Die Prinzipien Der Chirurgischen Therapie Beim Fortgeschrittenen
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vesicular and Ulcerative Dermatopathy Resembling Superficial Necrolytic Dermatitis in Captive Black Rhinoceroses (Diceros Bicornis)
Vet Path01 353 1-42 (1998) Vesicular and Ulcerative Dermatopathy Resembling Superficial Necrolytic Dermatitis in Captive Black Rhinoceroses (Diceros bicornis) L. MUNSON, J. W. KOEHLER, J. E. WILKINSON, AND R. E. MILLER Department of Pathology, College of Veterinary Medicine, University of Tennessee,Knoxville, TN (LM, JWK, JEW); and Department of Animal Health, St. Louis Zoological Park, St. Louis, MO (REM) Abstract. The histopathology, clinical presentation, and epidemiology of a cutaneous and oral mucosal disease affecting 40 black rhinoceroses (Diceros bicomis) at 21 zoological parks (50% of the captive US population) were investigated. Twenty-seven biopsies were examined from recent lesions, and clinical infor- mation was available from 127 episodes.The cutaneous lesions began as plaques that progressedto vesicles, bullae, or ulcers. Lesions waxed and waned in individual cases.Lesions were predominantly bilaterally sym- metrical, affecting pressurepoints, coronary bands, tips of the ears and tail, and along the lateral body wall and dorsum. Oral lesions were first noticed as ulcers and were present on the lateral margins of the tongue, palate, and mucocutaneousjunctions of the lips. All recent lesions had similar histopathologic findings of prominent acanthosis,hydropic degenerationof keratinocytes in the stratum spinosum,spongiosis, intraepithelial vesicles, and parakeratosiswithout dermal inflammation. Chronic lesions were ulcerated. No pathogens were identified by culture or electron microscopy. Most episodescoincided with stressevents -

PLENARY SESSION ABSTRACTS Theme: IMMUNITY and AUTOIMMUNITY
PLENARY SESSION ABSTRACTS Theme: IMMUNITY AND AUTOIMMUNITY State-of-the-Art Address Supporting Review What’s new in autoimmune blistering diseases? Epithelial, immune cell and microbial cross- D. F. MURRELL talk in homeostasis and atopic dermatitis Department of Dermatology, St George Hospital, and T. KOBAYASHI UNSW Faculty of Medicine, Sydney, New South Wales, Laboratory for Innate Immune Systems, RIKEN Center Australia for Integrative Medical Sciences (IMS), Yokohama, There are several blistering diseases which occur natu- Japan rally in other species as well as in humans; for example, Skin is a complex and dynamic ecosystem, wherein the pemphigus occurs naturally in dogs and horses and the epithelial cells, immune cells and microbiota engage in inherited blistering disease, epidermolysis bullosa, also active dialogues and maintain barrier integrity and occurs in dogs. Several new validated scoring systems functional immunity. Alterations of the peaceful coexis- to measure the severity of autoimmune blistering dis- tence with the resident microbiota, referred to as dys- ease (AIBD) have been developed which assist in biosis, lead to dysregulation of host immunity. It has demonstrating efficacy of new treatments, such as the been long debated whether the dysbiosis in the skin of Pemphigus Disease Area Index (PDAI) for pemphigus atopic dermatitis is merely a consequence of chronic and Bullous Pemphigoid Disease Area Index (BPDAI) skin inflammation or whether it is actively involved in for pemphigoid. Pemphigus is due to autoantibodies to driving skin inflammation. Microbiome analysis by 16S desmogleins 1 and 3 in human pemphigus foliaceus and rRNA sequencing in humans and dogs with atopic der- vulgaris and desmocollin1 in canine pemphigus foli- matitis showed the shifts in microbial diversity repre- aceus, generated by the late onset activation of the sented by increased proportion of Staphylococcus spp. -
Annex 1: List of Medical Case Rates
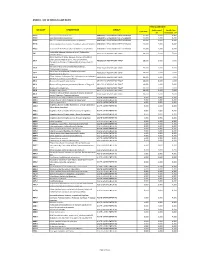
ANNEX 1. LIST OF MEDICAL CASE RATES FIRST CASE RATE ICD CODE DESCRIPTION GROUP Professional Health Care Case Rate Fee Institution Fee P91.3 Neonatal cerebral irritability ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.4 Neonatal cerebral depression ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.6 Hypoxic ischemic encephalopathy of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.8 Other specified disturbances of cerebral status of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.9 Disturbance of cerebral status of newborn, unspecified ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 Peritonsillar abscess; Abscess of tonsil; Peritonsillar J36 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 cellulitis; Quinsy Other diseases of larynx; Abscess of larynx; Cellulitis of larynx; Disease NOS of larynx; Necrosis of larynx; J38.7 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Pachyderma of larynx; Perichondritis of larynx; Ulcer of larynx Retropharyngeal and parapharyngeal abscess; J39.0 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Peripharyngeal abscess Other abscess of pharynx; Cellulitis of pharynx; J39.1 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Nasopharyngeal abscess Other diseases of pharynx; Cyst of pharynx or nasopharynx; J39.2 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Oedema of pharynx or nasopharynx J85.1 Abscess of lung with pneumonia ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 J85.2 Abscess of lung without pneumonia; Abscess of lung NOS ABSCESS OF RESPIRATORY -

