YF-VAX® Rx Only AHFS Category
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Safety of Immunization During Pregnancy a Review of the Evidence
Safety of Immunization during Pregnancy A review of the evidence Global Advisory Committee on Vaccine Safety © World Health Organization 2014 All rights reserved. Publications of the World Health Organization are available on the WHO website (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications –whether for sale or for non-commercial distribution– should be addressed to WHO Press through the WHO website (www.who.int/about/licensing/copyright_form/en/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. -
Pneumococcal Vaccine
Vaccines for Primary Care Pneumococcal, Shingles, Pertussis Devang Patel, M.D. Assistant Professor Chief of Service, MICU ID Service University of Maryland School of Medicine Pneumococcal Vaccine Pneumococcal Disease • 2nd most common cause of vaccine preventable death in the US • Major Syndromes – Pneumonia – Bacteremia – Meningitis Active Bacterial Core Surveillance (ABCs) Report Emerging Infections Program Network Streptococcus pneumoniae, 2010 (ORIG) Vaccine Target • Polysaccharide capsule allows bacteria to resist phagocytosis • Antibodies to capsule facilitate phagocytosis • >90 different pneumococcal capsular serotypes • Vaccines contain most common serotypes causing disease Pneumococcal Vaccines Pneumococcal Vaccines • Pneumococcal polysaccharide vaccine (PPSV23; Pneumovax) – Contains capsular polysaccharides – 23 most commonly infecting serotypes • Cause 60% of all pneumococcal infections in adults – Not recommended for children <2 due to poor immunogenicity of polysaccharides Pneumococcal Vaccines • Pneumococcal conjugate vaccine (PCV13, Prevnar) – Polysaccharides linked to nontoxic protein • higher antigenicity – Stimulates mucosal antibody • Eliminates nasal carriage in young children • Herd effect in adults – Reduction in PCV7 serotype disease >90% Prevnar 13 • 2000 - PCV7 approved for infants toddlers • 2010 - PCV13 recommended for infants and toddlers • 2012 – ACIP recommended PCV13 for high- risk adults • 2014 – recommended for adults >65 • 2018 – ACIP will revisit PCV13 use in adults – Childhood vaccines may eliminate -

Summary Guide to Tetanus Prophylaxis in Routine Wound Management
Summary Guide to Tetanus Prophylaxis in Routine Wound Management ASSESS WOUND A clean, minor wound All other wounds (contaminated with dirt, feces, saliva, soil; puncture wounds; avulsions; wounds resulting from flying or crushing objects, animal bites, burns, frostbite) Has patient completed a primary Has patient completed a primary tetanus diphtheria series?1, 7 tetanus diphtheria series?1, 7 No/Unknown Yes No/Unknown Yes Administer vaccine today.2,3,4 Was the most recent Administer vaccine and Was the most Instruct patient to complete dose within the past tetanus immune gobulin recent dose within series per age-appropriate 10 years? (TIG) now.2,4,5,6,7 the past 5 years?7 vaccine schedule. No Yes No Yes Vaccine not needed today. Vaccine not needed today. Administer vaccine today.2,4 2,4 Patient should receive next Administer vaccine today. Patient should receive next Patient should receive next dose Patient should receive next dose dose at 10-year interval after dose at 10-year interval after per age-appropriate schedule. per age-appropriate schedule. last dose. last dose. 1 A primary series consists of a minimum of 3 doses of tetanus- and diphtheria- 4 Tdap* is preferred for persons 11 through 64 years of age if using Adacel* or 10 years of containing vaccine (DTaP/DTP/Tdap/DT/Td). age and older if using Boostrix* who have never received Tdap. Td is preferred to tetanus 2 Age-appropriate vaccine: toxoid (TT) for persons 7 through 9 years, 65 years and older, or who have received a • DTaP for infants and children 6 weeks up to 7 years of age (or DT pediatric if Tdap previously. -

Vaccines for Preteens
