Eye Disease 1 Eye Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Café Au Lait Spots As a Marker of Neuropaediatric Diseases
Mini Review Open Access J Neurol Neurosurg Volume 3 Issue 5 - May 2017 DOI: 10.19080/OAJNN.2017.03.555622 Copyright © All rights are reserved by Francisco Carratalá-Marco Café Au Lait Spots as a Marker of Neuropaediatric Diseases Francisco Carratalá-Marco1*, Rosa María Ruiz-Miralles2, Patricia Andreo-Lillo1, Julia Dolores Miralles-Botella3, Lorena Pastor-Ferrándiz1 and Mercedes Juste-Ruiz2 1Neuropaediatric Unit, University Hospital of San Juan de Alicante, Spain 2Paediatric Department, University Hospital of San Juan de Alicante, Spain 3Dermatology Department, University Hospital of San Juan de Alicante, Spain Submission: March 22, 2017; Published: May 10, 2017 *Corresponding author: Francisco Carratalá-Marco, Neuropaediatric Unit, University Hospital of San Juan de Alicante, Spain, Tel: ; Email: Abstract Introduction: want to know in which The measure,Café au lait the spots presence (CALS) of isolated are shown CALS in representsthe normal a population risk factor forwithout neurological pathological disease. significance, although they could also be criteria for some neurologic syndromes. Unspecific association with general neurologic illnesses has been less frequently described. We Patients and methods: We set up an observational transversal study of cases, patients admitted for neuropaediatric reasons (NPP; n=49) excluding all the patients suffering from neurologic illnesses associated to CALS, and controls, a hospital simultaneously admitted pediatric population for non-neurologic causes (CP; n=101) since October 2012 to January 2013. The data were collected from the clinical reports at admission, and then analyzed by SPSS 22.0 statistical package, and the Stat Calc module of EpiInfo 7.0, following the ethics current rules of the institution for observational studies. -

ICD-10-CM TABULAR LIST of DISEASES and INJURIES 2018 Addenda No Change Chapter 1 No Change Certain Infectious and Parasitic Diseases (A00-B99)
ICD-10-CM TABULAR LIST of DISEASES and INJURIES 2018 Addenda No Change Chapter 1 No Change Certain infectious and parasitic diseases (A00-B99) No Change Intestinal infectious diseases (A00-A09) No Change A04 Other bacterial intestinal infections No Change A04.7 Enterocolitis due to Clostridium difficile Add A04.71 Enterocolitis due to Clostridium difficile, recurrent Add A04.72 Enterocolitis due to Clostridium difficile, not specified as recurrent No Change A05 Other bacterial foodborne intoxications, not elsewhere classified No Change Excludes1: Revise from Clostridium difficile foodborne intoxication and infection (A04.7) Revise to Clostridium difficile foodborne intoxication and infection (A04.7-) No Change Helminthiases (B65-B83) No Change B81 Other intestinal helminthiases, not elsewhere classified No Change Excludes1: Revise from angiostrongyliasis due to Parastrongylus cantonensis (B83.2) Revise to angiostrongyliasis due to: Add Angiostrongylus cantonensis (B83.2) Add Parastrongylus cantonensis (B83.2) No Change B81.3 Intestinal angiostrongyliasis Revise from Angiostrongyliasis due to Parastrongylus costaricensis Revise to Angiostrongyliasis due to: Add Angiostrongylus costaricensis Add Parastrongylus costaricensis No Change Chapter 2 No Change Neoplasms (C00-D49) No Change Malignant neoplasms of ill-defined, other secondary and unspecified sites (C76-C80) No Change C79 Secondary malignant neoplasm of other and unspecified sites Delete Excludes2: lymph node metastases (C77.0) No Change C79.1 Secondary malignant neoplasm of bladder -

EFFECTIVE NEBRASKA DEPARTMENT of 01/01/2017 HEALTH and HUMAN SERVICES 173 NAC 1 I TITLE 173 COMMUNICABLE DISEASES CHAPTER 1
EFFECTIVE NEBRASKA DEPARTMENT OF 01/01/2017 HEALTH AND HUMAN SERVICES 173 NAC 1 TITLE 173 COMMUNICABLE DISEASES CHAPTER 1 REPORTING AND CONTROL OF COMMUNICABLE DISEASES TABLE OF CONTENTS SECTION SUBJECT PAGE 1-001 SCOPE AND AUTHORITY 1 1-002 DEFINITIONS 1 1-003 WHO MUST REPORT 2 1-003.01 Healthcare Providers (Physicians and Hospitals) 2 1-003.01A Reporting by PA’s and APRN’s 2 1-003.01B Reporting by Laboratories in lieu of Physicians 3 1-003.01C Reporting by Healthcare Facilities in lieu of Physicians for 3 Healthcare Associated Infections (HAIs) 1-003.02 Laboratories 3 1-003.02A Electronic Ordering of Laboratory Tests 3 1-004 REPORTABLE DISEASES, POISONINGS, AND ORGANISMS: 3 LISTS AND FREQUENCY OF REPORTS 1-004.01 Immediate Reports 4 1-004.01A List of Diseases, Poisonings, and Organisms 4 1-004.01B Clusters, Outbreaks, or Unusual Events, Including Possible 5 Bioterroristic Attacks 1-004.02 Reports Within Seven Days – List of Reportable Diseases, 5 Poisonings, and Organisms 1-004.03 Reporting of Antimicrobial Susceptibility 8 1-004.04 New or Emerging Diseases and Other Syndromes and Exposures – 8 Reporting and Submissions 1-004.04A Criteria 8 1-004.04B Surveillance Mechanism 8 1-004.05 Sexually Transmitted Diseases 9 1-004.06 Healthcare Associated Infections 9 1-005 METHODS OF REPORTING 9 1-005.01 Health Care Providers 9 1-005.01A Immediate Reports of Diseases, Poisonings, and Organisms 9 1-005.01B Immediate Reports of Clusters, Outbreaks, or Unusual Events, 9 Including Possible Bioterroristic Attacks i EFFECTIVE NEBRASKA DEPARTMENT OF -
