ICD-10-CM TABULAR LIST of DISEASES and INJURIES 2018 Addenda No Change Chapter 1 No Change Certain Infectious and Parasitic Diseases (A00-B99)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ICD-10-CM Expert for SNF, IRF, and LTCH the Complete Official Code Set Codes Valid from October 1, 2018 Through September 30, 2019
EXPERT 2019 ICD-10-CM Expert for SNF, IRF, and LTCH The complete official code set Codes valid from October 1, 2018 through September 30, 2019 Power up your coding optum360coding.com ITSN_ITSN19_CVR.indd 1 12/4/17 2:54 PM Contents Preface ................................................................................ iii ICD-10-CM Index to Diseases and Injuries .......................... 1 ICD-10-CM Official Preface ........................................................................iii Characteristics of ICD-10-CM ....................................................................iii ICD-10-CM Neoplasm Table ............................................ 331 What’s New for 2019 .......................................................... iv ICD-10-CM Table of Drugs and Chemicals ...................... 349 Official Updates ............................................................................................iv Proprietary Updates ...................................................................................vii ICD-10-CM Index to External Causes ............................... 397 Introduction ....................................................................... ix ICD-10-CM Tabular List of Diseases and Injuries ............ 433 History of ICD-10-CM .................................................................................ix Chapter 1. Certain Infectious and Parasitic Diseases (A00-B99) .........................................................................433 How to Use ICD-10-CM Expert for Skilled Nursing Chapter -

Do the Lifetime Prevalence and Prognosis of Schizophrenia Differ Among World Regions? Cheryl Lynn Smith
Claremont Colleges Scholarship @ Claremont CMC Senior Theses CMC Student Scholarship 2018 Do the Lifetime Prevalence and Prognosis of Schizophrenia Differ Among World Regions? Cheryl Lynn Smith Recommended Citation Smith, Cheryl Lynn, "Do the Lifetime Prevalence and Prognosis of Schizophrenia Differ Among World Regions?" (2018). CMC Senior Theses. 1978. http://scholarship.claremont.edu/cmc_theses/1978 This Open Access Senior Thesis is brought to you by Scholarship@Claremont. It has been accepted for inclusion in this collection by an authorized administrator. For more information, please contact [email protected]. Do the Lifetime Prevalence and Prognosis of Schizophrenia Differ Among World Regions? A Thesis Presented by Cheryl Lynn Smith To the Keck Science Department Of Claremont McKenna, Pitzer, and Scripps Colleges In partial fulfillment of The degree of Bachelor of Arts Senior Thesis in Human Biology 04/23/2018 LIFETIME PREVALENCE AND PROGNOSIS OF SCHIZOPHRENIA 1 Table of Contents Abstract …………………………………………………………...……………………… 2 1. Introduction………………………………………………...…………...……………… 3 2. Background Information ……………………………...……………………………….. 5 2.1 Historical Background of Schizophrenia ……………………....…………… 5 2.2 Lifetime Prevalence of Schizophrenia …………………………...…..……… 12 2.3 Prognosis in People with Schizophrenia ……………....………...…..……… 13 3. Methods …………………………………………...……………………..……………. 17 4. Results ……………………………………………...…………………….…….…….... 18 5. Discussion ……………………………………………...……………………………… 24 6. Acknowledgements …………………………………………...………………………. -

