Guidebook On
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

EAACI/ESCD Skin Allergy Meeting 2017 (SAM 2017)
Clin Transl Allergy 2017, 7(Suppl 4):47 DOI 10.1186/s13601-017-0184-5 Clinical and Translational Allergy MEETING ABSTRACTS Open Access EAACI/ESCD Skin Allergy Meeting 2017 (SAM 2017) Zurich, Switzerland. 27 – 29 April 2017 Published: 15 December 2017 Thursday, 27 April 2017 O02 Assessment of aggregate consumer exposure to isothiazolinones O01 via cosmetics and detergents Methylisothiazolinone contact allergy: a real outbreak Elena Garcia Hidalgo, Natalie Von Goetz, Konrad Hungerbühler Luis Amaral1, Emidio Silva2, Marcio Oliveira3, Ana Paula Cunha4 ETH Zürich, Zürich, Switzerland 1Serviço de Imunoalergologia, Centro Hospitalar de São João E.P.E., Porto, Correspondence: Elena Garcia Hidalgo ‑ [email protected] Portugal; 2Serviço de Medicina do Trabalho e Saúde Ocupacional, Centro Clinical and Translational Allergy 2017, 7(Supple 4):O02 Hospitalar do Baixo Vouga E.P.E., Aveiro, Portugal; 3Serviço de Saúde Ocu‑ pacional, Centro Hospitalar de São João E.P.E., Porto, Portugal; 4Serviço de Background: Isothiazoliones can cause allergic contact dermati- Dermatologia, Centro Hospitalar de São João E.P.E., Porto, Portugal tis and are present in a variety of consumer products, such as cos- Correspondence: Luis Amaral ‑ [email protected] metics, detergents and do-it-yourself products. Skin sensitization Clinical and Translational Allergy 2017, 7(Supple 4):O01 is induced following dermal exposure to a sensitizer in an amount exceeding the sensitization threshold. The critical determinant of Background: Methylisothiazolinone (MI) is used as a preservative in exposure for evaluating skin sensitization risks is dose per unit area occupational, domestic products and, since 2005, in cosmetics. It is a of exposed skin. -

