New Opportunities for Targeting the Androgen Receptor in Prostate Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Androgen Receptor Interacting Proteins and Coregulators Table
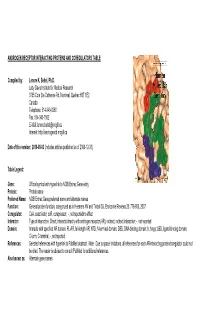
ANDROGEN RECEPTOR INTERACTING PROTEINS AND COREGULATORS TABLE Compiled by: Lenore K. Beitel, Ph.D. Lady Davis Institute for Medical Research 3755 Cote Ste Catherine Rd, Montreal, Quebec H3T 1E2 Canada Telephone: 514-340-8260 Fax: 514-340-7502 E-Mail: [email protected] Internet: http://androgendb.mcgill.ca Date of this version: 2010-08-03 (includes articles published as of 2009-12-31) Table Legend: Gene: Official symbol with hyperlink to NCBI Entrez Gene entry Protein: Protein name Preferred Name: NCBI Entrez Gene preferred name and alternate names Function: General protein function, categorized as in Heemers HV and Tindall DJ. Endocrine Reviews 28: 778-808, 2007. Coregulator: CoA, coactivator; coR, corepressor; -, not reported/no effect Interactn: Type of interaction. Direct, interacts directly with androgen receptor (AR); indirect, indirect interaction; -, not reported Domain: Interacts with specified AR domain. FL-AR, full-length AR; NTD, N-terminal domain; DBD, DNA-binding domain; h, hinge; LBD, ligand-binding domain; C-term, C-terminal; -, not reported References: Selected references with hyperlink to PubMed abstract. Note: Due to space limitations, all references for each AR-interacting protein/coregulator could not be cited. The reader is advised to consult PubMed for additional references. Also known as: Alternate gene names Gene Protein Preferred Name Function Coregulator Interactn Domain References Also known as AATF AATF/Che-1 apoptosis cell cycle coA direct FL-AR Leister P et al. Signal Transduction 3:17-25, 2003 DED; CHE1; antagonizing regulator Burgdorf S et al. J Biol Chem 279:17524-17534, 2004 CHE-1; AATF transcription factor ACTB actin, beta actin, cytoplasmic 1; cytoskeletal coA - - Ting HJ et al. -

1 Supporting Information for a Microrna Network Regulates
Supporting Information for A microRNA Network Regulates Expression and Biosynthesis of CFTR and CFTR-ΔF508 Shyam Ramachandrana,b, Philip H. Karpc, Peng Jiangc, Lynda S. Ostedgaardc, Amy E. Walza, John T. Fishere, Shaf Keshavjeeh, Kim A. Lennoxi, Ashley M. Jacobii, Scott D. Rosei, Mark A. Behlkei, Michael J. Welshb,c,d,g, Yi Xingb,c,f, Paul B. McCray Jr.a,b,c Author Affiliations: Department of Pediatricsa, Interdisciplinary Program in Geneticsb, Departments of Internal Medicinec, Molecular Physiology and Biophysicsd, Anatomy and Cell Biologye, Biomedical Engineeringf, Howard Hughes Medical Instituteg, Carver College of Medicine, University of Iowa, Iowa City, IA-52242 Division of Thoracic Surgeryh, Toronto General Hospital, University Health Network, University of Toronto, Toronto, Canada-M5G 2C4 Integrated DNA Technologiesi, Coralville, IA-52241 To whom correspondence should be addressed: Email: [email protected] (M.J.W.); yi- [email protected] (Y.X.); Email: [email protected] (P.B.M.) This PDF file includes: Materials and Methods References Fig. S1. miR-138 regulates SIN3A in a dose-dependent and site-specific manner. Fig. S2. miR-138 regulates endogenous SIN3A protein expression. Fig. S3. miR-138 regulates endogenous CFTR protein expression in Calu-3 cells. Fig. S4. miR-138 regulates endogenous CFTR protein expression in primary human airway epithelia. Fig. S5. miR-138 regulates CFTR expression in HeLa cells. Fig. S6. miR-138 regulates CFTR expression in HEK293T cells. Fig. S7. HeLa cells exhibit CFTR channel activity. Fig. S8. miR-138 improves CFTR processing. Fig. S9. miR-138 improves CFTR-ΔF508 processing. Fig. S10. SIN3A inhibition yields partial rescue of Cl- transport in CF epithelia. -

