsis with a microbiologically a role in the treatment of atypical, as well as typical, pneumonia. confirmed infection, and 9% died. A model with a set of variables all significantly (p<0.01) contributing to the prediction of mortality was Boubaker A. et al. [Investigation of the urinary tract in children in nuclear med- derived.The set included the presence of hospital-acquired fever, the icine]. Rev Med Suisse Romande. 2000; 120(3) : 251-7.p Abstract: peak respiratory rate, the nadir score on the Glasgow coma scale, and The early detection of urologic abnormalities by antenatal sonogra- the nadir albumin plasma level within the first 2 days after inclusion. phy has resulted in the investigation of many infants and neonates for This set of variables predicted mortality for febrile patients with suspicion of either obstructive uropathy or reflux nephropathy. microbiologically confirmed infection even better.The predictive val- Nuclear medicine techniques allow to assess renal parenchyma ues for mortality of SIRS and sepsis were less than that of our set of integrity, to detect pyelonephritic scars and to measure absolute and variables. -

Meningitis Protocol
Winnipeg Regional Health Authority Acute Care Infection Prevention & Control Manual MENINGITIS PROTOCOL Meningitis is an inflammation of the meninges, the thin lining that surrounds the brain and spinal cord. It can be caused by many bacteria and viruses. Viral infections are the most common cause of meningitis; bacterial infections are the second most common cause. Other rarer causes of meningitis include fungi, parasites, and non-infectious causes, including those related to drugs. Severity of illness and treatment for meningitis differ depending on the cause. It is therefore important to know the specific cause of meningitis: bacterial meningitis is usually more severe than viral, fungal, or parasitic meningitis. Implement Droplet Precautions for all suspect meningitis types until a type has been confirmed/diagnosis determined. Not all cases of meningitis require Additional Precautions. Pediatric: • Implement Droplet/Contact Precautions until etiology determined. • If confirmed as bacterial in origin, implement Droplet Precautions. • If confirmed as viral in origin, implement Contact Precautions for children who are incontinent or unable to comply with hygiene practice. Adult: implement Droplet Precautions until Neisseria meningitidis ruled out. Type of Type of Meningitis Duration of Precautions Precautions Etiology unknown – adult Droplet Until etiology is determined Etiology unknown – pediatric Droplet/Contact Haemophilus influenzae Routine Practices Ongoing type B – adult Haemophilus influenzae Until 24 hours after Droplet type -

Glossary of Icd-10 Codes
glossary of icd-10 codes List of 113 Causes of Death (1999-present) Cause of Death ICD-10 Codes Salmonella infections A01-A02 Shigellosis and amebiasis A03, A06 Certain other intestinal infections A04, A07-A09 Tuberculosis A16-A19 Respiratory Tuberculosis A16 Other Tuberculosis A17-A19 Whooping cough A37 Scarlet fever and erysipelas A38, A46 Meningococcal infection A39 Septicemia A40-A41 Syphilis A50-A53 Acute poliomyelitis A80 Arthropod-borne viral encephalitis A83-A84, A85.2 Measles B05 Viral Hepatitis B15-B19 Human immunodeficiency virus (HIV) disease B20-B24 Malaria B50-B54 Other and unspecified infections and parasitic diseases and their sequelae A00, A05, A20-A36, A42-A44, A48-A49, A54-A79, A81-A82, A85.0-A85.1, A85.8, A86-B04, B06-B09, B25-B49, B55-B99 Malignant neoplasm C00-C97 Malignant neoplasm of lip, oral cavity and pharynx C00-C14 Malignant neoplasm of esophagus C15 Malignant neoplasm of stomach C16 Malignant neoplasm of colon, rectum, anus C18-C21 Malignant neoplasm of liver and intrahepatic bile ducts C22 Malignant neoplasm of pancreas C25 Malignant neoplasm of larynx C32 Malignant neoplasm of trachea, bronchus and lung C33-C34 Malignant melanoma of skin C43 Malignant neoplasm of breast C50 Malignant neoplasm of cervix uteri C53 Malignant neoplasm of corpus uteri and uterus, part unspecified C54-C55 Malignant neoplasm of ovary C56 Malignant neoplasm of prostate C61 Malignant neoplasm of kidney and renal pelvis C64-C65 Malignant neoplasm of bladder C67 Malignant neoplasm of meninges, brain, and other parts of central nervous -

Reportable Disease Desk Reference
Page 1 REPORTABLE DISEASE DESK REFERENCE Division of Epidemiology and Health Planning Department for Public Health Commonwealth of Kentucky April, 2006 Page 2 FOREWORD In the United States, requirements for reporting diseases are mandated by state laws or regulations, and the list of reportable diseases in each state varies. The Kentucky Disease Surveillance Administrative Regulations 902 KAR 2:020 require reporting of Communicable Diseases to the local health departments and the Kentucky Department for Public Health. Additionally, state health departments report cases of selected diseases to the Centers for Disease Control and Prevention (CDC) National Notifiable Disease Surveillance System (NNDSS), on a weekly basis. These data are published weekly in the Morbidity Mortality Weekly Report (MMWR). An updated final report is published annually in the Summary of Notifiable Diseases. With the 2006 version of the desk reference, we have tried to adhere as closely as possible to the case definitions developed by the CDC and the Council of State and Territorial Epidemiologists (CSTE) published in “Case Definitions for Public Health Surveillance”, MMWR 1997; 46:RR-10 and available on the CDC’s Epidemiology Program Office website, http://www.cdc.gov/epo/dphsi/casedef/index.htm. As uniform case definitions are adopted by the states, the incidence of reported diseases in different geographic areas may be more meaningfully compared at the local, state, and national levels. KYEPHRS AND THE DISEASE SURVEILLANCE MODULE The Kentucky Electronic Public Health Record System (KY-EPHRS) provides the backbone of an integrated electronic health record, including disease surveillance. The Disease Surveillance is one of several modules that make up KY-EPHRS.