Gender at the Core: Results-Based Financing For
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mashonaland Central Province Zimbabwe Vulnerability Assessment Committee (Zimvac) 2020 Rural Livelihoods Assessment Report Foreword
Mashonaland Central Province Zimbabwe Vulnerability Assessment Committee (ZimVAC) 2020 Rural Livelihoods Assessment Report Foreword The Zimbabwe Vulnerability Assessment Committee (ZimVAC) under the coordination of the Food and Nutrition Council, successfully undertook the 2020 Rural Livelihoods Assessment (RLA), the 20th since its inception. ZimVAC is a technical advisory committee comprised of representatives from Government, Development Partners, UN, NGOs, Technical Agencies and the Academia. In its endeavour to ‘promote and ensure adequate food and nutrition security for all people at all times’, the Government of Zimbabwe has continued to exhibit its commitment for reducing food and nutrition insecurity, poverty and improving livelihoods amongst the vulnerable populations in Zimbabwe through operationalization of Commitment 6 of the Food and Nutrition Security Policy (FNSP). As the country is grappling with the COVID-19 pandemic, this assessment was undertaken at an opportune time as there was an increasing need to urgently collect up to date food and nutrition security data to effectively support the planning and implementation of actions in a timely and responsive manner. The findings from the RLA will also go a long way in providing local insights into the full impact of the Corona virus on food and nutrition security in this country as the spread of the virus continues to evolve differently by continent and by country. In addition, the data will be of great use to Government, development partners, programme planners and communities in the recovery from the pandemic, providing timely information and helping monitor, prepare for, and respond to COVID-19 and any similar future pandemics. Thematic areas covered in this report include the following: education, food and income sources, income levels, expenditure patterns and food security, COVID-19 and gender based violence, among other issues. -

PLAAS RR46 Smeadzim 1.Pdf
Chrispen Sukume, Blasio Mavedzenge, Felix Murimbarima and Ian Scoones Faculty of Economic and Management Sciences Research Report 46 Space, Markets and Employment in Agricultural Development: Zimbabwe Country Report Chrispen Sukume, Blasio Mavedzenge, Felix Murimbarima and Ian Scoones Published by the Institute for Poverty, Land and Agrarian Studies, Faculty of Economic and Management Sciences, University of the Western Cape, Private Bag X17, Bellville 7535, Cape Town, South Africa Tel: +27 21 959 3733 Fax: +27 21 959 3732 Email: [email protected] Institute for Poverty, Land and Agrarian Studies Research Report no. 46 June 2015 All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means without prior permission from the publisher or the authors. Copy Editor: Vaun Cornell Series Editor: Rebecca Pointer Photographs: Pamela Ngwenya Typeset in Frutiger Thanks to the UK’s Department for International Development (DfID) and the Economic and Social Research Council’s (ESRC) Growth Research Programme Contents List of tables ................................................................................................................ ii List of figures .............................................................................................................. iii Acronyms and abbreviations ...................................................................................... v 1 Introduction ........................................................................................................ -
Covid-19 Addendum
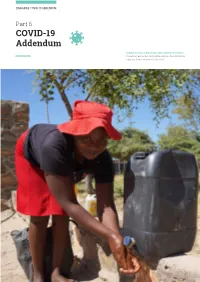
ZIMBABWE COVID-19 ADDENDUM Part 6 COVID-19 Addendum SHAMVA DISTRICT, MASHONALAND CENTRAL PROVINCE A beneficiary washes her hands before entering a food distribution in Shamva district. Photo:WFP/Claire Nevill 46 ZIMBABWE COVID-19 ADDENDUM COVID-19 Response at a Glance PEOPLE IN NEED PEOPLE TARGETED REQUIREMENTS (US$) OPERATIONAL PARTNERS 7.5M 5.9M $84.9M 37 People in Need and Targeted Requirements by Cluster H M Me Hurungwe Cy/ Mabani M F S M U Dwin Rushinga MASHONALAND CENTRAL Karoi M Guruve Mwi M Shamva M AIBA Kariba Zvimba B Pfungwe Cyi U M Mowe MASHONALAND EAST Education Ba Moko Nth MASHONALAND WEST Nton Goromonzi HARARE Mehwa B South Sanyati C Water S U Nanga V Monder M Kadoma M Town Seke U U C H WASH U MIDLANDS Mondera MANICALAND M-N Hdweza Rusape M Lupane Kwekwe MATEBELELAND NORTH K Nyi C N U M Hwange Redcliff M U C Ba urban Gutu Me Tsholotsho B Gweru U U P BV Byo C M MASVINGO I B C M Zvishavane U B Zvishavane U Z U U M C Potection Plumtree Mengwa MATEBELELAND SOUTH 2M C C Potection U U M Mobo M Gwanda Cedzi B SM M Propor IN Targeted B P geted U R 02M People in Need and Targeted by Cluster Operational Partners by Type Water S M H WASH 2M F S 0M M NNO Education M 9 M INO H M 18 0M PBV 2M 845K PP 22M UN 22 0 MS 20M 20 0M N 353K 2 S 91K In addition to the humanitarian response requirements, R 14K $4.5 million is needed to support Governance interventions 14K dination and $22.5 million for social protection, which will be 953 M 953 carried out by development actors. -

