In the Prevention of Occupational Diseases 94 7.1 Introduction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Eye Disease 1 Eye Disease
Eye disease 1 Eye disease Eye disease Classification and external resources [1] MeSH D005128 This is a partial list of human eye diseases and disorders. The World Health Organisation publishes a classification of known diseases and injuries called the International Statistical Classification of Diseases and Related Health Problems or ICD-10. This list uses that classification. H00-H59 Diseases of the eye and adnexa H00-H06 Disorders of eyelid, lacrimal system and orbit • (H00.0) Hordeolum ("stye" or "sty") — a bacterial infection of sebaceous glands of eyelashes • (H00.1) Chalazion — a cyst in the eyelid (usually upper eyelid) • (H01.0) Blepharitis — inflammation of eyelids and eyelashes; characterized by white flaky skin near the eyelashes • (H02.0) Entropion and trichiasis • (H02.1) Ectropion • (H02.2) Lagophthalmos • (H02.3) Blepharochalasis • (H02.4) Ptosis • (H02.6) Xanthelasma of eyelid • (H03.0*) Parasitic infestation of eyelid in diseases classified elsewhere • Dermatitis of eyelid due to Demodex species ( B88.0+ ) • Parasitic infestation of eyelid in: • leishmaniasis ( B55.-+ ) • loiasis ( B74.3+ ) • onchocerciasis ( B73+ ) • phthiriasis ( B85.3+ ) • (H03.1*) Involvement of eyelid in other infectious diseases classified elsewhere • Involvement of eyelid in: • herpesviral (herpes simplex) infection ( B00.5+ ) • leprosy ( A30.-+ ) • molluscum contagiosum ( B08.1+ ) • tuberculosis ( A18.4+ ) • yaws ( A66.-+ ) • zoster ( B02.3+ ) • (H03.8*) Involvement of eyelid in other diseases classified elsewhere • Involvement of eyelid in impetigo -

Osteoporosis in Premenopausal Women: a Clinical Narrative Review by the ECTS and the IOF
This is a repository copy of Osteoporosis in premenopausal women: a clinical narrative review by the ECTS and the IOF. White Rose Research Online URL for this paper: https://eprints.whiterose.ac.uk/162028/ Version: Accepted Version Article: Pepe, J., Body, J.-J., Hadji, P. et al. (8 more authors) (2020) Osteoporosis in premenopausal women: a clinical narrative review by the ECTS and the IOF. The Journal of Clinical Endocrinology & Metabolism. ISSN 0021-972X https://doi.org/10.1210/clinem/dgaa306 This is a pre-copyedited, author-produced version of an article accepted for publication in Journal of Clinical Endocrinology and Metabolism following peer review. The version of record Jessica Pepe, Jean-Jacques Body, Peyman Hadji, Eugene McCloskey, Christian Meier, Barbara Obermayer-Pietsch, Andrea Palermo, Elena Tsourdi, M Carola Zillikens, Bente Langdahl, Serge Ferrari, Osteoporosis in premenopausal women: a clinical narrative review by the ECTS and the IOF, The Journal of Clinical Endocrinology & Metabolism, dgaa306 is available online at: https://doi.org/10.1210/clinem/dgaa306 Reuse Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. -
Level I Syllabus
LEVEL I SYLLABUS 1 ACDT Course Learning Objectives Upon Completion, Those Enrolled Will Be MODULE Prepared To... The Language of Dermatology 1. Define and spell the following cutaneous lesions/descriptors: a. Macule b. Patch c. Papule d. Nodule e. Cyst f. Plaque g. Wheal h. Vesicle i. Bulla j. Pustule k. Erosion l. Ulcer m. Atrophy n. Scaling o. Crusting p. Excoriations q. Fissures r. Lichenification s. Erythematous t. Violaceous u. Purpuric v. Hypo/Hyperpigmented w. Linear x. Annular y. Nummular/Discoid z. Blaschkoid aa. Morbilliform bb. Polycyclic cc. Arcuate dd. Reticular Collecting & Documenting Patient History Part I 1. Describe the importance of documentation and chart review, while properly collecting dermatologyspecific medical history components, including: a. Chief Complaint b. Past Medical History c. Family History d. Medications e. Allergies Collecting & Documenting Patient History Part II 1. Demonstrate the proper collection of dermatologyspecific medical history and explain the significance of the following: a. Social History b. Review of Systems c. History of Present Illness Anatomy 1. Spell and document the following directional indicators while applying them to the appropriate anatomical landmarks: a. Proximal/Distal b. Superior/Mid/Inferior c. Anterior/Posterior d. Medial/Lateral e. Dorsal/Ventral 2. Spell and identify specific anatomical locations involving the: a. Scalp b. Forehead c. Ears d. Eyes e. Nose f. Cheeks g. Lips h. Chin i. Neck j. Back k. Upper extremity l. Hands m. Nails n. Chest o. Abdomen p. Buttocks q. Hips r. Lower extremity s. Feet Skin Structure and Function 1. Identify and spell the three primary layers of skin: a. -