Diseases/Symptoms Reported to Be Associated with Lyme Disease
Diseases/Symptoms Reported to be Associated with Lyme Disease Abdominal pseudo-eventration Abdominal wall weakness Acrodermatitis chronica atrophicans (ACA) Acute Acral Ischemia Acute conduction disorders Acute coronary syndrome Acute exogenous psychosis Acute febrile illness Acute hemiparesis Acute ischaemic pontine stroke Acute meningitis Acute myelo-meningo-radiculitis Acute myelitis Acute pediatric monoarticular arthritis Acute peripheral facial palsy Acute perimyocarditis Acute posterior multifocal placoid pigment epitheliopathy (APMPPE) Acute pyogenic arthritis Acute reversible diffuse conduction system disease Acute septic arthritis Acute severe encephalitis Acute transitory auriculoventricular block Acute transverse myelitis Acute urinary retention Acquired Immune Deficiency Syndrome (AIDS) Algodystrophy Allergic conditions Allergic conjunctivitis Alopecia Alzheimer’s Disease Amyotrophic lateral sclerosis (ALS - Lou Gehrig's Disease) Amyotrophy Anamnesis Anetoderma Anorexia nervosa Anterior optic neuropathy Antepartum fever Anxiety Arrhythmia Arthralgia Arthritis Asymmetrical hearing loss Ataxic sensory neuropathy Atraumatic spontaneous hemarthrosis Atrioventricular block Attention Deficit Disorder (ADD) Attention Deficit Hyperactivity Disorder (ADHD) Back pain without radiculitis Bannwarth’s Syndrome Behcet's disease Bell’s Palsy Benign cutaneous lymphocytoma Benign lymphocytic infiltration (Jessner-Kanof) Bilateral acute confluent disseminated choroiditis Bilateral carpal tunnel syndrome Bilateral facial nerve palsy Bilateral -

EFFECTIVE NEBRASKA DEPARTMENT of 01/01/2017 HEALTH and HUMAN SERVICES 173 NAC 1 I TITLE 173 COMMUNICABLE DISEASES CHAPTER 1
EFFECTIVE NEBRASKA DEPARTMENT OF 01/01/2017 HEALTH AND HUMAN SERVICES 173 NAC 1 TITLE 173 COMMUNICABLE DISEASES CHAPTER 1 REPORTING AND CONTROL OF COMMUNICABLE DISEASES TABLE OF CONTENTS SECTION SUBJECT PAGE 1-001 SCOPE AND AUTHORITY 1 1-002 DEFINITIONS 1 1-003 WHO MUST REPORT 2 1-003.01 Healthcare Providers (Physicians and Hospitals) 2 1-003.01A Reporting by PA’s and APRN’s 2 1-003.01B Reporting by Laboratories in lieu of Physicians 3 1-003.01C Reporting by Healthcare Facilities in lieu of Physicians for 3 Healthcare Associated Infections (HAIs) 1-003.02 Laboratories 3 1-003.02A Electronic Ordering of Laboratory Tests 3 1-004 REPORTABLE DISEASES, POISONINGS, AND ORGANISMS: 3 LISTS AND FREQUENCY OF REPORTS 1-004.01 Immediate Reports 4 1-004.01A List of Diseases, Poisonings, and Organisms 4 1-004.01B Clusters, Outbreaks, or Unusual Events, Including Possible 5 Bioterroristic Attacks 1-004.02 Reports Within Seven Days – List of Reportable Diseases, 5 Poisonings, and Organisms 1-004.03 Reporting of Antimicrobial Susceptibility 8 1-004.04 New or Emerging Diseases and Other Syndromes and Exposures – 8 Reporting and Submissions 1-004.04A Criteria 8 1-004.04B Surveillance Mechanism 8 1-004.05 Sexually Transmitted Diseases 9 1-004.06 Healthcare Associated Infections 9 1-005 METHODS OF REPORTING 9 1-005.01 Health Care Providers 9 1-005.01A Immediate Reports of Diseases, Poisonings, and Organisms 9 1-005.01B Immediate Reports of Clusters, Outbreaks, or Unusual Events, 9 Including Possible Bioterroristic Attacks i EFFECTIVE NEBRASKA DEPARTMENT OF -

Preventable Diseases Nick Wilson, Michael G Baker Abstract New Zealanders Can Now Reflect on and Celebrate 50 Years of Polio Elimination in This Country
THE NEW ZEALAND MEDICAL JOURNAL Journal of the New Zealand Medical Association Celebrating 50 years of polio elimination in New Zealand: but inadequate progress in eliminating other vaccine- preventable diseases Nick Wilson, Michael G Baker Abstract New Zealanders can now reflect on and celebrate 50 years of polio elimination in this country. This success was followed by eliminating two other infectious diseases, brucellosis and hydatids, and an imported potential disease vector, the southern saltmarsh mosquito. However, this country has made inadequate progress in eliminating several other vaccine-preventable diseases. These include measles, mumps, and rubella, which are priority candidates for elimination, and potentially Hib disease and rotavirus infection. To achieve such successes almost certainly requires that the country: (i) builds national leadership for elimination goals; (ii) develops detailed plans; (iii) continues recent successes in enhancing routine vaccination coverage; (iv) introduces rotavirus vaccine into the childhood immunisation schedule; and (v) strengthens surveillance and research (on such questions as the cost-effectiveness of new vaccines, measures to enhance uptake, and effective border controls to reduce the risk of disease importation). For 50 years now (since 1 April 1962), New Zealand has been free of transmission of wild-type polio virus infection. The end of this disease was particularly sudden with cases declining from 214 notifications in an outbreak in 1961 (with seven deaths) to only five cases in early 1962. 1 The end coincided with mass immunisation campaigns with the new Sabin (oral) vaccine in 1961 and 1962. The coverage in the vaccination campaign running from April to June 1962 was approximately 95% of the child population up to school leaving age. -