Aberrant Activity of Histone–Lysine N-Methyltransferase 2 (KMT2) Complexes in Oncogenesis
International Journal of Molecular Sciences Review Aberrant Activity of Histone–Lysine N-Methyltransferase 2 (KMT2) Complexes in Oncogenesis Elzbieta Poreba 1,* , Krzysztof Lesniewicz 2 and Julia Durzynska 1,* 1 Institute of Experimental Biology, Faculty of Biology, Adam Mickiewicz University, ul. Uniwersytetu Pozna´nskiego6, 61-614 Pozna´n,Poland 2 Department of Molecular and Cellular Biology, Institute of Molecular Biology and Biotechnology, Faculty of Biology, Adam Mickiewicz University, ul. Uniwersytetu Pozna´nskiego6, 61-614 Pozna´n,Poland; [email protected] * Correspondence: [email protected] (E.P.); [email protected] (J.D.); Tel.: +48-61-829-5857 (E.P.) Received: 19 November 2020; Accepted: 6 December 2020; Published: 8 December 2020 Abstract: KMT2 (histone-lysine N-methyltransferase subclass 2) complexes methylate lysine 4 on the histone H3 tail at gene promoters and gene enhancers and, thus, control the process of gene transcription. These complexes not only play an essential role in normal development but have also been described as involved in the aberrant growth of tissues. KMT2 mutations resulting from the rearrangements of the KMT2A (MLL1) gene at 11q23 are associated with pediatric mixed-lineage leukemias, and recent studies demonstrate that KMT2 genes are frequently mutated in many types of human cancers. Moreover, other components of the KMT2 complexes have been reported to contribute to oncogenesis. This review summarizes the recent advances in our knowledge of the role of KMT2 complexes in cell transformation. In addition, it discusses the therapeutic targeting of different components of the KMT2 complexes. Keywords: histone–lysine N-methyltransferase 2; COMPASS; COMPASS-like; H3K4 methylation; oncogenesis; cancer; epigenetics; chromatin 1. -

Genome-Wide Analysis of Androgen Receptor Binding and Gene Regulation in Two CWR22-Derived Prostate Cancer Cell Lines
Endocrine-Related Cancer (2010) 17 857–873 Genome-wide analysis of androgen receptor binding and gene regulation in two CWR22-derived prostate cancer cell lines Honglin Chen1, Stephen J Libertini1,4, Michael George1, Satya Dandekar1, Clifford G Tepper 2, Bushra Al-Bataina1, Hsing-Jien Kung2,3, Paramita M Ghosh2,3 and Maria Mudryj1,4 1Department of Medical Microbiology and Immunology, University of California Davis, 3147 Tupper Hall, Davis, California 95616, USA 2Division of Basic Sciences, Department of Biochemistry and Molecular Medicine, Cancer Center and 3Department of Urology, University of California Davis, Sacramento, California 95817, USA 4Veterans Affairs Northern California Health Care System, Mather, California 95655, USA (Correspondence should be addressed to M Mudryj at Department of Medical Microbiology and Immunology, University of California, Davis; Email: [email protected]) Abstract Prostate carcinoma (CaP) is a heterogeneous multifocal disease where gene expression and regulation are altered not only with disease progression but also between metastatic lesions. The androgen receptor (AR) regulates the growth of metastatic CaPs; however, sensitivity to androgen ablation is short lived, yielding to emergence of castrate-resistant CaP (CRCaP). CRCaP prostate cancers continue to express the AR, a pivotal prostate regulator, but it is not known whether the AR targets similar or different genes in different castrate-resistant cells. In this study, we investigated AR binding and AR-dependent transcription in two related castrate-resistant cell lines derived from androgen-dependent CWR22-relapsed tumors: CWR22Rv1 (Rv1) and CWR-R1 (R1). Expression microarray analysis revealed that R1 and Rv1 cells had significantly different gene expression profiles individually and in response to androgen. -