RETINAL DISORDERS Eye63 (1)
RETINAL DISORDERS Eye63 (1) Retinal Disorders Last updated: May 9, 2019 CENTRAL RETINAL ARTERY OCCLUSION (CRAO) ............................................................................... 1 Pathophysiology & Ophthalmoscopy ............................................................................................... 1 Etiology ............................................................................................................................................ 2 Clinical Features ............................................................................................................................... 2 Diagnosis .......................................................................................................................................... 2 Treatment ......................................................................................................................................... 2 BRANCH RETINAL ARTERY OCCLUSION ................................................................................................ 3 CENTRAL RETINAL VEIN OCCLUSION (CRVO) ..................................................................................... 3 Pathophysiology & Etiology ............................................................................................................ 3 Clinical Features ............................................................................................................................... 3 Diagnosis ......................................................................................................................................... -
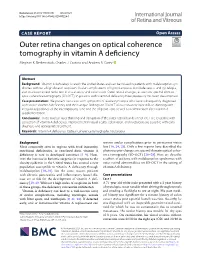
Outer Retina Changes on Optical Coherence Tomography in Vitamin a Defciency Meghan K
Berkenstock et al. Int J Retin Vitr (2020) 6:23 https://doi.org/10.1186/s40942-020-00224-1 International Journal of Retina and Vitreous CASE REPORT Open Access Outer retina changes on optical coherence tomography in vitamin A defciency Meghan K. Berkenstock, Charles J. Castoro and Andrew R. Carey* Abstract Background: Vitamin A defciency is rare in the United States and can be missed in patients with malabsorption syn- dromes without a high dose of suspicion. Ocular complications of hypovitaminosis A include xerosis and nyctalopia, and to a lesser extent reduction in visual acuity and color vision. Outer retinal changes, as seen on spectral domain optic coherence tomography (SD-OCT), in patients with vitamin A defciency have previously not been documented. Case presentation: We present two cases with symptoms of severe nyctalopia who were subsequently diagnosed with severe Vitamin A defciency and their unique fndings on SD-OCT of outer nuclear layer difuse thinning with irregular appearance of the interdigitating zone and the ellipsoid zone as well as normalization after vitamin A supplementation. Conclusions: Outer nuclear layer thinning and disruption of the outer retinal bands on SD-OCT are reversible with correction of vitamin A defciency. Improvement in visual acuity, color vision, and nyctalopia are possible with early diagnosis and appropriate treatment. Keywords: Vitamin A defciency, Optical coherence tomography, Nyctalopia Background reverse ocular complications prior to permanent vision Most commonly seen in regions with food insecurity, loss [16, 24, 25]. Only a few reports have described the nutritional defciencies, or restricted diets, vitamin A photoreceptor changes on spectral domain optical coher- defciency is rare in developed countries [1–9]. -

Special Considerations in Cataract Surgery: Five Cornea Challenges
Clinical Update EXTRA CONTENT AVAILABLE CATARACT Special Considerations in Cataract Surgery: Five Cornea Challenges by linda roach, contributing writer interviewing preston h. blomquist, md, rosa a. braga-mele, md, kimberly a. drenser, md, phd, herbert e. kaufman, md, marguerite mcdonald, md, and roger f. steinert, md s the most common surgical choices, said Marguerite McDonald, IOL Selection procedure in ophthalmol- MD, of Lynbrook, N.Y. The device en- ogy, replacement of a cloudy ables the surgeon to directly measure 1 crystalline lens with an the eye’s aphakic refractive power in intraocular lens (IOL) usu- the operating room. Aally presents the ophthalmologist with Using intraoperative aberrometry is familiar sets of surgical routines. But becoming more commonplace, as “it what about those cases that involve may help in achieving more