Hematopoietic and Lymphoid Neoplasm Coding Manual
Hematopoietic and Lymphoid Neoplasm Coding Manual Effective with Cases Diagnosed 1/1/2010 and Forward Published August 2021 Editors: Jennifer Ruhl, MSHCA, RHIT, CCS, CTR, NCI SEER Margaret (Peggy) Adamo, BS, AAS, RHIT, CTR, NCI SEER Lois Dickie, CTR, NCI SEER Serban Negoita, MD, PhD, CTR, NCI SEER Suggested citation: Ruhl J, Adamo M, Dickie L., Negoita, S. (August 2021). Hematopoietic and Lymphoid Neoplasm Coding Manual. National Cancer Institute, Bethesda, MD, 2021. Hematopoietic and Lymphoid Neoplasm Coding Manual 1 In Appreciation NCI SEER gratefully acknowledges the dedicated work of Drs, Charles Platz and Graca Dores since the inception of the Hematopoietic project. They continue to provide support. We deeply appreciate their willingness to serve as advisors for the rules within this manual. The quality of this Hematopoietic project is directly related to their commitment. NCI SEER would also like to acknowledge the following individuals who provided input on the manual and/or the database. Their contributions are greatly appreciated. • Carolyn Callaghan, CTR (SEER Seattle Registry) • Tiffany Janes, CTR (SEER Seattle Registry) We would also like to give a special thanks to the following individuals at Information Management Services, Inc. (IMS) who provide us with document support and web development. • Suzanne Adams, BS, CTR • Ginger Carter, BA • Sean Brennan, BS • Paul Stephenson, BS • Jacob Tomlinson, BS Hematopoietic and Lymphoid Neoplasm Coding Manual 2 Dedication The Hematopoietic and Lymphoid Neoplasm Coding Manual (Heme manual) and the companion Hematopoietic and Lymphoid Neoplasm Database (Heme DB) are dedicated to the hard-working cancer registrars across the world who meticulously identify, abstract, and code cancer data. -