Download WAO White Book on Allergy
WORLD ALLERGY ORGANIZATION WAWAOO WhiteWhite BookBook onon AllergyAllergy WAO White Book on Allergy World Allergy Organization (WAO) White Book on Allergy Copyright 2011 World Allergy Organization WAO White Book on Allergy Editors Prof. Ruby Pawankar, MD, PhD Prof. Giorgio Walter Canonica, MD WAO President Elect (2010-2011) WAO Past President (2010-2011) Allergy and Rhinology Allergy & Respiratory Diseases Nippon Medical School Department of Internal Medicine 1-1-5 Sendagi, Bunkyo-ku University of Genoa Tokyo 113-8603 Padiglione Maragliano, Largo Rosanna Benzi 10 JAPAN 1-16132 Genoa ITALY Prof. Stephen T. Holgate, BSc, MD, DSc, FMed Sci Prof. Richard F. Lockey, MD Member, WAO Board of Directors (2010-2011) WAO President (2010-2011) Medical Research Council Clinical Professor of Division of Allergy & Immunology Immunopharmacology Joy McCann Culverhouse Chair in Allergy & Immunology Infection, Inflammation and Immunity University of South Florida College of Medicine School of Medicine James Haley Veterans Administration Medical Center (111D) University of Southampton 13000 Bruce B. Downs Boulevard Level F, South Block Tampa, Florida 33612 Southampton General Hospital USA Tremona Road Southampton SO16 6YD United Kingdom Acknowledgement On behalf of the World Allergy Organization (WAO), the editors and authors of the WAO White Book on Allergy express their gratitude to the charity, Asthma, Allergy, Inflammation Research (AAIR) and Asian Allergy Asthma Foundation (AAAF) for their support in the production of this publication. The Editors of the White book extend their gratitude to His Excellency Dr. APJ Abdul Kalam, Former President of India and Madame Ilora Finlay Baronness of the House of Lords for their Forewords to the White Book and to the International Primary Care Respiratory Group (IPCRG) and European Federation of Allergy and Airways Diseases Patients ‘Associations (EFA) for their supporting statements. -
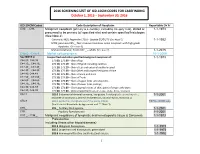
2016 SCREENING LIST of ICD-10CM CODES for CASEFINDING October 1, 2015 – September 30, 2016
2016 SCREENING LIST OF ICD-10CM CODES FOR CASEFINDING October 1, 2015 – September 30, 2016 ICD-10-CM Codes Code Description of Neoplasm Reportable Dx Yr C00._- C96._ Malignant neoplasm (primary & secondary; excluding category C44), stated or 1-1-1973 presumed to be primary (of specified site) and certain specified histologies (See Note 2) Carcinoid, NOS; Appendix C18.0 - Update 01/01/15 (See Note 5) 1-1-1992 MCN; pancreas C25._; Non-invasive mucinous cystic neoplasm with high grade dysplasia. (See note 6) Mature teratoma; Testis C62._ – adults (See note 7) 1-1-2015 C4a.0_-C4a.9_ Merkel cell carcinoma 10-1-2009 See NOTE 4 Unspecified and other specified malignant neoplasm of : 1-1-1973 C44.00.-C44.09 173.00, 173.09 – Skin of Lip C44.10_, C44.19_ 173.10, 173.19 – Skin of Eyelid including canthus C44.20_, C44.29_ 173. 20, 173.29 – Skin of Ear and external auditory canal C44.30_, C44.39_ 173.30, 173.39 – Skin Other and unspecified parts of face C44.40, C44.49 173. 40, 173.49 – Skin of Scalp and neck C44.50_, C44.59_ 173.50, 173.59 – Skin of Trunk C44.60_, C44.69_ 173. 60, 173.69 – Skin of Upper limb and shoulder, C44.70_, C44.79_ 173.70, 173.79 – Skin of Lower limb and hip; C44.80, C44.89 173.80, 173.89 – Overlapping lesions of skin, point of origin unknown; C44.90, C44.99 173.90, 173.99 - Sites unspecified (excludes Labia, Vulva, Penis, Scrotum) C54.1 182.0 Endometrial stromal sarcoma, low grade; Endolymphatic stromal myosis ; 1-1-2001 Endometrial stromatosis, Stromal endometriosis, Stromal myosis, NOS (C54.1) C56.9 183.0 Borderline malignancies -

Urticaria from Wikipedia, the Free Encyclopedia Jump To: Navigation, Search "Hives" Redirects Here
Urticaria From Wikipedia, the free encyclopedia Jump to: navigation, search "Hives" redirects here. For other uses, see Hive. Urticaria Classification and external resourcesICD-10L50.ICD- 9708DiseasesDB13606MedlinePlus000845eMedicineemerg/628 MeSHD014581Urtic aria (or hives) is a skin condition, commonly caused by an allergic reaction, that is characterized by raised red skin wheals (welts). It is also known as nettle rash or uredo. Wheals from urticaria can appear anywhere on the body, including the face, lips, tongue, throat, and ears. The wheals may vary in size from about 5 mm (0.2 inches) in diameter to the size of a dinner plate; they typically itch severely, sting, or burn, and often have a pale border. Urticaria is generally caused by direct contact with an allergenic substance, or an immune response to food or some other allergen, but can also appear for other reasons, notably emotional stress. The rash can be triggered by quite innocent events, such as mere rubbing or exposure to cold. Contents [hide] * 1 Pathophysiology * 2 Differential diagnosis * 3 Types * 4 Related conditions * 5 Treatment and management o 5.1 Histamine antagonists o 5.2 Other o 5.3 Dietary * 6 See also * 7 References * 8 External links [edit] Pathophysiology Allergic urticaria on the shin induced by an antibiotic The skin lesions of urticarial disease are caused by an inflammatory reaction in the skin, causing leakage of capillaries in the dermis, and resulting in an edema which persists until the interstitial fluid is absorbed into the surrounding cells. Urticarial disease is thought to be caused by the release of histamine and other mediators of inflammation (cytokines) from cells in the skin. -

