The Spectrum of Autoimmune Diseases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Do the Lifetime Prevalence and Prognosis of Schizophrenia Differ Among World Regions? Cheryl Lynn Smith
Claremont Colleges Scholarship @ Claremont CMC Senior Theses CMC Student Scholarship 2018 Do the Lifetime Prevalence and Prognosis of Schizophrenia Differ Among World Regions? Cheryl Lynn Smith Recommended Citation Smith, Cheryl Lynn, "Do the Lifetime Prevalence and Prognosis of Schizophrenia Differ Among World Regions?" (2018). CMC Senior Theses. 1978. http://scholarship.claremont.edu/cmc_theses/1978 This Open Access Senior Thesis is brought to you by Scholarship@Claremont. It has been accepted for inclusion in this collection by an authorized administrator. For more information, please contact [email protected]. Do the Lifetime Prevalence and Prognosis of Schizophrenia Differ Among World Regions? A Thesis Presented by Cheryl Lynn Smith To the Keck Science Department Of Claremont McKenna, Pitzer, and Scripps Colleges In partial fulfillment of The degree of Bachelor of Arts Senior Thesis in Human Biology 04/23/2018 LIFETIME PREVALENCE AND PROGNOSIS OF SCHIZOPHRENIA 1 Table of Contents Abstract …………………………………………………………...……………………… 2 1. Introduction………………………………………………...…………...……………… 3 2. Background Information ……………………………...……………………………….. 5 2.1 Historical Background of Schizophrenia ……………………....…………… 5 2.2 Lifetime Prevalence of Schizophrenia …………………………...…..……… 12 2.3 Prognosis in People with Schizophrenia ……………....………...…..……… 13 3. Methods …………………………………………...……………………..……………. 17 4. Results ……………………………………………...…………………….…….…….... 18 5. Discussion ……………………………………………...……………………………… 24 6. Acknowledgements …………………………………………...………………………. -

Diseases/Symptoms Reported to Be Associated with Lyme Disease
Diseases/Symptoms Reported to be Associated with Lyme Disease Abdominal pseudo-eventration Abdominal wall weakness Acrodermatitis chronica atrophicans (ACA) Acute Acral Ischemia Acute conduction disorders Acute coronary syndrome Acute exogenous psychosis Acute febrile illness Acute hemiparesis Acute ischaemic pontine stroke Acute meningitis Acute myelo-meningo-radiculitis Acute myelitis Acute pediatric monoarticular arthritis Acute peripheral facial palsy Acute perimyocarditis Acute posterior multifocal placoid pigment epitheliopathy (APMPPE) Acute pyogenic arthritis Acute reversible diffuse conduction system disease Acute septic arthritis Acute severe encephalitis Acute transitory auriculoventricular block Acute transverse myelitis Acute urinary retention Acquired Immune Deficiency Syndrome (AIDS) Algodystrophy Allergic conditions Allergic conjunctivitis Alopecia Alzheimer’s Disease Amyotrophic lateral sclerosis (ALS - Lou Gehrig's Disease) Amyotrophy Anamnesis Anetoderma Anorexia nervosa Anterior optic neuropathy Antepartum fever Anxiety Arrhythmia Arthralgia Arthritis Asymmetrical hearing loss Ataxic sensory neuropathy Atraumatic spontaneous hemarthrosis Atrioventricular block Attention Deficit Disorder (ADD) Attention Deficit Hyperactivity Disorder (ADHD) Back pain without radiculitis Bannwarth’s Syndrome Behcet's disease Bell’s Palsy Benign cutaneous lymphocytoma Benign lymphocytic infiltration (Jessner-Kanof) Bilateral acute confluent disseminated choroiditis Bilateral carpal tunnel syndrome Bilateral facial nerve palsy Bilateral -