| DISEASES and the VACCINES THAT PREVENT THEM | INFORMATION FOR PARENTS Vaccines for Preteens: What Parents Should Know Last updated JANUARY 2017 Why does my child need vaccines now? to get vaccinated. The best time to get the flu vaccine is as soon as it’s available in your community, ideally by October. Vaccines aren’t just for babies. Some of the vaccines that While it’s best to be vaccinated before flu begins causing babies get can wear off as kids get older. And as kids grow up illness in your community, flu vaccination can be beneficial as they may come in contact with different diseases than when long as flu viruses are circulating, even in January or later. they were babies. There are vaccines that can help protect your preteen or teen from these other illnesses. When should my child be vaccinated? What vaccines does my child need? A good time to get these vaccines is during a yearly health Tdap Vaccine checkup. Your preteen or teen can also get these vaccines at This vaccine helps protect against three serious diseases: a physical exam required for sports, school, or camp. It’s a tetanus, diphtheria, and pertussis (whooping cough). good idea to ask the doctor or nurse every year if there are any Preteens should get Tdap at age 11 or 12. If your teen didn’t vaccines that your child may need. get a Tdap shot as a preteen, ask their doctor or nurse about getting the shot now. What else should I know about these vaccines? These vaccines have all been studied very carefully and are Meningococcal Vaccine safe. -
Commonly Administered Vaccines
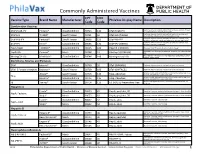
Commonly Administered Vaccines CPT CVX Vaccine Type Brand Name Manufacturer PhilaVax Display Name Description Code Code Combination Vaccines Diptheria, tetanus toxoids and acellular pertussis vaccine, Hepati- DTaP-HepB-IPV Pediarix® GlaxoSmithKline 90723 110 DTaP-HepB-IPV tis B and poliovirus vaccine, inactivated Diptheria, tetanus toxoids and acellular pertussis vaccine and DTaP-Hib TriHIBit® Sanofi Pasteur 90721 50 DTaP-Hib (TriHIBit) Haemophilus influenzae type b conjugate vaccine Diptheria, tetanus toxoids and acellular pertussis vaccine, Hae- DTaP-Hib-IPV Pentacel® Sanofi Pasteur 90698 120 DTaP-Hib-IPV mophilus influenzae type b, and poliovirus vaccine, inactivated Diptheria, tetanus toxoids and acellular pertussis vaccine, and DTaP-IPV Kinrix® GlaxoSmithKline 90696 130 DTaP-IPV (KINRIX) poliovirus vaccine, inactivated HepA-HepB TWINRIX® GlaxoSmithKline 90636 104 HepA/B (TWINRIX) Hepatisis A and Hepatitis B vaccine, adult dosage Hepatitis B and Hemophilus influenza b vaccine, for intramuscular HepB-Hib Comvax® Merck 90748 51 Hib-Hep B (COMVAX) use Haemophilus influenza b and meningococcal sero groups C and Y MeningC/Y-Hib Menhibrix® GlaxoSmithKline 90644 148 Meningococcal-Hib vaccine, 4 dose series Diphtheria, Tetanus and Pertussis DTaP Infanrix® GlaxoSmithKline 90700 20 DTaP (INFANRIX) Diptheria, tetanus toxoids and acellular pertussis vaccine DTaP, 5 Pertussis Antigens Daptacel® Sanofi Pasteur 90700 106 DTaP (DAPTACEL) Diptheria, tetanus toxoids and acellular pertussis vaccine Tetanus toxoid, reduced diphtheria toxoid, and acellular -

Ensuring the World's Poorest Children Benefit from Lifesaving Vaccines
WHAT WE’RE LEARNING Ensuring the World’s Poorest Children Benefit from Lifesaving Vaccines “Supporting children’s immunization is undoubtedly the best investment we’ve ever made.” —Bill and Melinda Gates Program Area pertussis) vaccine. When GAVI was The Challenge launched, 71 percent of the world’s Global Health Most people in rich nations do not children were receiving DTP vaccine. realize how difficult it is simply to By 2004, the rate had increased to survive early childhood in many parts Our Goal 78 percent. of the world. Every year, more than Prevent needless deaths in the world’s GAVI has concentrated the greatest 10 million children are buried before poorest countries by increasing access percentage of its resources on speeding they reach their fifth