Natural Remedies of Common Human Parasites and Pathogens
ACTA SCIENTIFIC MICROBIOLOGY (ISSN: 2581-3226) Volume 2 Issue 11 November 2019 Investigation Paper Natural Remedies of Common Human Parasites and Pathogens Omar M Amin* Parasitology Center, Scottsdale, Arizona *Corresponding Author: Omar M Amin, Parasitology Center, Scottsdale, Arizona. Received: July 12, 2019; Published: October 16, 2019 DOI: 10.31080/ASMI.2019.02.0401 • Bleeding. • Appetite changes. • Malabsorption. • Mucus. • Rectal itching. • Gut leakage. • Poor digestion. • Systemic/other symptoms • Fatigue. • Skin rash. • Dry cough. • Brain fog/memory loss. • Lymph blockage. Figure 1 • Allergies. • Nausea. Diagnosis and management of: • Muscle or joint pain. • Parasitic organisms and agents of medical and public • Dermatitis. health importance in fecal, blood, skin, urine specimens. • Headaches. • Toxicities related to Neurocutaneous Syndrome (NCS). • Insomnia. Development of anti-parasitic herbal products (F/C/R) Edu- How we get infected cational services: workshops, seminars, training and publications Drinking water or juice: Giardia, Cryptosporidium. provided. 1. 2. Skin contact with contaminated water: Schistosomi- Consultations and protocols for herbal and allopathic treat- asis, swimmers itch. ments. Research: over 220 publications on parasites from all con- Food (fecal-oral infections): most protozoans, ex., tinents. 3. Blastocysts, Entamoeba spp. and worms: Ascaris. Why test? 4. Arthropods: Lyme disease, plague, typhus, etc. You need to be tested if you have one or more of these symp- 5. Air: Upper respiratory tract infections (viruses, bac- toms: teria), ex GI symptoms 6. Pets: Hydatid., flu, Valleycyst disease,fever, Hanta heart virus. worm, larva mi- grans (dogs), Toxoplasma (cats), Taenia (beef, swine. • Diarrhea/constipation. People (contagious diseases): AIDS, herpes. • Irritable bowel 7. Soil: hook worms, thread worms. • Cramps 8. -
A Retrospective Study of Idiopathic Ulcerative Dermatitis in Mice with a C57BL/6 Background
Journal of the American Association for Laboratory Animal Science Vol 45, No 6 Copyright 2006 November 2006 by the American Association for Laboratory Animal Science Pages 8-12 Reports A Retrospective Study of Idiopathic Ulcerative Dermatitis in Mice with a C57BL/6 Background Robin J Kastenmayer,* Michele A Fain, and Kathy A Perdue Idiopathic ulcerative dermatitis is a well-recognized disease in C57BL mice and related strains. This disease manifests as a pruritic dermatitis with resulting self-mutilation, dermal ulceration, necrosis, and fibrosis. Ulcerative dermatitis has the ability to confound ongoing research by causing systemic pathologic changes, such as lymphadenopathy and splenomegaly. Although various treatments have been described, none has been curative consistently; therefore, minimizing negative effects on research through prevention of disease is ideal. To identify etiologic factors, we conducted a 2-y retrospective study of 1352 mice with a C57BL/6 genetic background; these mice demonstrated an overall prevalence of 4.1% and a seasonal effect with a peak incidence during midsummer. Corroborating previous studies, our study revealed a disease predilection for female mice. In contrast to prior reports, the disease prevalence was greatest in 10- to 16-mo-old mice. In addition, mice with a C57BL/6 background that were deficient in the gene for inducible nitric oxide synthase had a 50% disease incidence, suggesting a potential animal model for further characterizing the pathogenesis, prevention, and treatment of ulcerative dermatitis. Abbreviations: iNOS, inducible nitric oxide synthase; UD, ulcerative dermatitis Idiopathic ulcerative dermatitis (UD) with pruritus is a Allentown, NJ) with corncob bedding (Harlan Teklad, Madison, common condition in C57BL mice, especially C57BL/6J mice. -