ICD-10-CM TABULAR LIST of DISEASES and INJURIES 2018 Addenda No Change Chapter 1 No Change Certain Infectious and Parasitic Diseases (A00-B99)
ICD-10-CM TABULAR LIST of DISEASES and INJURIES 2018 Addenda No Change Chapter 1 No Change Certain infectious and parasitic diseases (A00-B99) No Change Intestinal infectious diseases (A00-A09) No Change A04 Other bacterial intestinal infections No Change A04.7 Enterocolitis due to Clostridium difficile Add A04.71 Enterocolitis due to Clostridium difficile, recurrent Add A04.72 Enterocolitis due to Clostridium difficile, not specified as recurrent No Change A05 Other bacterial foodborne intoxications, not elsewhere classified No Change Excludes1: Revise from Clostridium difficile foodborne intoxication and infection (A04.7) Revise to Clostridium difficile foodborne intoxication and infection (A04.7-) No Change Helminthiases (B65-B83) No Change B81 Other intestinal helminthiases, not elsewhere classified No Change Excludes1: Revise from angiostrongyliasis due to Parastrongylus cantonensis (B83.2) Revise to angiostrongyliasis due to: Add Angiostrongylus cantonensis (B83.2) Add Parastrongylus cantonensis (B83.2) No Change B81.3 Intestinal angiostrongyliasis Revise from Angiostrongyliasis due to Parastrongylus costaricensis Revise to Angiostrongyliasis due to: Add Angiostrongylus costaricensis Add Parastrongylus costaricensis No Change Chapter 2 No Change Neoplasms (C00-D49) No Change Malignant neoplasms of ill-defined, other secondary and unspecified sites (C76-C80) No Change C79 Secondary malignant neoplasm of other and unspecified sites Delete Excludes2: lymph node metastases (C77.0) No Change C79.1 Secondary malignant neoplasm of bladder -

EFFECTIVE NEBRASKA DEPARTMENT of 01/01/2017 HEALTH and HUMAN SERVICES 173 NAC 1 I TITLE 173 COMMUNICABLE DISEASES CHAPTER 1
EFFECTIVE NEBRASKA DEPARTMENT OF 01/01/2017 HEALTH AND HUMAN SERVICES 173 NAC 1 TITLE 173 COMMUNICABLE DISEASES CHAPTER 1 REPORTING AND CONTROL OF COMMUNICABLE DISEASES TABLE OF CONTENTS SECTION SUBJECT PAGE 1-001 SCOPE AND AUTHORITY 1 1-002 DEFINITIONS 1 1-003 WHO MUST REPORT 2 1-003.01 Healthcare Providers (Physicians and Hospitals) 2 1-003.01A Reporting by PA’s and APRN’s 2 1-003.01B Reporting by Laboratories in lieu of Physicians 3 1-003.01C Reporting by Healthcare Facilities in lieu of Physicians for 3 Healthcare Associated Infections (HAIs) 1-003.02 Laboratories 3 1-003.02A Electronic Ordering of Laboratory Tests 3 1-004 REPORTABLE DISEASES, POISONINGS, AND ORGANISMS: 3 LISTS AND FREQUENCY OF REPORTS 1-004.01 Immediate Reports 4 1-004.01A List of Diseases, Poisonings, and Organisms 4 1-004.01B Clusters, Outbreaks, or Unusual Events, Including Possible 5 Bioterroristic Attacks 1-004.02 Reports Within Seven Days – List of Reportable Diseases, 5 Poisonings, and Organisms 1-004.03 Reporting of Antimicrobial Susceptibility 8 1-004.04 New or Emerging Diseases and Other Syndromes and Exposures – 8 Reporting and Submissions 1-004.04A Criteria 8 1-004.04B Surveillance Mechanism 8 1-004.05 Sexually Transmitted Diseases 9 1-004.06 Healthcare Associated Infections 9 1-005 METHODS OF REPORTING 9 1-005.01 Health Care Providers 9 1-005.01A Immediate Reports of Diseases, Poisonings, and Organisms 9 1-005.01B Immediate Reports of Clusters, Outbreaks, or Unusual Events, 9 Including Possible Bioterroristic Attacks i EFFECTIVE NEBRASKA DEPARTMENT OF -