birthday. Of these, to basic vaccines and speeding the the introduction of newer, more about 1.4 million die from diseases that introduction of new vaccines. expensive vaccines, including those for existing vaccines can prevent—including hepatitis B, Haemophilus influenzae B measles, pertussis, and tetanus. Another Our Progress in Brief (Hib), and yellow fever. The vaccine 1.1 million die from diseases for which The Global Alliance for Vaccines for hepatitis B, for example, had been we will soon have vaccines. Because and Immunization (GAVI), which widely used in rich countries for childhood death is so frequent, parents the foundation helped to launch in 20 years but was severely underutilized in some countries in Africa and Asia 1999, has made significant progress. in the developing world because of a don’t even name their babies until they Children’s immunization is no longer a lack of political will and the vaccine’s reach several months of age. -
Association Between Thimerosal-Containing Vaccine and Autism
BRIEF REPORT Association Between Thimerosal-Containing Vaccine and Autism Anders Hviid, MSc Context Mercuric compounds are nephrotoxic and neurotoxic at high doses. Thi- Michael Stellfeld, MD merosal, a preservative used widely in vaccine formulations, contains ethylmercury. Thus it has been suggested that childhood vaccination with thimerosal-containing vac- Jan Wohlfahrt, MSc cine could be causally related to neurodevelopmental disorders such as autism. Mads Melbye, MD, PhD Objective To determine whether vaccination with a thimerosal-containing vaccine is associated with development of autism. IGH DOSES OF MERCURIC COM- Design, Setting, and Participants Population-based cohort study of all children pounds are nephrotoxic and born in Denmark from January 1, 1990, until December 31, 1996 (N=467450) com- neurotoxic.1 Thimerosal, an paring children vaccinated with a thimerosal-containing vaccine with children vacci- organic compound that con- nated with a thimerosal-free formulation of the same vaccine. Htains ethylmercury, has been widely used Main Outcome Measures Rate ratio (RR) for autism and other autistic-spectrum since the 1930s as a preservative in cer- disorders, including trend with dose of ethylmercury. tain vaccines. In the 1990s, an increas- Results During 2986654 person-years, we identified 440 autism cases and 787 cases ing number of different vaccines con- of other autistic-spectrum disorders. The risk of autism and other autistic-spectrum taining thimerosal were introduced in disorders did not differ significantly between children vaccinated with thimerosal- immunization schedules around the containing vaccine and children vaccinated with thimerosal-free vaccine (RR, 0.85 [95% world, and thus the average cumula- confidence interval {CI}, 0.60-1.20] for autism; RR, 1.12 [95% CI, 0.88-1.43] for other tive exposure to thimerosal in infants has autistic-spectrum disorders). -

Diphtheria Tetanus and Pertussis Vaccine Supply Update October 2016
Diphtheria Tetanus and Pertussis Vaccine Supply Update UNICEF Supply Division October 2016 0 Diphtheria Tetanus and Pertussis Vaccine Supply Update October 2016 This update provides information on diphtheria, tetanus, and whole cell pertussis (DTwP) vaccines and UNICEF’s long-term arrangement issuance to two manufacturers with significant production capacity. Lead times for delivery through UNICEF have now reduced to eight weeks. DTP vaccine containing acellular pertussis (DTaP) availability through UNICEF remains limited and currently unavailable through 2018. 