PRODUCT MONOGRAPH Prerbitux®
PRODUCT MONOGRAPH PrERBITUX® (cetuximab) Intravenous Injection, 2 mg cetuximab / mL 50 mL and 100 mL vials Antineoplastic Manufactured by ImClone LLC Date of Authorization: Branchburg, NJ, USA January 10, 2018 Distributed by Date of Revision: Eli Lilly Canada Inc. Exchange Tower August 13, 2020 130 King Street West, Suite 900 P.O. Box 73 Toronto, Ontario M5X 1B1 1-888-545-5972 www.lilly.ca Control No.: 211842 Page 1 of 77 Table of Contents PART I: HEALTH PROFESSIONAL INFORMATION.................................................................................................................3 SUMMARY PRODUCT INFORMATION ...................................................................................................................................3 INDICATIONS AND CLINICAL USE..........................................................................................................................................3 CONTRAINDICATIONS................................................................................................................................................................4 WARNINGS AND PRECAUTIONS.............................................................................................................................................4 ADVERSE REACTIONS.............................................................................................................................................................. 10 DRUG INTERACTIONS............................................................................................................................................................. -

Cutaneous Balamuthia Mandrillaris Infection As a Precursor To
Volume 23 Number 7 | July 2017 Dermatology Online Journal || Case Report DOJ 23 (7): 4 Cutaneous Balamuthia mandrillaris infection as a precursor to Balamuthia amoebic encephalitis (BAE) in a healthy 84-year-old Californian Larisa M Lehmer, Gabriel E Ulibarri, Bruce D Ragsdale, James Kunkle Affiliations: University of California Irvine Health, Department of Dermatology, Irvine, California, Central Coast Pathology Laboratory, San Luis Obispo, California, Western Diagnostic Services Laboratory, San Luis Obispo, California, Central Coast Dermatology, Arroyo Grande, California Corresponding Author: Larisa M Lehmer, Department of Dermatology, UC Irvine Health, 118 Med Surg 1, Irvine, CA 92697-2400, Email: [email protected] Abstract Keywords: Balamuthia mandrillaris; cutaneous balamuthiasis; granulomatous amoebic encephalitis; Soil and freshwater-dwelling amoebae may GAE; balamuthia amoebic encephalitis; BAE; opportunistically infect the skin and evoke a immunocompromise; granulomatous dermatitis; granulomatous dermatitis that camouflages their immune senescence. underlying morphology. Amoebic infestations are incredibly rare in the U.S., predominantly occurring in the young, elderly, and immunocompromised. Introduction Sadly, because diagnosis is difficult and unsuspected, Balamuthia mandrillaris (B. mandrillaris), along most cases are diagnosed at autopsy. The following with Naegleria, Sappinia and several species of case is of a healthy 84-year-old man with a non- Acanthomeba, are free-living amoebae found in fresh healing nodulo-ulcerative cutaneous lesion on his water and soil worldwide that may opportunistically left forearm that appeared following a gardening infect the skin and/or central nervous system (CNS) injury. Lesional punch biopsies repeatedly showed of humans. The first sign of infection ranges from non-specific granulomatous inflammation with a stubborn indurated plaque or ulceration on the no pathogens evident histologically or by culture. -