Preventable Diseases Nick Wilson, Michael G Baker Abstract New Zealanders Can Now Reflect on and Celebrate 50 Years of Polio Elimination in This Country
THE NEW ZEALAND MEDICAL JOURNAL Journal of the New Zealand Medical Association Celebrating 50 years of polio elimination in New Zealand: but inadequate progress in eliminating other vaccine- preventable diseases Nick Wilson, Michael G Baker Abstract New Zealanders can now reflect on and celebrate 50 years of polio elimination in this country. This success was followed by eliminating two other infectious diseases, brucellosis and hydatids, and an imported potential disease vector, the southern saltmarsh mosquito. However, this country has made inadequate progress in eliminating several other vaccine-preventable diseases. These include measles, mumps, and rubella, which are priority candidates for elimination, and potentially Hib disease and rotavirus infection. To achieve such successes almost certainly requires that the country: (i) builds national leadership for elimination goals; (ii) develops detailed plans; (iii) continues recent successes in enhancing routine vaccination coverage; (iv) introduces rotavirus vaccine into the childhood immunisation schedule; and (v) strengthens surveillance and research (on such questions as the cost-effectiveness of new vaccines, measures to enhance uptake, and effective border controls to reduce the risk of disease importation). For 50 years now (since 1 April 1962), New Zealand has been free of transmission of wild-type polio virus infection. The end of this disease was particularly sudden with cases declining from 214 notifications in an outbreak in 1961 (with seven deaths) to only five cases in early 1962. 1 The end coincided with mass immunisation campaigns with the new Sabin (oral) vaccine in 1961 and 1962. The coverage in the vaccination campaign running from April to June 1962 was approximately 95% of the child population up to school leaving age. -
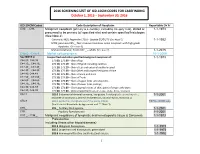
2016 SCREENING LIST of ICD-10CM CODES for CASEFINDING October 1, 2015 – September 30, 2016
2016 SCREENING LIST OF ICD-10CM CODES FOR CASEFINDING October 1, 2015 – September 30, 2016 ICD-10-CM Codes Code Description of Neoplasm Reportable Dx Yr C00._- C96._ Malignant neoplasm (primary & secondary; excluding category C44), stated or 1-1-1973 presumed to be primary (of specified site) and certain specified histologies (See Note 2) Carcinoid, NOS; Appendix C18.0 - Update 01/01/15 (See Note 5) 1-1-1992 MCN; pancreas C25._; Non-invasive mucinous cystic neoplasm with high grade dysplasia. (See note 6) Mature teratoma; Testis C62._ – adults (See note 7) 1-1-2015 C4a.0_-C4a.9_ Merkel cell carcinoma 10-1-2009 See NOTE 4 Unspecified and other specified malignant neoplasm of : 1-1-1973 C44.00.-C44.09 173.00, 173.09 – Skin of Lip C44.10_, C44.19_ 173.10, 173.19 – Skin of Eyelid including canthus C44.20_, C44.29_ 173. 20, 173.29 – Skin of Ear and external auditory canal C44.30_, C44.39_ 173.30, 173.39 – Skin Other and unspecified parts of face C44.40, C44.49 173. 40, 173.49 – Skin of Scalp and neck C44.50_, C44.59_ 173.50, 173.59 – Skin of Trunk C44.60_, C44.69_ 173. 60, 173.69 – Skin of Upper limb and shoulder, C44.70_, C44.79_ 173.70, 173.79 – Skin of Lower limb and hip; C44.80, C44.89 173.80, 173.89 – Overlapping lesions of skin, point of origin unknown; C44.90, C44.99 173.90, 173.99 - Sites unspecified (excludes Labia, Vulva, Penis, Scrotum) C54.1 182.0 Endometrial stromal sarcoma, low grade; Endolymphatic stromal myosis ; 1-1-2001 Endometrial stromatosis, Stromal endometriosis, Stromal myosis, NOS (C54.1) C56.9 183.0 Borderline malignancies -

Viability of B. Typhosus in Stored Shell Oysters
PUBLIC HEALTH REPORTS VOL. 40 APRIL 24, 1925 No. 17 VIABILITY OF B. TYPHOSUS IN STORED SHELL OYSTERS By CONRAD KINYOuN, Assistant Bacteriologist, hlygienic Laboratory, United Stztes Ptiblic Ilealti Serviee The object of this work was to determine whether oysters con- taminated with B. typhosuis and then stored unider uisual market conditions woul(l remain potentially infectious over a length of time sufficient to allow them to reach the consumer. Conflicting opinions are now current as to the length of time the causative agent of typhoid fever can remain viable in the oyster, and even as to whether the oyster can harbor the organisms at all. Obviouisly an oyster which harbors typhoidl organismns for as short a time as 24 hours becomes a potential infecting, agent for thlat time. Practi- cally it is of interest to know whether the time elapsing between the remov-al of the oyster from the bed and( actual consumption after passing through customary commercial channels is sufficient for oysters to rid themselves of possible infection. As early as 1603, oysters were incriminate(d in intestinal disor(lers, when suspicion was directed toward them by an illness of Henry IV of France (7). It was not uIntil the close of the nineteenth century, however, that oysters and shellfislh as agents of (lisease transmission receive(d particular attention. In October, 1894, Conn focused attention on the oyster by his investigation of the now famous Wesleyan outbreak, an(d thoughl only thlree outbreaks of typhoid fever were definitely traced to the oyster before 19,25, these stimulated wide interest and consequent study, with atten(lant epidemiological and bacteriological investigations. -