Mechanisms Directing Receptor-Specific Gene Regulation
Mechanisms Directing Receptor-Specific Gene Regulation by the Androgen and Glucocorticoid Receptor Inaugural-Dissertation to obtain the academic degree Doctor rerum naturalium (Dr. rer. nat.) submitted to the Department of Biology, Chemistry, Pharmacy of Freie Universität Berlin by Marina Kulik • 2021 The dissertation was prepared under the supervision of Dr. Sebastiaan H. Meijsing at the Max Planck Institute for Molecular Genetics in Berlin from September 2015 to February 2021. 1st Reviewer: Dr. Sebastiaan Meijsing 2nd Reviewer: Prof. Dr. Markus Wahl Date of defense: 21.05.2021 1 Selbstständigkeitserklärung Hiermit bestätige ich, dass ich die vorliegende Arbeit selbstständig und unter Zuhilfenahme der angegebenen Literatur erstellt habe. Acknowledgments First of all, I would like to express my gratitude to my supervisor Sebastiaan Meijsing for his support and guidance during my PhD. I would like to thank Martin Vingron for the opportunity to be part of his research group and for the great collaborations. Especially, I would like to thank Stefan Haas for introducing me to the world of RNA-seq and Gözde Kibar, who contributed with her bioinformatical analyses to this work. I would like to thank Sarah Kinkley for her support and for giving me the opportunity to finish my PhD in her group. I wish to thank Stefan Prekovic, Isabel Mayayo-Peralta and Wilbert Zwart from the NKI in Amsterdam for sharing their expertise in “nuclear signaling” and the great collaboration. I am particularly grateful to Melissa Bothe, her computational analyses and support in the lab contributed a lot to this work. My special gratitude goes to Laura Glaser for her continuous advice and for freezing my cells in the evening countless times. -

Noelia Díaz Blanco
Effects of environmental factors on the gonadal transcriptome of European sea bass (Dicentrarchus labrax), juvenile growth and sex ratios Noelia Díaz Blanco Ph.D. thesis 2014 Submitted in partial fulfillment of the requirements for the Ph.D. degree from the Universitat Pompeu Fabra (UPF). This work has been carried out at the Group of Biology of Reproduction (GBR), at the Department of Renewable Marine Resources of the Institute of Marine Sciences (ICM-CSIC). Thesis supervisor: Dr. Francesc Piferrer Professor d’Investigació Institut de Ciències del Mar (ICM-CSIC) i ii A mis padres A Xavi iii iv Acknowledgements This thesis has been made possible by the support of many people who in one way or another, many times unknowingly, gave me the strength to overcome this "long and winding road". First of all, I would like to thank my supervisor, Dr. Francesc Piferrer, for his patience, guidance and wise advice throughout all this Ph.D. experience. But above all, for the trust he placed on me almost seven years ago when he offered me the opportunity to be part of his team. Thanks also for teaching me how to question always everything, for sharing with me your enthusiasm for science and for giving me the opportunity of learning from you by participating in many projects, collaborations and scientific meetings. I am also thankful to my colleagues (former and present Group of Biology of Reproduction members) for your support and encouragement throughout this journey. To the “exGBRs”, thanks for helping me with my first steps into this world. Working as an undergrad with you Dr. -

RCHY1 Antibody