accuracy comorbidities or other complicating with IOL power selection,” Dr. Mc- factors? Donald said. Several experts shared their per- Tips on IOL selection. The chosen spectives on approaching out-of-the- IOL should be shaped to neutralize After an off-center LASIK procedure ordinary cataract surgeries in ways spherical aberrations, said Rosa A. such as this, the irregularity of the that offer the best chance at optimiz- Braga-Mele, MD, at the University of corneal topography indicates that a ing patient outcomes. This month, Toronto. “In anybody who has had multifocal IOL should be avoided. here’s a look at five challenges involv- myopic LASIK or PRK, I think it’s very ing the cornea. important to use a negatively aspheric prior to cataract surgery. 2) A dysfunc- IOL, because these patients have more tional, unstable tear film will affect the Challenge: Prior Refractive Surgery positively aberrant corneas. -

Viability of B. Typhosus in Stored Shell Oysters
PUBLIC HEALTH REPORTS VOL. 40 APRIL 24, 1925 No. 17 VIABILITY OF B. TYPHOSUS IN STORED SHELL OYSTERS By CONRAD KINYOuN, Assistant Bacteriologist, hlygienic Laboratory, United Stztes Ptiblic Ilealti Serviee The object of this work was to determine whether oysters con- taminated with B. typhosuis and then stored unider uisual market conditions woul(l remain potentially infectious over a length of time sufficient to allow them to reach the consumer. Conflicting opinions are now current as to the length of time the causative agent of typhoid fever can remain viable in the oyster, and even as to whether the oyster can harbor the organisms at all. Obviouisly an oyster which harbors typhoidl organismns for as short a time as 24 hours becomes a potential infecting, agent for thlat time. Practi- cally it is of interest to know whether the time elapsing between the remov-al of the oyster from the bed and( actual consumption after passing through customary commercial channels is sufficient for oysters to rid themselves of possible infection. As early as 1603, oysters were incriminate(d in intestinal disor(lers, when suspicion was directed toward them by an illness of Henry IV of France (7). It was not uIntil the close of the nineteenth century, however, that oysters and shellfislh as agents of (lisease transmission receive(d particular attention. In October, 1894, Conn focused attention on the oyster by his investigation of the now famous Wesleyan outbreak, an(d thoughl only thlree outbreaks of typhoid fever were definitely traced to the oyster before 19,25, these stimulated wide interest and consequent study, with atten(lant epidemiological and bacteriological investigations. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Characterization of a Meiotic Recombination Hotspot in Arabidopsis Thaliana Hossein Khademian
Characterization of a meiotic recombination hotspot in Arabidopsis thaliana Hossein Khademian To cite this version: Hossein Khademian. Characterization of a meiotic recombination hotspot in Arabidopsis thaliana. Agricultural sciences. Université Paris Sud - Paris XI, 2012. English. NNT : 2012PA112051. tel- 00800551 HAL Id: tel-00800551 https://tel.archives-ouvertes.fr/tel-00800551 Submitted on 14 Mar 2013 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. UNIVERSITE PARIS-SUD 11 U.F.R. Scientifique d’Orsay Thèse Présentée pour l’obtention du grade de Docteur en Sciences de l’Université Paris-Sud XI Spécialité : Sciences du Végétal par Hossein KHADEMIAN Caractérisation d’un point chaud de recombinaison méiotique chez Arabidopsis thaliana Composition du jury : Valérie BORDE Rapporteur Michel DRON Président du Jury Corinne GREY Examinateur Christine MEZARD Directeur de Thèse Minoo RASSOULZADEGAN Rapporteur Abstract Meiotic recombination initiated in prophase I of meiosis generates either crossovers (COs), which are reciprocal exchanges between chromosome segments, or gene conversion not associated to crossovers (NCOs). Both kinds of events occur in narrow regions (less than 10 kilobases) called hotspots, which are distributed non-homogenously along chromosomes. The aim of my PhD was the characterization of a hotspot of meiotic recombination (named 14a) in Arabidopsis thaliana (i) across different accessions (ii) in msh4 mutant, a gene involved in CO formation. -

Changes in Ocular Rigidityin Endocrine Exophthalmos