Scientific and Medical Aspects of Apheresis: Issues and Evidence 3 ● Scientific and Medical Aspects of Apheresis: Issues and Evidence
3 Scientific and Medical Aspects of Apheresis: Issues and Evidence 3 ● Scientific and Medical Aspects of Apheresis: Issues and Evidence Various types of apheresis procedures have paucity of high-quality research, conclusions been performed on a clinical basis for many years, about the safety, efficacy, and effectiveness of but the number of patients and types of diseases apheresis are necessarily limited, although some treated have risen significantly in the last 5 years. tentative conclusions and directions for treatment This increase is partially due to increased under- can be discerned. standing of the disease and partially due to engi- The present chapter analyzes the methodolog- neering advances in equipment technologies. By ical problems in conducting apheresis research and almost any standard, treatment by apheresis is still examines available evidence of the safety, ef- in relatively early stages of development—there ficacy, and effectiveness of apheresis. Following are no ideal protocols based on a thorough un- a discussion of methodological issues, several derstanding of reasons for its efficacy. Never- major reviews of apheresis research will be sum- theless, there is an increasing flow of clinical data, marized and evaluated. This chapter will further sometimes describing dramatic patient improve- include the findings of a primary literature review ment, supporting the view that apheresis is a and assessment of apheresis in the treatment of rapidly emerging technology with significant three diseases—namely, hemolytic uremic syn- promise (117). Such evidence of treatment effec- drome, acquired Factor-VIII inhibitor, and Guil- tiveness’ is even today, however, often based on lain-Barré syndrome— where preliminary reports unsystematically collected data. -
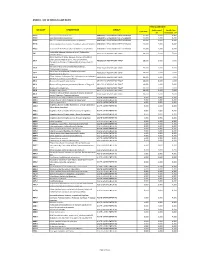
Annex 1: List of Medical Case Rates
ANNEX 1. LIST OF MEDICAL CASE RATES FIRST CASE RATE ICD CODE DESCRIPTION GROUP Professional Health Care Case Rate Fee Institution Fee P91.3 Neonatal cerebral irritability ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.4 Neonatal cerebral depression ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.6 Hypoxic ischemic encephalopathy of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.8 Other specified disturbances of cerebral status of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.9 Disturbance of cerebral status of newborn, unspecified ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 Peritonsillar abscess; Abscess of tonsil; Peritonsillar J36 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 cellulitis; Quinsy Other diseases of larynx; Abscess of larynx; Cellulitis of larynx; Disease NOS of larynx; Necrosis of larynx; J38.7 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Pachyderma of larynx; Perichondritis of larynx; Ulcer of larynx Retropharyngeal and parapharyngeal abscess; J39.0 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Peripharyngeal abscess Other abscess of pharynx; Cellulitis of pharynx; J39.1 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Nasopharyngeal abscess Other diseases of pharynx; Cyst of pharynx or nasopharynx; J39.2 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Oedema of pharynx or nasopharynx J85.1 Abscess of lung with pneumonia ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 J85.2 Abscess of lung without pneumonia; Abscess of lung NOS ABSCESS OF RESPIRATORY -

Natural Remedies of Common Human Parasites and Pathogens
ACTA SCIENTIFIC MICROBIOLOGY (ISSN: 2581-3226) Volume 2 Issue 11 November 2019 Investigation Paper Natural Remedies of Common Human Parasites and Pathogens Omar M Amin* Parasitology Center, Scottsdale, Arizona *Corresponding Author: Omar M Amin, Parasitology Center, Scottsdale, Arizona. Received: July 12, 2019; Published: October 16, 2019 DOI: 10.31080/ASMI.2019.02.0401 • Bleeding. • Appetite changes. • Malabsorption. • Mucus. • Rectal itching. • Gut leakage. • Poor digestion. • Systemic/other symptoms • Fatigue. • Skin rash. • Dry cough. • Brain fog/memory loss. • Lymph blockage. Figure 1 • Allergies. • Nausea. Diagnosis and management of: • Muscle or joint pain. • Parasitic organisms and agents of medical and public • Dermatitis. health importance in fecal, blood, skin, urine specimens. • Headaches. • Toxicities related to Neurocutaneous Syndrome (NCS). • Insomnia. Development of anti-parasitic herbal products (F/C/R) Edu- How we get infected cational services: workshops, seminars, training and publications Drinking water or juice: Giardia, Cryptosporidium. provided. 1. 2. Skin contact with contaminated water: Schistosomi- Consultations and protocols for herbal and allopathic treat- asis, swimmers itch. ments. Research: over 220 publications on parasites from all con- Food (fecal-oral infections): most protozoans, ex., tinents. 3. Blastocysts, Entamoeba spp. and worms: Ascaris. Why test? 4. Arthropods: Lyme disease, plague, typhus, etc. You need to be tested if you have one or more of these symp- 5. Air: Upper respiratory tract infections (viruses, bac- toms: teria), ex GI symptoms 6. Pets: Hydatid., flu, Valleycyst disease,fever, Hanta heart virus. worm, larva mi- grans (dogs), Toxoplasma (cats), Taenia (beef, swine. • Diarrhea/constipation. People (contagious diseases): AIDS, herpes. • Irritable bowel 7. Soil: hook worms, thread worms. • Cramps 8. -