Efficient Professional Protein and Antibody Platforms RCHY1 Antibody Basic information: Catalog No.: UMA60398 Source: Mouse Size: 50ul/100ul Clonality: Monoclonal Concentration: 1mg/ml Isotype: Mouse IgG1 Purification: Protein A affinity purified Useful Information: WB:1:500-1:1000 ICC:1:50-1:200 Applications: IHC:1:50-1:200 FC:1:100-1:200 Reactivity: Human, Rat Specificity: This antibody recognizes RCHY1 protein. Immunogen: Recombinant protein Pirh2, also known as Androgen receptor N-terminal-interacting protein (ARNIP), ZN363 or CHIMP, has p53-induced ubiquitin-protein ligase activity, promoting p53 degradation. The protein physically interacts with p53 and the resulting degradation of p53 renders Pirh2 an oncogenic protein as the loss of p53 function contributes to malignant tumor development. The gene Description: encoding for the protein maps to chromosome 4q21.1 and transcription of this gene is regulated by p53. Pirh2 expression decreases the level of p53 and a decrease of endogenous Pirh2 expression ups p53 levels. Pirh2 is therefore considered, together with MDM2, to be acting as a negative reg- ulator of p53 function. Uniprot: Q96PM5(Human) BiowMW: 30 kDa Buffer: 1*TBS (pH7.4), 1%BSA, 40%Glycerol. Preservative: 0.05% Sodium Azide. Storage: Store at 4°C short term and -20°C long term. Avoid freeze-thaw cycles. Note: For research use only, not for use in diagnostic procedure. Data: Western blot analysis of Pirh2 on different cell lysate using anti-Pirh2 antibody at 1/1,000 dilu- tion. Positive control: Line1: HelaLine2: A549 Line3: MCF-7 Line4: PC-12 Gene Universal Technology Co. Ltd www.universalbiol.com Tel: 0550-3121009 E-mail: [email protected] Efficient Professional Protein and Antibody Platforms ICC staining Pirh2 (green) and Actin filaments (red) in Hela cells. -

Aneuploidy: Using Genetic Instability to Preserve a Haploid Genome?
Health Science Campus FINAL APPROVAL OF DISSERTATION Doctor of Philosophy in Biomedical Science (Cancer Biology) Aneuploidy: Using genetic instability to preserve a haploid genome? Submitted by: Ramona Ramdath In partial fulfillment of the requirements for the degree of Doctor of Philosophy in Biomedical Science Examination Committee Signature/Date Major Advisor: David Allison, M.D., Ph.D. Academic James Trempe, Ph.D. Advisory Committee: David Giovanucci, Ph.D. Randall Ruch, Ph.D. Ronald Mellgren, Ph.D. Senior Associate Dean College of Graduate Studies Michael S. Bisesi, Ph.D. Date of Defense: April 10, 2009 Aneuploidy: Using genetic instability to preserve a haploid genome? Ramona Ramdath University of Toledo, Health Science Campus 2009 Dedication I dedicate this dissertation to my grandfather who died of lung cancer two years ago, but who always instilled in us the value and importance of education. And to my mom and sister, both of whom have been pillars of support and stimulating conversations. To my sister, Rehanna, especially- I hope this inspires you to achieve all that you want to in life, academically and otherwise. ii Acknowledgements As we go through these academic journeys, there are so many along the way that make an impact not only on our work, but on our lives as well, and I would like to say a heartfelt thank you to all of those people: My Committee members- Dr. James Trempe, Dr. David Giovanucchi, Dr. Ronald Mellgren and Dr. Randall Ruch for their guidance, suggestions, support and confidence in me. My major advisor- Dr. David Allison, for his constructive criticism and positive reinforcement. -

Pentosan Polysulfate Binds to STRO