European Conference on Rare Diseases
EUROPEAN CONFERENCE ON RARE DISEASES Luxembourg 21-22 June 2005 EUROPEAN CONFERENCE ON RARE DISEASES Copyright 2005 © Eurordis For more information: www.eurordis.org Webcast of the conference and abstracts: www.rare-luxembourg2005.org TABLE OF CONTENT_3 ------------------------------------------------- ACKNOWLEDGEMENTS AND CREDITS A specialised clinic for Rare Diseases : the RD TABLE OF CONTENTS Outpatient’s Clinic (RDOC) in Italy …………… 48 ------------------------------------------------- ------------------------------------------------- 4 / RARE, BUT EXISTING The organisers particularly wish to thank ACKNOWLEDGEMENTS AND CREDITS 4.1 No code, no name, no existence …………… 49 ------------------------------------------------- the following persons/organisations/companies 4.2 Why do we need to code rare diseases? … 50 PROGRAMME COMMITTEE for their role : ------------------------------------------------- Members of the Programme Committee ……… 6 5 / RESEARCH AND CARE Conference Programme …………………………… 7 …… HER ROYAL HIGHNESS THE GRAND DUCHESS OF LUXEMBOURG Key features of the conference …………………… 12 5.1 Research for Rare Diseases in the EU 54 • Participants ……………………………………… 12 5.2 Fighting the fragmentation of research …… 55 A multi-disciplinary approach ………………… 55 THE EUROPEAN COMMISSION Funding of the conference ……………………… 14 Transfer of academic research towards • ------------------------------------------------- industrial development ………………………… 60 THE GOVERNEMENT OF LUXEMBOURG Speakers ……………………………………………… 16 Strengthening cooperation between academia -

Heberden Society
Ann Rheum Dis: first published as 10.1136/ard.25.1.86-b on 1 January 1966. Downloaded from Ann. rheum. Dis. (1966), 25, 86 HEBERDEN SOCIETY OFFICERS, 1966 Junior Hon. Secretary: Dr. J. A. Cosh President: Dr. Oswald Savage Hon. Librarian: Dr. W. S. C. Copeman President-Elect: Dr. J. J. R. Duthie PROGRAMME OF MEETINGS, 1966 March 25: Clinical Meeting, Rheumatism Research Hon. Treasurer: Wing, Birmingham. May 20: Meeting at Harrogate. Dr. F. Dudley Hart October 7: Heberden Round conducted by Dr. R. M. Mason at the London Hospital. Senior Hon. Secretary: November 18: Heberden Oration by Prof. E. G. L. Dr. C. F. Hawkins, Bywaters and Annual General Meeting at the Wellcome Rheumatism Research Wing, Foundation, London. Annual Dinner at the Royal Queen Elizabeth Hospital, Birmingham, 15 College of Physicians, Regents Park, London. by copyright. DR. HUGH CLEGG Dr. Hugh Clegg retired from the Editorship of the in 1945, soon after the war. He has always exerted an British Medical Journal at the beginning of this year and active influence and rheumatology in Great Britain owes so also from the Editorial Board of the Annals. It was him much. due to his foresight and help that our Journal was The Editor and members of the Editorial Committee adopted by the British Medical Association as one of and Board will miss his wise guidance, but wish him well their quarterly specialist journals which he inaugurated in his retirement. http://ard.bmj.com/ LIGUE INTERNATIONALE CONTRE LE RHUMATISME XI International Congress of Rheumatology, Argentina, 1965 on September 28, 2021 by guest. -
Neurodegeneration in Accelerated Aging
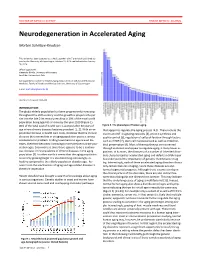
DOCTOR OF MEDICAL SCIENCE DANISH MEDICAL JOURNAL Neurodegeneration in Accelerated Aging Morten Scheibye-Knudsen This review has been accepted as a thesis together with 7 previously published pa- pers by the University of Copenhagen, October 16, 2014 and defended on January 14, 2016 Official opponents: Alexander Bürkle, University of Konstanz Lars Eide, University of Oslo Correspondence: Center for Healthy Aging, Department of Cellular and Molecular Medicine, Faculty of Health and Medical Sciences, University of Copenhagen E-mail: [email protected] Dan Med J 2016;63(11):B5308 INTRODUCTION The global elderly population has been progressively increasing throughout the 20th century and this growth is projected to per- sist into the late 21st century resulting in 20% of the total world population being aged 65 or more by the year 2100 (Figure 1). 80% of the total cost of health care is accrued after 40 years of Figure 2. The phenotype of human aging. age where chronic diseases become prevalent [1, 2]. With an ex- that appear to regulate the aging process [4,5]. These include the ponential increase in health care costs, it follows that the chronic insulin and IGF-1 signaling cascades [4], protein synthesis and diseases that accumulate in an aging population poses a serious quality control [6], regulation of cell proliferation through factors socioeconomic problem. Finding treatments to age related dis- such as mTOR [7], stem cell maintenance 8 as well as mitochon- eases, therefore becomes increasingly more pertinent as the pop- drial preservation [9]. Most of these pathways are conserved ulation ages. Even more so since there appears to be a continu- through evolution and appear to regulate aging in many lower or- ous increase in the prevalence of chronic diseases in the aging ganisms. -