LIST of OCCUPATIONAL DISEASES (Revised 2010)
LIST OF OCCUPATIONAL DISEASES (revised 2010) Identification and recognition of occupational diseases: Criteria for incorporating diseases in the ILO list of occupational diseases Occupational Safety and Health Series, No. 74 List of occupational diseases (revised 2010) Identification and recognition of occupational diseases: Criteria for incorporating diseases in the ILO list of occupational diseases INTERNATIONAL LABOUR OFFICE • GENEVA Copyright © International Labour Organization 2010 First published 2010 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Convention. Nevertheless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to ILO Publications (Rights and Permissions), International Labour Office, CH-1211 Geneva 22, Switzerland, or by email: pubdroit@ ilo.org. The International Labour Office welcomes such applications. Libraries, institutions and other users registered with reproduction rights organizations may make copies in accordance with the licences issued to them for this purpose. Visit www.ifrro.org to find the reproduction rights organization in your country. ILO List of occupational diseases (revised 2010). Identification and recognition of occupational diseases: Criteria for incorporating diseases in the ILO list of occupational diseases Geneva, International Labour Office, 2010 (Occupational Safety and Health Series, No. 74) occupational disease / definition. 13.04.3 ISBN 978-92-2-123795-2 ISSN 0078-3129 Also available in French: Liste des maladies professionnelles (révisée en 2010): Identification et reconnaissance des maladies professionnelles: critères pour incorporer des maladies dans la liste des maladies professionnelles de l’OIT (ISBN 978-92-2-223795-1, ISSN 0250-412x), Geneva, 2010, and in Spanish: Lista de enfermedades profesionales (revisada en 2010). -

ICD-10 International Statistical Classification of Diseases and Related Health Problems
ICD-10 International Statistical Classification of Diseases and Related Health Problems 10th Revision Volume 2 Instruction manual 2010 Edition WHO Library Cataloguing-in-Publication Data International statistical classification of diseases and related health problems. - 10th revision, edition 2010. 3 v. Contents: v. 1. Tabular list – v. 2. Instruction manual – v. 3. Alphabetical index. 1.Diseases - classification. 2.Classification. 3.Manuals. I.World Health Organization. II.ICD-10. ISBN 978 92 4 154834 2 (NLM classification: WB 15) © World Health Organization 2011 All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. -

THE DEVELOPMENT of NEUROLOGY in BELFAST by H
THE DEVELOPMENT OF NEUROLOGY IN BELFAST by H. G. CALWELL Offices of Archives, Royal Victoria Hospital, Belfast BEFORE the middle of the nineteenth century no special facilities existed in the United Kingdom for the care and treatment of sufferers from diseases of the nervous system. It was the policy of general hospitals not to admit any patient suffering from an incurable disease, and patients with epilepsy were generally refused admission, not because treatment was unavailable,-but because of the effect of the fits on other patients. Hospitals and institutions for the treatment of "nervous diseases" existed before the nineteenth century, but these did not cater for diseases of the nervous system as we understand them in the context of neurology. One such example is the institution founded by Dean Swift in Dublin in 1745. Its title was St. Patrick's Hospital for the Treatment of Nervous and Mental Diseases. It was in fact, in the parlance of the time, a madhouse. In the satiric poem written by Swift in 1731 which he entitled "On the Death of Dean Swift" there is a verse:- He gave the little wealth he had To build a house for fools and mad And shewed by one satiric touch No nation wanted it so much. In these lines Swift made it clear that he was extending his bounty to the insane, not the paralysed. If we look at the teaching of a famous physician in Edinburgh in the eighteenth century we find that Professor William Cullen in his First Lines on the Practice of Physic (1777) included a section entitled "Of Neuroses or Nervous Diseases". -