Wu et al. Stem Cell Research & Therapy (2017) 8:278 DOI 10.1186/s13287-017-0723-y RESEARCH Open Access Pentosan polysulfate binds to STRO-1+ mesenchymal progenitor cells, is internalized, and modifies gene expression: a novel approach of pre-programing stem cells for therapeutic application requiring their chondrogenesis Jiehua Wu1,7, Susan Shimmon1,8, Sharon Paton2, Christopher Daly3,4,5, Tony Goldschlager3,4,5, Stan Gronthos6, Andrew C. W. Zannettino2 and Peter Ghosh1,5* Abstract Background: The pharmaceutical agent pentosan polysulfate (PPS) is known to induce proliferation and chondrogenesis of mesenchymal progenitor cells (MPCs) in vitro and in vivo. However, the mechanism(s) of action of PPS in mediating these effects remains unresolved. In the present report we address this issue by investigating the binding and uptake of PPS by MPCs and monitoring gene expression and proteoglycan biosynthesis before and after the cells had been exposed to limited concentrations of PPS and then re-established in culture in the absence of the drug (MPC priming). Methods: Immuno-selected STRO-1+ mesenchymal progenitor stem cells (MPCs) were prepared from human bone marrow aspirates and established in culture. The kinetics of uptake, shedding, and internalization of PPS by MPCs was determined by monitoring the concentration-dependent loss of PPS media concentrations using an enzyme-linked immunosorbent assay (ELISA) and the uptake of fluorescein isothiocyanate (FITC)-labelled PPS by MPCs. The proliferation of MPCs, following pre-incubation and removal of PPS (priming), was assessed using the Wst-8 assay 35 method, and proteoglycan synthesis was determined by the incorporation of SO4 into their sulphated glycosaminoglycans. -

Loss of Supervillin Causes Myopathy with Myofibrillar Disorganization and Autophagic Vacuoles
University of Massachusetts Medical School eScholarship@UMMS Open Access Articles Open Access Publications by UMMS Authors 2020-08-01 Loss of supervillin causes myopathy with myofibrillar disorganization and autophagic vacuoles Carola Hedberg-Oldfors University of Gothenburg Et al. Let us know how access to this document benefits ou.y Follow this and additional works at: https://escholarship.umassmed.edu/oapubs Part of the Amino Acids, Peptides, and Proteins Commons, Cardiovascular Diseases Commons, Cell Biology Commons, Cellular and Molecular Physiology Commons, Molecular and Cellular Neuroscience Commons, Musculoskeletal Diseases Commons, Musculoskeletal, Neural, and Ocular Physiology Commons, Nervous System Diseases Commons, and the Neurology Commons Repository Citation Hedberg-Oldfors C, Luna EJ, Oldfors A, Knopp C. (2020). Loss of supervillin causes myopathy with myofibrillar disorganization and autophagic vacuoles. Open Access Articles. https://doi.org/10.1093/ brain/awaa206. Retrieved from https://escholarship.umassmed.edu/oapubs/4320 Creative Commons License This work is licensed under a Creative Commons Attribution-Noncommercial 4.0 License This material is brought to you by eScholarship@UMMS. It has been accepted for inclusion in Open Access Articles by an authorized administrator of eScholarship@UMMS. For more information, please contact [email protected]. doi:10.1093/brain/awaa206 BRAIN 2020: 143; 2406–2420 | 2406 Loss of supervillin causes myopathy with Downloaded from https://academic.oup.com/brain/article/143/8/2406/5890852 by Medical Center Library user on 17 September 2020 myofibrillar disorganization and autophagic vacuoles Carola Hedberg-Oldfors,1,* Robert Meyer,2,* Kay Nolte,3,* Yassir Abdul Rahim,1 Christopher Lindberg,4 Kristjan Karason,5 Inger Johanne Thuestad,6 Kittichate Visuttijai,1 Mats Geijer,7,8 Matthias Begemann,2 Florian Kraft,2 Eva Lausberg,2 Lea Hitpass,9 Rebekka Go¨tzl,10 Elizabeth J. -

Mutational Landscape and Clinical Outcome of Patients with De Novo Acute Myeloid Leukemia and Rearrangements Involving 11Q23/KMT2A