Remodeling Clinical Examinations Using OWL∗
Representing Knowledge in Oral Medicine – Remodeling Clinical Examinations Using OWL∗ Technical Report HS-IKI-TR-06-009 School of Humanities and Informatics, University of Sk¨ovde Marie Gustafsson [email protected] School of Humanities and Informatics University of Sk¨ovde, Box 408, SE-541 28 Sk¨ovde, Sweden Department of Computer Science and Engineering Chalmers University of Technology, SE-412 96 G¨oteborg, Sweden Abstract This report describes the remodeling of the representation of clinical examinations in oral medicine, from the previous proprietary format used by the MedView project, to using the World Wide Web Consortium’s recommendations Web Ontology Language (OWL) and Resource Description Framework (RDF). This includes the representation of (1) ex- amination templates, (2) lists of values that can be included in individual examination records, and (3) aggregates of such values used for e.g., analyzing and visualizing data. It also includes the representation of (4) individual examination records. We describe how OWL and RDF are used to represent these different knowledge components of MedView, along with the design decisions made in the remodeling process. These design decisions are related to, among other things, whether or not to use the constructs of domain and range, appropriate naming in URIs, the level of detail to initially aim for, and appropriate use of classes and individuals. A description of how these new representations are used in the previous applications and code base is also given, as well as their use in the Swedish Oral Medicine Web (SOMWeb) online community. We found that OWL and RDF can be used to address most, but not all, of the requirements we compiled based on the limitations of the MedView knowledge model. -

Managing Communicable Diseases in Child Care Settings
MANAGING COMMUNICABLE DISEASES IN CHILD CARE SETTINGS Prepared jointly by: Child Care Licensing Division Michigan Department of Licensing and Regulatory Affairs and Divisions of Communicable Disease & Immunization Michigan Department of Health and Human Services Ways to Keep Children and Adults Healthy It is very common for children and adults to become ill in a child care setting. There are a number of steps child care providers and staff can take to prevent or reduce the incidents of illness among children and adults in the child care setting. You can also refer to the publication Let’s Keep It Healthy – Policies and Procedures for a Safe and Healthy Environment. Hand Washing Hand washing is one of the most effective way to prevent the spread of illness. Hands should be washed frequently including after diapering, toileting, caring for an ill child, and coming into contact with bodily fluids (such as nose wiping), before feeding, eating and handling food, and at any time hands are soiled. Note: The use of disposable gloves during diapering does not eliminate the need for hand washing. The use of gloves is not required during diapering. However, if gloves are used, caregivers must still wash their hands after each diaper change. Instructions for effective hand washing are: 1. Wet hands under warm, running water. 2. Apply liquid soap. Antibacterial soap is not recommended. 3. Vigorously rub hands together for at least 20 seconds to lather all surfaces of the hands. Pay special attention to cleaning under fingernails and thumbs. 4. Thoroughly rinse hands under warm, running water. 5. -
National System for Recording and Notification of Occupational Diseases Practical Guide
InternationalInternational LabourLabour OfficeOffice GenevaGeneva National System for Recording and Notification of Occupational Diseases Practical guide Programme on Safety and Health at Work and the Environment (SafeWork) International Labour Organization Route des Morillons 4 CH -1211 Geneva 22 Switzerland TEL. + 41 22 7996715 FAX + 41 22 7996878 E-mail : safework @ ilo.org www.ilo.org / safework ILO National System for Recording and Notification of Occupational Diseases – Practical guide ISBN 978-92-2-127057-7 9 789221 270577 Programme on Safety and Health at Work and the Environment (SafeWork) National System for Recording and Notification of Occupational Diseases Practical guide International Labour Office, Geneva Copyright © International Labour Organization 2013 First published 2013 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Convention. Never- theless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to ILO Publications (Rights and Permissions), International Labour Office, CH-1211 Geneva 22, Switzerland, or by email: [email protected]. The International Labour Office welcomes such applications. Libraries, institutions and other users registered with reproduction rights organizations may make copies in accordance with the licences issued to them for this purpose. Visit www.ifrro.org to find the reproduction rights organization in your country. -