Eye Disease 1 Eye Disease
Eye disease 1 Eye disease Eye disease Classification and external resources [1] MeSH D005128 This is a partial list of human eye diseases and disorders. The World Health Organisation publishes a classification of known diseases and injuries called the International Statistical Classification of Diseases and Related Health Problems or ICD-10. This list uses that classification. H00-H59 Diseases of the eye and adnexa H00-H06 Disorders of eyelid, lacrimal system and orbit • (H00.0) Hordeolum ("stye" or "sty") — a bacterial infection of sebaceous glands of eyelashes • (H00.1) Chalazion — a cyst in the eyelid (usually upper eyelid) • (H01.0) Blepharitis — inflammation of eyelids and eyelashes; characterized by white flaky skin near the eyelashes • (H02.0) Entropion and trichiasis • (H02.1) Ectropion • (H02.2) Lagophthalmos • (H02.3) Blepharochalasis • (H02.4) Ptosis • (H02.6) Xanthelasma of eyelid • (H03.0*) Parasitic infestation of eyelid in diseases classified elsewhere • Dermatitis of eyelid due to Demodex species ( B88.0+ ) • Parasitic infestation of eyelid in: • leishmaniasis ( B55.-+ ) • loiasis ( B74.3+ ) • onchocerciasis ( B73+ ) • phthiriasis ( B85.3+ ) • (H03.1*) Involvement of eyelid in other infectious diseases classified elsewhere • Involvement of eyelid in: • herpesviral (herpes simplex) infection ( B00.5+ ) • leprosy ( A30.-+ ) • molluscum contagiosum ( B08.1+ ) • tuberculosis ( A18.4+ ) • yaws ( A66.-+ ) • zoster ( B02.3+ ) • (H03.8*) Involvement of eyelid in other diseases classified elsewhere • Involvement of eyelid in impetigo -
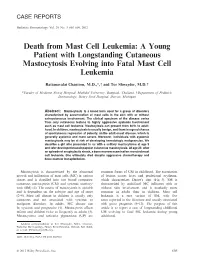
Death from Mast Cell Leukemia: a Young Patient with Longstanding Cutaneous Mastocytosis Evolving Into Fatal Mast Cell Leukemia
CASE REPORTS Pediatric Dermatology Vol. 29 No. 5 605–609, 2012 Death from Mast Cell Leukemia: A Young Patient with Longstanding Cutaneous Mastocytosis Evolving into Fatal Mast Cell Leukemia Rattanavalai Chantorn, M.D.,*, and Tor Shwayder, M.D. *Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand, Department of Pediatric Dermatology, Henry Ford Hospital, Detroit, Michigan Abstract: Mastocytosis is a broad term used for a group of disorders characterized by accumulation of mast cells in the skin with or without extracutaneous involvement. The clinical spectrum of the disease varies from only cutaneous lesions to highly aggressive systemic involvement such as mast cell leukemia. Mastocytosis can present from birth to adult- hood. In children, mastocytosis is usually benign, and there is a good chance of spontaneous regression at puberty, unlike adult-onset disease, which is generally systemic and more severe. Moreover, individuals with systemic mastocytosis may be at risk of developing hematologic malignancies. We describe a girl who presented to us with a solitary mastocytoma at age 5 and later developed maculopapular cutaneous mastocytosis. At age 23, after an episode of anaphylactic shock, a bone marrow examination revealed mast cell leukemia. She ultimately died despite aggressive chemotherapy and bone marrow transplantation. Mastocytosis is characterized by the abnormal common forms of CM in childhood. The excoriation growth and infiltration of mast cells (MC) in various of lesions causes hives and perilesional erythema, tissues and is classified into two broad categories: which characterizes Darier’s sign (Fig. 3). SM is cutaneous mastocytosis (CM) and systemic mastocy- characterized by multifocal MC infiltrates with or tosis (SM) (1). -

European Conference on Rare Diseases
EUROPEAN CONFERENCE ON RARE DISEASES Luxembourg 21-22 June 2005 EUROPEAN CONFERENCE ON RARE DISEASES Copyright 2005 © Eurordis For more information: www.eurordis.org Webcast of the conference and abstracts: www.rare-luxembourg2005.org TABLE OF CONTENT_3 ------------------------------------------------- ACKNOWLEDGEMENTS AND CREDITS A specialised clinic for Rare Diseases : the RD TABLE OF CONTENTS Outpatient’s Clinic (RDOC) in Italy …………… 48 ------------------------------------------------- ------------------------------------------------- 4 / RARE, BUT EXISTING The organisers particularly wish to thank ACKNOWLEDGEMENTS AND CREDITS 4.1 No code, no name, no existence …………… 49 ------------------------------------------------- the following persons/organisations/companies 4.2 Why do we need to code rare diseases? … 50 PROGRAMME COMMITTEE for their role : ------------------------------------------------- Members of the Programme Committee ……… 6 5 / RESEARCH AND CARE Conference Programme …………………………… 7 …… HER ROYAL HIGHNESS THE GRAND DUCHESS OF LUXEMBOURG Key features of the conference …………………… 12 5.1 Research for Rare Diseases in the EU 54 • Participants ……………………………………… 12 5.2 Fighting the fragmentation of research …… 55 A multi-disciplinary approach ………………… 55 THE EUROPEAN COMMISSION Funding of the conference ……………………… 14 Transfer of academic research towards • ------------------------------------------------- industrial development ………………………… 60 THE GOVERNEMENT OF LUXEMBOURG Speakers ……………………………………………… 16 Strengthening cooperation between academia -