Disease Discovery Classification of Lymphoid Neoplasms
From www.bloodjournal.org by on December 4, 2008. For personal use only. 2008 112: 4384-4399 doi:10.1182/blood-2008-07-077982 Classification of lymphoid neoplasms: the microscope as a tool for disease discovery Elaine S. Jaffe, Nancy Lee Harris, Harald Stein and Peter G. Isaacson Updated information and services can be found at: http://bloodjournal.hematologylibrary.org/cgi/content/full/112/12/4384 Articles on similar topics may be found in the following Blood collections: Neoplasia (4200 articles) Free Research Articles (544 articles) ASH 50th Anniversary Reviews (32 articles) Clinical Trials and Observations (2473 articles) Information about reproducing this article in parts or in its entirety may be found online at: http://bloodjournal.hematologylibrary.org/misc/rights.dtl#repub_requests Information about ordering reprints may be found online at: http://bloodjournal.hematologylibrary.org/misc/rights.dtl#reprints Information about subscriptions and ASH membership may be found online at: http://bloodjournal.hematologylibrary.org/subscriptions/index.dtl Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published semimonthly by the American Society of Hematology, 1900 M St, NW, Suite 200, Washington DC 20036. Copyright 2007 by The American Society of Hematology; all rights reserved. From www.bloodjournal.org by on December 4, 2008. For personal use only. ASH 50th anniversary review Classification of lymphoid neoplasms: the microscope as a tool for disease discovery Elaine S. Jaffe,1 Nancy Lee Harris,2 Harald Stein,3 and Peter -

Characterization of a Meiotic Recombination Hotspot in Arabidopsis Thaliana Hossein Khademian
Characterization of a meiotic recombination hotspot in Arabidopsis thaliana Hossein Khademian To cite this version: Hossein Khademian. Characterization of a meiotic recombination hotspot in Arabidopsis thaliana. Agricultural sciences. Université Paris Sud - Paris XI, 2012. English. NNT : 2012PA112051. tel- 00800551 HAL Id: tel-00800551 https://tel.archives-ouvertes.fr/tel-00800551 Submitted on 14 Mar 2013 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. UNIVERSITE PARIS-SUD 11 U.F.R. Scientifique d’Orsay Thèse Présentée pour l’obtention du grade de Docteur en Sciences de l’Université Paris-Sud XI Spécialité : Sciences du Végétal par Hossein KHADEMIAN Caractérisation d’un point chaud de recombinaison méiotique chez Arabidopsis thaliana Composition du jury : Valérie BORDE Rapporteur Michel DRON Président du Jury Corinne GREY Examinateur Christine MEZARD Directeur de Thèse Minoo RASSOULZADEGAN Rapporteur Abstract Meiotic recombination initiated in prophase I of meiosis generates either crossovers (COs), which are reciprocal exchanges between chromosome segments, or gene conversion not associated to crossovers (NCOs). Both kinds of events occur in narrow regions (less than 10 kilobases) called hotspots, which are distributed non-homogenously along chromosomes. The aim of my PhD was the characterization of a hotspot of meiotic recombination (named 14a) in Arabidopsis thaliana (i) across different accessions (ii) in msh4 mutant, a gene involved in CO formation. -