Mutational landscape and clinical outcome of patients with de novo acute myeloid leukemia and rearrangements involving 11q23/KMT2A Marius Billa,1,2, Krzysztof Mrózeka,1,2, Jessica Kohlschmidta,b, Ann-Kathrin Eisfelda,c, Christopher J. Walkera, Deedra Nicoleta,b, Dimitrios Papaioannoua, James S. Blachlya,c, Shelley Orwicka,c, Andrew J. Carrolld, Jonathan E. Kolitze, Bayard L. Powellf, Richard M. Stoneg, Albert de la Chapelleh,i,2, John C. Byrda,c, and Clara D. Bloomfielda,c aThe Ohio State University Comprehensive Cancer Center, Columbus, OH 43210; bAlliance for Clinical Trials in Oncology Statistics and Data Center, The Ohio State University Comprehensive Cancer Center, Columbus, OH 43210; cDivision of Hematology, Department of Internal Medicine, The Ohio State University Comprehensive Cancer Center, Columbus, OH 43210; dDepartment of Genetics, University of Alabama at Birmingham, Birmingham, AL 35294; eNorthwell Health Cancer Institute, Zucker School of Medicine at Hofstra/Northwell, Lake Success, NY 11042; fDepartment of Internal Medicine, Section on Hematology & Oncology, Wake Forest Baptist Comprehensive Cancer Center, Winston-Salem, NC 27157; gDepartment of Medical Oncology, Dana-Farber/Partners Cancer Care, Boston, MA 02215; hHuman Cancer Genetics Program, Comprehensive Cancer Center, The Ohio State University, Columbus, OH 43210; and iDepartment of Cancer Biology and Genetics, Comprehensive Cancer Center, The Ohio State University, Columbus, OH 43210 Contributed by Albert de la Chapelle, August 28, 2020 (sent for review July 17, 2020; reviewed by Anne Hagemeijer and Stefan Klaus Bohlander) Balanced rearrangements involving the KMT2A gene, located at patterns that include high expression of HOXA genes and thereby 11q23, are among the most frequent chromosome aberrations in contribute to leukemogenesis (14–16). -

A Dissertation Entitled the Androgen Receptor
A Dissertation entitled The Androgen Receptor as a Transcriptional Co-activator: Implications in the Growth and Progression of Prostate Cancer By Mesfin Gonit Submitted to the Graduate Faculty as partial fulfillment of the requirements for the PhD Degree in Biomedical science Dr. Manohar Ratnam, Committee Chair Dr. Lirim Shemshedini, Committee Member Dr. Robert Trumbly, Committee Member Dr. Edwin Sanchez, Committee Member Dr. Beata Lecka -Czernik, Committee Member Dr. Patricia R. Komuniecki, Dean College of Graduate Studies The University of Toledo August 2011 Copyright 2011, Mesfin Gonit This document is copyrighted material. Under copyright law, no parts of this document may be reproduced without the expressed permission of the author. An Abstract of The Androgen Receptor as a Transcriptional Co-activator: Implications in the Growth and Progression of Prostate Cancer By Mesfin Gonit As partial fulfillment of the requirements for the PhD Degree in Biomedical science The University of Toledo August 2011 Prostate cancer depends on the androgen receptor (AR) for growth and survival even in the absence of androgen. In the classical models of gene activation by AR, ligand activated AR signals through binding to the androgen response elements (AREs) in the target gene promoter/enhancer. In the present study the role of AREs in the androgen- independent transcriptional signaling was investigated using LP50 cells, derived from parental LNCaP cells through extended passage in vitro. LP50 cells reflected the signature gene overexpression profile of advanced clinical prostate tumors. The growth of LP50 cells was profoundly dependent on nuclear localized AR but was independent of androgen. Nevertheless, in these cells AR was unable to bind to AREs in the absence of androgen.