Ulcerative Dermatitis in C57BL/6 Mice
AN ABSTRACT OF THE THESIS OF Jennifer L. Sargent for the degree of Master of Science in Veterinary Science presented on June 2, 2015 Title: Ulcerative Dermatitis in C57BL/6 Mice Abstract approved: ______________________________________________________________________________ Helen E. Diggs Abstract Ulcerative dermatitis (UD) is a common condition in C57BL/6 mice that is poorly understood and challenging to treat. Inconsistently there have been reports of an increased incidence of the disease in female mice, mice exposed to certain diets, mice of advanced age, and in several seasons. These inconsistencies indicated a need for a systematic review to better assess the evidence for commonly cited UD risk factors and treatments. The aims for the systematic review were to assess the quality of evidence for both: 1) commonly cited risk factors for UD, specifically sex, age, season, and diet; and 2) reported UD treatments. A search of three electronic databases was performed and articles were evaluated using previously published criteria for assessing methodological quality. Dietary factors, particularly caloric restriction, appear to have an effect on UD risk. Female sex was associated with an increased risk of UD in some studies, particularly diet studies, but not in others. Also, UD was seen most commonly in mice between 14 and 24 months of age in the studies reviewed. The role of season was not assessed in any of the articles that met the inclusion criteria. Of the three publications that evaluated UD treatments only one had an untreated or alternative therapy control. Further research is needed to explore epidemiologic aspects of UD and to compare treatment options. -

Aminoglycoside Allergic Reactions
pharmacy Review Aminoglycoside Allergic Reactions Lindsey M. Childs-Kean 1,* , Kristy M. Shaeer 2, Sheeba Varghese Gupta 3 and Jonathan C. Cho 4 1 Department of Pharmacotherapy and Translational Research, University of Florida College of Pharmacy, Gainesville, FL 32610, USA 2 Department of Pharmacotherapeutics and Clinical Research, University of South Florida College of Pharmacy, Tampa, FL 33612, USA 3 Department of Pharmaceutical Sciences, University of South Florida College of Pharmacy, Tampa, FL 33612, USA 4 Department of Clinical Sciences, Ben and Maytee Fisch College of Pharmacy, The University of Texas at Tyler, Tyler, TX 75799, USA * Correspondence: [email protected]fl.edu Received: 13 July 2019; Accepted: 25 August 2019; Published: 29 August 2019 Abstract: Aminoglycosides are antimicrobial agents that are primarily used for infections caused by Gram-negative pathogens. The purpose of this article is to review the allergic reactions reported in the published literature to aminoglycoside antibiotics. A thorough PubMed search was conducted and excluded non-allergic adverse reactions to aminoglycosides. Allergic reactions to aminoglycosides occur infrequently, but can include cutaneous reactions as well as systemic reactions, including anaphylaxis. Of the evaluated aminoglycosides, gentamicin had the most reported allergic reactions, including the most reports of anaphylaxis, followed by tobramycin, and then amikacin. Most reports of allergic reactions occurred in patients who had a prior exposure to some dosage form of an aminoglycoside. Cross-reactivity among aminoglycosides is common and occurs due to the similarities in their chemical structures. Desensitization protocols to tobramycin have been described in the literature. Keywords: aminoglycosides; allergy; hypersensitivity; gentamicin; tobramycin; amikacin 1. Introduction Antibiotics are one of the most common causes of life-threatening medication allergies [1]. -

Differential Diagnosis in Dermatology
Differential Diagnosis in Dermatology ZohrehTehranchi Dermatologist COMMON ACNE AND CYSTIC ACNE Rosacea Rosacea PERIORAL DERMATITIS ECZEMA/DERMATITIS Chronic irritant dermatitis Dyshidrotic eczematous dermatitis Childood atopic dermatitis Autosensitization dermatitis (“id” reaction): dermatophytid Seborrheic dermatitis PSORIASIS VULGARIS Pemphigus vulgaris BULLOUS PEMPHIGOID (BP) Pityriasis rosea small-plaque parapsoriasis Large-plaque parapsoriasis (parapsoriasis en plaques) LICHEN PLANUS (LP) GRANULOMA ANNULARE (GA) Erythema multiforme ERYTHEMA NODOSUM Actinic keratoses Bowen disease (Squamous cell carcinoma in situ) Bowen disease and invasive SCC Squamous cell carcinoma: invasive on the lip Squamous cell carcinoma, well differentiated Squamous cell carcinoma, undifferentiated Squamous cell carcinoma, advanced, well differentiated, on the hand Keratoacanthoma showing different stages of evolution BASAL CELL CARCINOMA (BCC) Basal cell carcinoma, ulcerated: Rodent ulcer A large rodent ulcer in the nuchal and Bas cell calarcinoma: sclerosing type retroauricular area extending to the temple Basal cell carcinoma, sclerosing, nodular, Superficial basal cell carcinoma: solitary lesion and multiple lesions Superficial basal cell carcinoma, invasive Basal cell carcinoma, pigmented Dysplastic nevi Superficial spreading melanoma: arising within a dysplastic nevus Congenital nevomelanocytic nevus Melanoma: arising in small CNMN Melanoma in situ: lentigo maligna Melanoma in situ, superficial spreading type Superficial spreading melanoma, vertical -