Distal Myopathies a Review: Highlights on Distal Myopathies with Rimmed Vacuoles
Review Article Distal myopathies a review: Highlights on distal myopathies with rimmed vacuoles May Christine V. Malicdan, Ikuya Nonaka Department of Neuromuscular Research, National Institutes of Neurosciences, National Center of Neurology and Psychiatry, Tokyo, Japan Distal myopathies are a group of heterogeneous disorders Since the discovery of the gene loci for a number classiÞ ed into one broad category due to the presentation of distal myopathies, several diseases previously of weakness involving the distal skeletal muscles. The categorized as different disorders have now proven to recent years have witnessed increasing efforts to identify be the same or allelic disorders (e.g. distal myopathy the causative genes for distal myopathies. The identiÞ cation with rimmed vacuoles and hereditary inclusion body of few causative genes made the broad classiÞ cation of myopathy, Miyoshi myopathy and limb-girdle muscular these diseases under “distal myopathies” disputable and dystrophy type 2B (LGMD 2B). added some enigma to why distal muscles are preferentially This review will focus on the most commonly affected. Nevertheless, with the clariÞ cation of the molecular known and distinct distal myopathies, using a simple basis of speciÞ c conditions, additional clues have been classification: distal myopathies with known molecular uncovered to understand the mechanism of each condition. defects [Table 1] and distal myopathies with unknown This review will give a synopsis of the common distal causative genes [Table 2]. The identification of the myopathies, presenting salient facts regarding the clinical, genes involved in distal myopathies has broadened pathological, and molecular aspects of each disease. Distal this classification into sub-categories as to the location myopathy with rimmed vacuoles, or Nonaka myopathy, will of encoded proteins: sarcomere (titin, myosin); plasma be discussed in more detail. -

Managing Communicable Diseases in Child Care Settings
MANAGING COMMUNICABLE DISEASES IN CHILD CARE SETTINGS Prepared jointly by: Child Care Licensing Division Michigan Department of Licensing and Regulatory Affairs and Divisions of Communicable Disease & Immunization Michigan Department of Health and Human Services Ways to Keep Children and Adults Healthy It is very common for children and adults to become ill in a child care setting. There are a number of steps child care providers and staff can take to prevent or reduce the incidents of illness among children and adults in the child care setting. You can also refer to the publication Let’s Keep It Healthy – Policies and Procedures for a Safe and Healthy Environment. Hand Washing Hand washing is one of the most effective way to prevent the spread of illness. Hands should be washed frequently including after diapering, toileting, caring for an ill child, and coming into contact with bodily fluids (such as nose wiping), before feeding, eating and handling food, and at any time hands are soiled. Note: The use of disposable gloves during diapering does not eliminate the need for hand washing. The use of gloves is not required during diapering. However, if gloves are used, caregivers must still wash their hands after each diaper change. Instructions for effective hand washing are: 1. Wet hands under warm, running water. 2. Apply liquid soap. Antibacterial soap is not recommended. 3. Vigorously rub hands together for at least 20 seconds to lather all surfaces of the hands. Pay special attention to cleaning under fingernails and thumbs. 4. Thoroughly rinse hands under warm, running water. 5. -
National System for Recording and Notification of Occupational Diseases Practical Guide
InternationalInternational LabourLabour OfficeOffice GenevaGeneva National System for Recording and Notification of Occupational Diseases Practical guide Programme on Safety and Health at Work and the Environment (SafeWork) International Labour Organization Route des Morillons 4 CH -1211 Geneva 22 Switzerland TEL. + 41 22 7996715 FAX + 41 22 7996878 E-mail : safework @ ilo.org www.ilo.org / safework ILO National System for Recording and Notification of Occupational Diseases – Practical guide ISBN 978-92-2-127057-7 9 789221 270577 Programme on Safety and Health at Work and the Environment (SafeWork) National System for Recording and Notification of Occupational Diseases Practical guide International Labour Office, Geneva Copyright © International Labour Organization 2013 First published 2013 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Convention. Never- theless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to ILO Publications (Rights and Permissions), International Labour Office, CH-1211 Geneva 22, Switzerland, or by email: [email protected]. The International Labour Office welcomes such applications. Libraries, institutions and other users registered with reproduction rights organizations may make copies in accordance with the licences issued to them for this purpose. Visit www.ifrro.org to find the reproduction rights organization in your country.