Fast Track Land Reform in Matepatepa Commercial Farming Area, Bindura District: Effects on Farm Workers, 2000 – 2010
Fast Track Land Reform in Matepatepa Commercial Farming Area, Bindura District: Effects on Farm Workers, 2000 – 2010. By Joyline Takudzwa Kufandirori THIS THESIS HAS BEEN SUBMITTED IN ACCORDANCE WITH THE REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS IN THE FACULTY OF THE HUMANITIES, FOR THE CENTRE OF AFRICA STUDIES AT THE UNIVERSITY OF THE FREE STATE. NOVEMBER 2015 SUPERVISOR: PROF. I. R. PHIMISTER CO-SUPERVISOR: DR. R. PILOSSOF Declaration I, Joyline Takudzwa Kufandirori declare that the Master’s research dissertation that I herewith submit for the Master’s Degree qualification, Arts at the University of the Free State is my own independent work, and that I have not previously submitted it for a qualification at another institution of higher learning. I, Joyline Takudzwa Kufandirori , hereby declare that I am aware that the copyright is vested in the University of the Free State. I, Joyline Takudzwa Kufandirori, hereby declare that all royalties as regards intellectual property that was developed during the course of and/ or in connection with the study at the University of the Free State, will accrue to the University. ……………………… ……………………… Joyline Takudzwa Kufandirori Bloemfontein 1 Table of Contents Abstract……………………………………………………………………………………………………………………………….i Acknowledgements..................................................................................................................iii Dedication …………………………………………………………………………………………………………………….……iv Acronyms……………………………………………………………………………………………………………………………iv Chapter One: Introduction and -

DCA in Zimbabwe
Zimbabwe OPERATIONAL CONTEXT AND KEY RESULTS: DanChurchAid is working in Zimbabwe, a country facing the serious negative impact of climate change, protracted economic and political crisis. In response to the operational context DCA works with local implementing local partners to achieve the following: Resilience building, supporting 48.000 households translating to approximately 240.000 individuals Climate change related disaster response including drought and cyclones 240 000 individuals Interventions to address Food Insecurity facing 29.000 individuals. These include cash transfers to improve food purchasing power in peri-urban settings such as Epworth near Harare DCA works with partners in supporting smallholder farmers to enhance food and income security, reaching a total of 48 000 households FACTS: In 2019 DCA in coordination with other agencies fed 5 million people facing ● DCA operated in Zimbabwe from the early to the late 1980s providing food shortages in both rural and urban settings support to refugees following the war of independence. In 2014, DCA reopened its offices to respond to the worsening economic and DCA is working with churches to promote social cohesion humanitarian situation in the country. through peace building initiatives ● Offices in country: The country office is in Harare, with a field office located in Bulawayo. WHAT WE DO: ● Beneficiaries in 2019: 240 000 individuals In Zimbabwe DCA focuses primarily on three programmatic areas namely; ● Turnover in 2019: EUR 5,973,687 ● Projects: 9 Right to Food: DCA supports smallholder farmer households to improve production and productivity while ● Employees: 58 mainstreaming resilience building, value chain development, climate change adaptation and mitigation. ● Partners: Future of Hope Foundation, Pro Africa, Institute for Rural Technologies (IRT), Organisation of Rural Associations for Progress Humanitarian Work: In Zimbabwe, DCA supports individuals affected by disasters including drought, flooding and (ORAP), ProAfrica, CCBICA, Midlands State University. -