Eye Disease 1 Eye Disease
Eye disease 1 Eye disease Eye disease Classification and external resources [1] MeSH D005128 This is a partial list of human eye diseases and disorders. The World Health Organisation publishes a classification of known diseases and injuries called the International Statistical Classification of Diseases and Related Health Problems or ICD-10. This list uses that classification. H00-H59 Diseases of the eye and adnexa H00-H06 Disorders of eyelid, lacrimal system and orbit • (H00.0) Hordeolum ("stye" or "sty") — a bacterial infection of sebaceous glands of eyelashes • (H00.1) Chalazion — a cyst in the eyelid (usually upper eyelid) • (H01.0) Blepharitis — inflammation of eyelids and eyelashes; characterized by white flaky skin near the eyelashes • (H02.0) Entropion and trichiasis • (H02.1) Ectropion • (H02.2) Lagophthalmos • (H02.3) Blepharochalasis • (H02.4) Ptosis • (H02.6) Xanthelasma of eyelid • (H03.0*) Parasitic infestation of eyelid in diseases classified elsewhere • Dermatitis of eyelid due to Demodex species ( B88.0+ ) • Parasitic infestation of eyelid in: • leishmaniasis ( B55.-+ ) • loiasis ( B74.3+ ) • onchocerciasis ( B73+ ) • phthiriasis ( B85.3+ ) • (H03.1*) Involvement of eyelid in other infectious diseases classified elsewhere • Involvement of eyelid in: • herpesviral (herpes simplex) infection ( B00.5+ ) • leprosy ( A30.-+ ) • molluscum contagiosum ( B08.1+ ) • tuberculosis ( A18.4+ ) • yaws ( A66.-+ ) • zoster ( B02.3+ ) • (H03.8*) Involvement of eyelid in other diseases classified elsewhere • Involvement of eyelid in impetigo -

Scientific and Medical Aspects of Apheresis: Issues and Evidence 3 ● Scientific and Medical Aspects of Apheresis: Issues and Evidence
3 Scientific and Medical Aspects of Apheresis: Issues and Evidence 3 ● Scientific and Medical Aspects of Apheresis: Issues and Evidence Various types of apheresis procedures have paucity of high-quality research, conclusions been performed on a clinical basis for many years, about the safety, efficacy, and effectiveness of but the number of patients and types of diseases apheresis are necessarily limited, although some treated have risen significantly in the last 5 years. tentative conclusions and directions for treatment This increase is partially due to increased under- can be discerned. standing of the disease and partially due to engi- The present chapter analyzes the methodolog- neering advances in equipment technologies. By ical problems in conducting apheresis research and almost any standard, treatment by apheresis is still examines available evidence of the safety, ef- in relatively early stages of development—there ficacy, and effectiveness of apheresis. Following are no ideal protocols based on a thorough un- a discussion of methodological issues, several derstanding of reasons for its efficacy. Never- major reviews of apheresis research will be sum- theless, there is an increasing flow of clinical data, marized and evaluated. This chapter will further sometimes describing dramatic patient improve- include the findings of a primary literature review ment, supporting the view that apheresis is a and assessment of apheresis in the treatment of rapidly emerging technology with significant three diseases—namely, hemolytic uremic syn- promise (117). Such evidence of treatment effec- drome, acquired Factor-VIII inhibitor, and Guil- tiveness’ is even today, however, often based on lain-Barré syndrome— where preliminary reports unsystematically collected data. -

A Retrospective Chart Review Examining the Clinical Utility of Family Health History
Sarah Lawrence College DigitalCommons@SarahLawrence The Joan H. Marks Graduate Program in Human Genetics Theses Human Genetics 5-2017 A Retrospective Chart Review Examining the Clinical Utility of Family Health History Katherine Dao Sarah Lawrence College Julia Russo Sarah Lawrence College Follow this and additional works at: https://digitalcommons.slc.edu/genetics_etd Part of the Genetics Commons Recommended Citation Dao, Katherine and Russo, Julia, "A Retrospective Chart Review Examining the Clinical Utility of Family Health History" (2017). Human Genetics Theses. 33. https://digitalcommons.slc.edu/genetics_etd/33 This Thesis - Open Access is brought to you for free and open access by the The Joan H. Marks Graduate Program in Human Genetics at DigitalCommons@SarahLawrence. It has been accepted for inclusion in Human Genetics Theses by an authorized administrator of DigitalCommons@SarahLawrence. For more information, please contact [email protected]. Katherine Dao and Julia Russo A Retrospective Chart Review Examining the Clinical Utility of Family Health History Authors: Katherine Dao, Julia Russo, Jennifer L. Garbarini, Sheila C. Johal, Shannon Wieloch Submitted in partial completion of the Master of Science Degree at Sarah Lawrence College, May 2017 1/34 Katherine Dao and Julia Russo Abstract Family health history (FHH) is a simple and cost-effective clinical tool widely used by genetic professionals. Although the value of FHH for assessing personal and familial health and reproductive risk within a prenatal population has been demonstrated in past studies, its utility within a genetic carrier screening population has not been evaluated. The purpose of this study was to examine the utility of FHH as a clinical screening tool and explore the general outcomes of full FHH evaluations within an expanded carrier screening (ECS) population.