Br J Ophthalmol: first published as 10.1136/bjo.42.11.680 on 1 November 1958. Downloaded from Brit. J. Ophthal. (1958) 42, 680. CHANGES IN OCULAR RIGIDITY IN ENDOCRINE EXOPHTHALMOS* BY R. WEEKERS AND G. LAVERGNE From the Ophthalmological Clinic, Lie'ge University Two types of endocrine exophthalmos are frequently distinguished, being referred to thyrotoxic or hyperthyroid exophthalmos, and thyrotropic, ophthahnoplegic, or oedematous exophthalmos. (a) Hyperthyroid or Thyrotoxic Exophthalmos.-This accompanies Graves's disease and is, therefore, much more frequently seen in females than in males. In the majority of cases the exophthalmos is quite unobtrusive or there is merely an appearance of exophthalmos due to retraction of the upper lid. It is associated with a decreased frequency of blinking and a fixed stare. The majority of authors agree that these symptoms should be attributed to an increase in tone of the sym- pathetic system. The importance of the pituitary thyrotropic hormone in thiscopyright. clinical picture is not clear. Hyperthyroid exophthalmos is not complicated either by chemosis or by diplopia, but heterophoria and lack of convergence are often seen. (b) Thyrotropic, Ophthalmoplegic, or Oedematous Exophthalmos.-This may occur either in a subject suffering from verified and treated hyperthyroidism, when the signs of thyrotoxicosis are about to disappear, or in an apparently normal subject free from any thyroid symptom or history of symptoms. The second type http://bjo.bmj.com/ is more frequently seen in males than in females. Thyrotropic exophthalmos is often very marked'and may even lead to irreducible lagophthalmos; it is invariably associated with a disturbance of ocular movements, particularly with elevation of the gaze. -
Connecticut Insurance Coverage for Specialized Formula; New York's “Hannah's Law”
OLR RESEARCH REPORT July 5, 2012 2012-R-0304 CONNECTICUT INSURANCE COVERAGE FOR SPECIALIZED FORMULA; NEW YORK'S “HANNAH'S LAW” By: Janet L. Kaminski Leduc, Senior Legislative Attorney You asked if Connecticut law requires health insurance policies to cover specialized formula used for treating eosinophilic disorder. You also asked for a description of New York’s “Hannah’s Law.” SUMMARY Connecticut insurance law does not explicitly require health insurance policies to cover specialized formulas for treating eosinophilic disorder. However, the law requires specified health insurance policies to cover medically necessary specialized formula for children up to age 12 for treating a disease or condition when the formula is administered under a physician’s direction. Thus, it appears that this would include coverage of specialized formulas for treating eosinophilic disorder. Anyone denied such coverage may appeal to their insurance carrier (internal appeal) or the Insurance Department (external appeal). The explanation of benefits from the carrier describes the appeal process. Anyone with concerns or questions about his or her insurance coverage may contact the Insurance Department’s Consumer Affairs Division at (800) 203-3447 or (860) 297-3900. More information about contacting the department is available at http://www.ct.gov/cid/cwp/view.asp?q=254352. Sandra Norman-Eady, Director Room 5300 Phone (860) 240-8400 Legislative Office Building FAX (860) 240-8881 Connecticut General Assembly Hartford, CT 06106-1591 http://www.cga.ct.gov/olr Office of Legislative Research [email protected] A bill (“Hannah’s Law”) in the New York Assembly would require health insurance policies to cover the cost of enteral formulas for treating eosinophilic esophagitis and related eosinophilic disorders. -

Retinitis Pigmentosa and Allied Disorders Yog Raj Sharma, P
JK SCIENCE REVIEW ARTICLE Retinitis Pigmentosa and Allied Disorders Yog Raj Sharma, P. Raja Rami Reddy, Deependra V. Singh Retinitis pigmentosa (RP) is a generic term for a group Visual field loss is insidious, progressive, peripheral of disorders characterized by hereditary diffuse usually and symmetric between two eyes (except x-linked RP bilaterally symmetrical progressive dysfunction, cell loss which can have bizarre and asymmetric patterns). In the and eventual atrophy of retina. Initially photoreceptors majority of patients the earliest defects are relative are involved and subsequently inner retina is damaged. scotomas in the periphery between 30 and 50 degrees Although both rods and cones are involved, damage to from fixation, which enlarge, deepen and coalesce to the rods is predominant. RP may be seen in isolation form a ring of visual field loss. As ring scotomas enlarge (Typical RP) or in association with systemic diseases. toward the far periphery, islands of relatively normal The reported prevalence of typical RP is approximately vision remain usually temporal but occasionally 1: 50000 worldwide. Most commonly 46% of the cases inferiorly. In typical RP the progression of visual loss is are sporadic with only one affected member in a given slow and relentless. Berson et al found that overall about family. X- linked recessive inheritance is least common, 4.6% of remaining visual field was lost per year (3). amounting to 8%. Autosomal dominant inheritance is Central visual loss found in 19% and recessive in 19%. The age of onset This can occur early in typical RP while significant and the natural history of the disease depend on the peripheral field remains cystoid macular edema, macular inheritance.