Ufahamu: a Journal of African Studies
UCLA Ufahamu: A Journal of African Studies Title Armed Struggle in Zimbabwe: A Brief Chronology of Guerrilla Warfare 1966-74 Permalink https://escholarship.org/uc/item/3bx8v176 Journal Ufahamu: A Journal of African Studies, 5(3) ISSN 0041-5715 Author Waldman, Selma Publication Date 1975 DOI 10.5070/F753017489 Peer reviewed eScholarship.org Powered by the California Digital Library University of California - 4 - AMn SJJWiE IN Zlf13.4&E: A BRIEF CHRONOLOGY OF GUERRILLA WARFARE, 1966-1974 by SELMA WALDMAN I. 1966 Apri 1: First action of armed struggle, near town of Sinoia (90 miles northwest of Salisbury and 60 miles south of Zambia). Combatants of the Zimbabwe African National Union (ZANLA) engage in an intense skirmish against a larger number of enemy forces . 25 enemy forces killed or injured. Subsequent to beginning of guerrilla warfare, the Zimbabwe African People's Union (ZAPU) had launched sabotage campaigns (1963-4). May: "Sinoia Band" strikes again, after other clashes, in Hartley area 300 miles inland, almost in center of country. Aug. -Sept. : Makuti-Sinoia area, ZANLA clashes with enemy. Sept. -Dec. : Clashes elsewhere in the north and northeast, by ZANLA combatants. Mid-1966: ZAPU Campaign begins. ZAPU force engages enemy in open combat for the first time. Carries missions around Lupane and Urungwe areas of northern Zimbabwe (Gomoza area near Lupane) . Some victories, but many set-backs and losses: militants not properly equipped or politically and militarily prepared; in contrast, Rhodesian Security forces use modern equipment and have established a fairly good intelligence network. II. 1967-71 Mid-1967: ZANLA clashes at Feria, Rukomeshi River, Karoi, Nharine Hill. -
IRS Technical Report Template
ZIMBABWE ASSISTANCE PROGRAM IN MALARIA ANNUAL REPORT REPORTING PERIOD: OCT 1, 2017 – SEPT 30, 2018 SUBMISSION DATE: OCTOBER 30, 2018 Recommended Citation: ZAPIM Year Three Annual Report, October 1, 2017–September 30, 2018. Rockville, MD, U.S., and Harare, Zimbabwe. Zimbabwe Assistance Program in Malaria, Abt Associates. Contract and Task Order Number: AID-613-A-15-00010 Submitted to: United States Agency for International Development/President’s Malaria Initiative Submitted on: October 30, 2018 Abt Associates Inc. 1 6130 Executive Boulevard 1 1 Rockville, Maryland 20852 1 T. 301.347.5000 1 F. 301.913.9061 1 www.abtassociates.com Contents LIST OF FIGURES ...................................................................................................................... iii LIST OF TABLES ........................................................................................................................ iv ABBREVIATIONS AND ACRONYMS ............................................................................................ vi 1. Executive Summary ........................................................................................................ 1 2. Background .................................................................................................................... 1 3. Technical Activities ......................................................................................................... 3 3.1 Clinical Case Management ...................................................................................................3 -