View Continuation Patent in PDF Format
I 1111111111111111 1111111111 lllll lllll lllll 111111111111111 111111111111111111 US010144773B2 c12) United States Patent (IO) Patent No.: US 10,144,773 B2 Cook et al. (45) Date of Patent: *Dec. 4, 2018 (54) METHODS OF USE OF SECRETORY IGA WO 2004000035 Al 12/2003 WO 2009156301 Al 12/2009 (71) Applicant: WISCONSIN ALUMNI RESEARCH WO 2012080306 Al 6/2012 WO 2013087911 Al 6/2013 FOUNDATION, Madison, WI (US) WO 2013132052 Al 9/2013 WO 20140107269 Al 7/2014 (72) Inventors: Mark E. Cook, Madison, WI (US); Jordan Marshall Sand, Madison, WI OTHER PUBLICATIONS (US); Lisa Ann Krugner-Higby, Belleville, WI (US); James Mukasa Hampton et al., J Am Assoc Lab Anim Sci. 2012;51(5):586-93.* Ntambi, Fitchburg, WI (US) Nowland et al., "Guidelines on Treatment of Ulcerative Dermatitis" downloaded Jul. 26, 2018 from wiki.med.umich.edu/display/ (73) Assignee: WISCONSIN ALUMNI RESEARCH ULAMGSOP/Guidelines+on+ Treatment +of+ Ulcerative+ Dermati FOUNDATION, Madison, WI (US) tis, 2 pages.* Berneman, et al.; "The Specificity Patterns of Human Immuno ( *) Notice: Subject to any disclaimer, the term ofthis globulin G Antibodies in Serum Differ from Those in Autologous patent is extended or adjusted under 35 Secretions"; Infection and Immunity; pp. 4163-4168; (1998). U.S.C. 154(b) by 150 days. Definition of Feed efficiency, found in "Introduction to Animal Science"; Third Edition; W. Stephen Damron, Ed.; Pearson, Pren This patent is subject to a terminal dis tice Hall; p. 785; 2006. claimer. Karczewski, Jerry; "Animal-Derived Medicines Play a Critical Role in Human Health Care"; Meat+Poultry; Jan. 2017; pp. 16-22; (21) Appl. -

Ulcerative Dermatitis in Mice
Ulcerative Dermatitis in Mice Background Ulcerative dermatitis (UD) is a common idiopathic non-infectious skin condition in mice that is characterized by hair loss, skin redness and itching that rapidly progresses to excoriation and ulceration of the skin as a result of self-trauma.1 Due to the potential discomfort and pain associated with this condition and its high prevalence, UD is considered one of the most important welfare issues in lab mice.1,2 Etiology & Risk Factors While the exact etiology of UD is still unknown, recent literature suggests it may be a type I hypersensitivity response.3,4 The condition has been associated with various other pathologic processes.5-7 Risk factors for the development of UD include:1 C57BL/6 genetic background Increasing age – median age of onset is approximately 15 months8 Sex – earlier onset and higher prevalence in females9 High-fat diet consumption Changes in humidity Investigators planning studies using C57BL/6-background mice, especially aging studies, should anticipate that UD lesions may develop in approximately 20% of the mice8,10 and may require pharmacologic treatment or euthanasia. Management Early recognition and intervention is key for successfully managing UD cases. Lab personnel who are regularly handling their mice may be in the best position to identify early UD lesions that have a good prognosis for recovery. Report any health concerns to DCM for further evaluation so that we may assess the animal and recommend appropriate treatment(s). When DCM veterinary staff diagnose UD, they will assign a severity score and recommend treatment according to the table below.