FAQ REGARDING DISEASE REPORTING in MONTANA | Rev
Disease Reporting in Montana: Frequently Asked Questions Title 50 Section 1-202 of the Montana Code Annotated (MCA) outlines the general powers and duties of the Montana Department of Public Health & Human Services (DPHHS). The three primary duties that serve as the foundation for disease reporting in Montana state that DPHHS shall: • Study conditions affecting the citizens of the state by making use of birth, death, and sickness records; • Make investigations, disseminate information, and make recommendations for control of diseases and improvement of public health to persons, groups, or the public; and • Adopt and enforce rules regarding the reporting and control of communicable diseases. In order to meet these obligations, DPHHS works closely with local health jurisdictions to collect and analyze disease reports. Although anyone may report a case of communicable disease, such reports are submitted primarily by health care providers and laboratories. The Administrative Rules of Montana (ARM), Title 37, Chapter 114, Communicable Disease Control, outline the rules for communicable disease control, including disease reporting. Communicable disease surveillance is defined as the ongoing collection, analysis, interpretation, and dissemination of disease data. Accurate and timely disease reporting is the foundation of an effective surveillance program, which is key to applying effective public health interventions to mitigate the impact of disease. What diseases are reportable? A list of reportable diseases is maintained in ARM 37.114.203. The list continues to evolve and is consistent with the Council of State and Territorial Epidemiologists (CSTE) list of Nationally Notifiable Diseases maintained by the Centers for Disease Control and Prevention (CDC). In addition to the named conditions on the list, any occurrence of a case/cases of communicable disease in the 20th edition of the Control of Communicable Diseases Manual with a frequency in excess of normal expectancy or any unusual incident of unexplained illness or death in a human or animal should be reported. -

Commonly Coded Conditions in Dermatology
2/11/2014 Commonly Coded Conditions in Dermatology Betty Hovey, CPC, CPC-H, CPB, CPMA, CPC-I, CPCD Director, ICD-10 Development and Training AAPC Commonly Coded Conditions in Dermatology No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or mechanically, including photocopying, recording, or taping) without the expressed written permission of AAPC. 2 Commonly Coded Conditions in Dermatology AGENDA • Dermatitis • Actinic and seborrheic keratosis • Acne • Ulcers • Psoriasis Commonly Coded Conditions in Dermatology 1 2/11/2014 Commonly Coded Conditions in Dermatology Dermatitis • Inflammation of the skin • Comes in different forms • We will discuss: – Atopic dermatitis – Seborrheic dermatitis – Contact dermatitis • NOTE: For code block L20-L30 ICD-10-CM uses the terms dermatitis and eczema synonymously and interchangeably. Commonly Coded Conditions in Dermatology Atopic dermatitis (AD) • Located in category L20: – L20.0 Besnier’s prurigo – L20.81 Atopic neurodermatitis – L20.82 Flexural eczema – L20.83 Infantile (acute) (chronic) eczema – L20.84 Intrinsic (allergic) eczema – L20.89 Other atopic dermatitis – L20.9 Atopic dermatitis, unspecified Commonly Coded Conditions in Dermatology 2 2/11/2014 Example • 7-year-old girl brought in for itchy, popular rash on the flexural surfaces of the neck, axillae, and elbows. No other family members with AD, but mother has asthma. Scratching of the lesions is worse at night. Patient with lichenification in left elbow area. Patient is diagnosed with flexural dermatitis. L20.82 Flexural eczema Z82.5 Family history of asthma and other chronic lower respiratory diseases Commonly Coded Conditions in Dermatology Seborrheic dermatitis • Located in category L21 L21.0 Seborrheic capitis L21.1 Seborrheic infantile L21.8 Other seborrheic dermatitis L21.9 Seborrheic dermatitis, unspecified Commonly Coded Conditions in Dermatology Example • A new mother brings her infant in because she is worried about a yellowish, crusty deposit on the baby’s scalp.