Zimbabwe; Annual Appeal 2005; Appeal No
ZIMBAMBWE: ASSISTANCE TO THE 16 February 2006 POPULATION AFFECTED BY THE ‘CLEAN-UP’ EXERCISE The Federation’s mission is to improve the lives of vulnerable people by mobilizing the power of humanity. It is the world’s largest humanitarian organization and its millions of volunteers are active in over 183 countries. In Brief Appeal No. 05EA016; Operations Update no. 4; Period covered: 5 December 2005 to 12 January 2006; Appeal coverage: 35%. Click here to go directly to the attached Contributions List or here for the one on the website Appeal history: · Launched on 26 July 2005 for CHF 2,481,818 (USD 1,788,110 or EUR 1,487,813) for 5 months to assist 15,000 persons (3,000 households). Refer to http://www.ifrc.org/cgi/pdf_appeals.pl?05/05EA016.pdf. · Operations Update no. 1 http://www.ifrc.org/cgi/pdf_appeals.pl?05/05EA01601.pdf was released on 31 August 2005. · Operations Update no. 2 http://www.ifrc.org/cgi/pdf_appeals.pl?05/05EA01602.pdf was posted on 18 October 2005. · Operations Update no. 3 http://www.ifrc.org/cgi/pdf_appeals.pl?05/05EA01603.pdf was issued on 5 December 2005 and provided a revised plan of action for the period October-December 2005, in light of funding received. It also sought to extend the operation’s timeframe to 30 March 2006. · This Operations Update confirms the extension of the appeal timeframe to 30 March 2006. · Disaster Relief Emergency Funds (DREF) allocated: CHF 100,000. Outstanding needs: CHF 1,613,096 (USD 1,254,839 or EUR 1,037,727) Related Emergency or Annual Appeals: Zimbabwe; Annual Appeal 2005; Appeal no. -

Youth Violence in Bindura Urban, Zimbabwe
American International Journal of Contemporary Research Vol. 2 No. 6; June 2012 Political Intolerance, Diversity and Democracy: Youth Violence in Bindura Urban, Zimbabwe Obediah Dodo Lecturer Bindura University of Science Education (BUSE) P. Bag 1020 Bindura, Zimbabwe & Collen Musorowegomo Peace and Governance Masters‟ Student at BUSE Abstract Following political violence that was witnessed in Bindura constituency urban area during election periods between 1999 and 2011, a research was conducted to assess and evaluate the level of youth participation in the violence. The research, guided by the Culture of Violence theory by Wolfgang and Ferracuti and the Youth Bulge theory by Gunnar Heinsohn, sampled 243 respondents from various stakeholders. The research was conducted between August 2011 and January 2012. After a critical analysis and evaluation of all the information, the research did establish that indeed, the youth played some role in all the violence over the period. The research also noted that to some extent, youth participation was due to idleness, poverty and adult influence. (117) Key words: Youth, Democracy, Violence, Tolerance, Diversity. Introduction Zimbabwe attained its independence through a protracted liberation struggle that claimed thousands of lives. Ever since the independence in 1980, the country has had timely elections that have however been characterised by violence and bloodshed. In all these cases of violence and bloodshed, on the front line were the youth who have been described as vanguards of their political parties. It is therefore the intention of this paper to critically evaluate the role that these youth have played in Zimbabwe‟s violence with particular focus on the Bindura urban constituency between 1999 and 2011. -

Food Insecurity
Emergency appeal Zimbabwe: Food Insecurity Emergency appeal n° MDRZW006 19 December 2012 This Emergency Appeal seeks CHF 1,290,342 in cash, kind, or services to support the Zimbabwe Red Cross Society (ZRCS) to assist 10,000 beneficiaries for 9 months, and will be completed by September 2013. A Final Report will be made available by December 2013 (three months after the end of the operation). CHF 120,000 has been allocated from the International Federation of Red Cross and Red Crescent (IFRC) Disaster Relief Emergency Fund (DREF) to support this operation. Unearmarked funds to replenish DREF are encouraged. Failure of seasonal rainfall has resulted in increased food insecurity This Emergency Appeal seeks to support the and lack of safe water for both people and livestock/ZRCS photo National Society to assist vulnerable people in Zimbabwe who are food insecure as a result of a drought that affected the country in the 2011/2012 main agricultural season. The situation requires timely support of food aid and rehabilitation of water points to reduce the adverse effects of reduced nutritional intake, reinforce coping mechanisms, and increase coverage and access to clean and safe water in the form of sanitation and hygiene promotion activities. The planned intervention also includes agricultural inputs for small-scale gardening, combined with the provision of agricultural tools and training. Summary: The declared acute food insecurity crisis in Zimbabwe is now reaching its peak period with an anticipated 1.6 million people in need of food assistance. Despite interventions from the authorities and the international community, gaps still remain and many families in need have still not been assisted. -