Regulations for Disease Reporting and Control
Department of Health Regulations for Disease Reporting and Control Commonwealth of Virginia State Board of Health October 2016 Virginia Department of Health Office of Epidemiology 109 Governor Street P.O. Box 2448 Richmond, VA 23218 Department of Health Department of Health TABLE OF CONTENTS Part I. DEFINITIONS ......................................................................................................................... 1 12 VAC 5-90-10. Definitions ............................................................................................. 1 Part II. GENERAL INFORMATION ............................................................................................... 8 12 VAC 5-90-20. Authority ............................................................................................... 8 12 VAC 5-90-30. Purpose .................................................................................................. 8 12 VAC 5-90-40. Administration ....................................................................................... 8 12 VAC 5-90-70. Powers and Procedures of Chapter Not Exclusive ................................ 9 Part III. REPORTING OF DISEASE ............................................................................................. 10 12 VAC 5-90-80. Reportable Disease List ....................................................................... 10 A. Reportable disease list ......................................................................................... 10 B. Conditions reportable by directors of -

ICD-10 Will Allow Dermatologists to Effectively Communicate with Payors About Patient Visits
ICD-10 UpDate ICD-10 Will Allow Dermatologists to Effectively Communicate With Payors About Patient Visits Angela J. Lamb, MD Practice Points With International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), derma- tologists will have a more accurate way to communicate with the pacopyyor. For example, physicians will be able to code for scabies as well as the cause of postscabetic pruritus. Physicians will have the option of coding for the reason the patient presented. For example, dermatolo- gists may code for a skin examination to screen for a malignant neoplasm. The reimbursement of the new codes has not been addressed; a head-to-head comparison will be needed during the testing period. not Do t is important that dermatologists do not over- The ICD-9 code 133.0 applies to scabies, and if we look the changes associated with the transition would like to code for the itch, we must enter a sec- Ito International Classification of Diseases, Tenth ond code for unspecified pruritic disorder (698.9).2 Revision, Clinical Modification (ICD-10-CM). Some With ICD-10-CM, we can be more specific and physicians believe that providing this level of speci- actually code for the cause of the itch. We will be ficity is not important because at the end of the day, able to mark the initial visit as B86 (scabies), but who is watching? You willCUTIS see with several of the subsequent visits for the itch related to scabies can codes highlighted in this column that specificity be coded as pruritus using the primary code L29.8 may be required before a claim can be submitted (other pruritus) and a new sequelae or late effect to the payor for processing. -

LIST of OCCUPATIONAL DISEASES (Revised 2010)
LIST OF OCCUPATIONAL DISEASES (revised 2010) Identification and recognition of occupational diseases: Criteria for incorporating diseases in the ILO list of occupational diseases Occupational Safety and Health Series, No. 74 List of occupational diseases (revised 2010) Identification and recognition of occupational diseases: Criteria for incorporating diseases in the ILO list of occupational diseases INTERNATIONAL LABOUR OFFICE • GENEVA Copyright © International Labour Organization 2010 First published 2010 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Convention. Nevertheless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to ILO Publications (Rights and Permissions), International Labour Office, CH-1211 Geneva 22, Switzerland, or by email: pubdroit@ ilo.org. The International Labour Office welcomes such applications. Libraries, institutions and other users registered with reproduction rights organizations may make copies in accordance with the licences issued to them for this purpose. Visit www.ifrro.org to find the reproduction rights organization in your country. ILO List of occupational diseases (revised 2010). Identification and recognition of occupational diseases: Criteria for incorporating diseases in the ILO list of occupational diseases Geneva, International Labour Office, 2010 (Occupational Safety and Health Series, No. 74) occupational disease / definition. 13.04.3 ISBN 978-92-2-123795-2 ISSN 0078-3129 Also available in French: Liste des maladies professionnelles (révisée en 2010): Identification et reconnaissance des maladies professionnelles: critères pour incorporer des maladies dans la liste des maladies professionnelles de l’OIT (ISBN 978-92-2-223795-1, ISSN 0250-412x), Geneva, 2010, and in Spanish: Lista de enfermedades profesionales (revisada en 2010).