Waniwa Ropafadzo B1335810
BINDURA UNIVERSITY OF SCIENCE EDUCATION FACULTY OF SOCIAL SCIENCE AND HUMANITIES DEPARTMENT OF PEACE AND GOVERNANCE STRUCTURAL VIOLENCE THROUGH EARLY CHILD MARRIAGES: A CASE OF MASHONALAND CENTRAL PROVINCE, BINDURA DISTRICT BY: WANIWA ROPAFADZO B1335810 SUPERVISOR: DR MUCHEMWA A DISSERTATION SUBMITTED IN PARTIAL FUFILMENT OF THE REQUIREMENTS OF THE BACHELOR OF SCIENCE HONOURS DEGREE IN PEACE AND GOVERNANCE 1 | Page RELEASE FORM Author: WANIWA ROPAFADZO Project title: STRUCTURAL VIOLENCE THROUGH EARLY CHILD MARRIAGES: A CASE OF MASHONALAND CENTRAL PROVINCE, BINDURA DISTRICT Programme: BACHELOR OF SCIENCE HONOURS DEGREE IN PEACE AND GOVERNANCE Declaration: I declare that the information contained in this project is the researcher’s original work and permission is granted to Bindura University of Science Education to produce copies without the written consent of the student Signed ……………………………………….. Permanent address: 4232, 162 Street, Warren Park D, Harare Date: …………………………………………. i | Page APPROVAL FORM TO BE COMPLETED BY PROJECT SUPERVISOR As the supervisor for………………………………………..., I declare that this dissertation has been checked for conformity with the faculty guidelines. Supervisor: DR MUCHEMWA Signature of supervisor …………………………. Date: …………………………. TO BE COMPLETED BY THE CHAIRPERSON OF DEPARTMENT I certify to the best of my knowledge that the required procedures have been followed and the preparation criteria has been met for this dissertation. Signature of chairperson: ……………………………… Date: ………………………………. ii | Page DECLARATION FORM I, WANIWA ROPAFADZO, declare that this research study is my original work and has not been copied or extracted from any previous source without due acknowledgement of the source. Signed: …………………………….. Date: ……………………………… iii | Page DEDICATION This dissertation is dedicated to my family, my father Febion, my mother Esinath, my sister Anesu and my brother Takudzwa Waniwa and my friend Tendai Tanya Chikasha. -

Zimbabwe's Irrigation Potential
USAID STRATEGIC ECONOMIC RESEARCH AND ANALYSIS – ZIMBABWE (SERA) PROGRAM ZIMBABWE’S IRRIGATION POTENTIAL: MANAGEMENT MODELS FOR IRRIGATION SCHEMES AND A POLICY FRAMEWORK FOR EFFICIENT IRRIGATED AGRICULTURE CONTRACT NO. AID-613-C-11-00001 SEPTEMBER 2016 This report was produced by Nathan Associates Inc. for review by the United States Agency for International Development (USAID). i USAID STRATEGIC ECONOMIC RESEARCH AND ANALYSIS – ZIMBABWE (SERA) PROGRAM ZIMBABWE’S IRRIGATION POTENTIAL: MANAGEMENT MODELS FOR IRRIGATION SCHEMES AND A POLICY FRAMEWORK FOR EFFICIENT IRRIGATED AGRICULTURE CONTRACT NO. AID-613-C-11-00001 Program Title: USAID Strategic Economic Research & Analysis – Zimbabwe (SERA) Sponsoring USAID Office: USAID/Zimbabwe Contract Number: AID-613-C-11-00001 Contractor: Nathan Associates Inc. Date of Publication: September 2016 Author: Oniward Svubure DISCLAIMER This document is made possible by the support of the American people through USAID. Its contents are the sole responsibility of the author or authors and do not necessarily reflect the views of USAID or the United States government. ii Contents LIST OF TABLES AND FIGURES .................................................................................................................. v ACRONYMS .............................................................................................................................................. vi EXECUTIVE SUMMARY ..........................................................................................................................