1. Summary The DTwP vaccine market remains fragile, characterized by low-demand volumes. While multiple DTwP vaccine manufacturers of WHO prequalified DTwP exist, only two currently offer prequalified DTwP vaccine through UNICEF. DTwP vaccine lead-time for delivery from manufacturers through UNICEF has reduced from six months to eight weeks from purchase order placement, as a result of additional supply availability, and procurement no longer being dependent on a single manufacturer. However, globally, standalone DTwP vaccine availability has decreased as manufacturers allocate existing DTwP bulk to produce DTwP-containing combination vaccines, particularly pentavalent DTwP-containing combination vaccines with antigens against Hepatitis B and Haemophilus Influenzae type b. UNICEF DTwP vaccine procurement since 2012 declined from approximately 20 million doses to reach an average 5 million doses per year, mainly as countries switched to other DTwP combination vaccines. Countries continue to seek to secure access to DTaP combination vaccines through UNICEF. However, global supply availability remains very limited and currently unavailable through UNICEF. UNICEF anticipates earliest availability end 2018-2019. 2. Background & Procurement History DTP vaccines have been part of the Expanded Programme of Immunization (EPI) vaccination schedule since 1974.1 Historically, several manufacturers with sufficient supply met global DTP vaccine demand. -

XXV TAG Meeting
XXV TAG Meeting Twenty-Fifth Meeting of the Technical Advisory Group (TAG) on Vaccine-preventable Diseases 9-11 July 2019 Cartagena, Colombia 1 TAG Members J. Peter Figueroa TAG Chair Professor of Public Health, Epidemiology & HIV/AIDS University of the West Indies Kingston, Jamaica Jon K. Andrus Adjunct Professor and Senior Investigator Center for Global Health, Division of Vaccines and Immunization University of Colorado Washington, DC, United States Pablo Bonvehi Scientific Director VACUNAR S.A. Buenos Aires, Argentina Roger Glass* Director Fogarty International Center & Associate Director for International Research NIH/JEFIC-National Institutes of Health Bethesda, MD, United States Akira Homma Chairman of Policy and Strategy Council Bio-Manguinhos Institute Rio de Janeiro, Brazil Arlene King Adjunct Professor Dalla Lana School of Public Health University of Toronto Ontario, Canada Nancy Messonnier* Director National Center for Immunization and Respiratory Diseases Centers for Disease Control and Prevention Decatur, GA, United States José Ignacio Santos Secretary General Health Council Government of Mexico Mexico City, Mexico Cristiana M. Toscano 2 Head of the Department of Collective Health Institute of Tropical Pathology and Public Health, Federal University of Goiás Goiania, Brazil Cuauhtémoc Ruiz-Matus Ad hoc Secretary Unit Chief Comprehensive Family Immunization PAHO/WHO Washington, DC, United States * Not present at the meeting 3 Table of Contents Contents Acronyms ..........................................................................................................................................6 -

Global Vaccination: Trends and U.S
Global Vaccination: Trends and U.S. Role October 18, 2019 Congressional Research Service https://crsreports.congress.gov R45975 SUMMARY R45975 Global Vaccination: Trends and U.S. Role October 18, 2019 For more than 50 years, the United States has taken an interest in the eradication of vaccine- preventable diseases (VPDs) in children worldwide, as well as vaccine research and Sara M. Tharakan development, particularly since playing a vital role in the global campaign to eradicate smallpox Analyst in Global Health in the 1960s. Since then, vaccinating children against VPDs has been a major U.S. foreign policy and International effort. Development Vaccinations are one of the most cost-effective ways to prevent infectious disease and associated morbidity and mortality. According to UNICEF, immunizations save around 3 million lives per year. As of 2019, VPDs continue to cause high levels of morbidity (illness) and mortality (death), and the World Health Organization (WHO) notes that the adoption of new vaccines by low- and middle-income countries (which often have the highest disease burdens) has been slower than in high-income countries. Receiving a vaccination during childhood can protect the recipient from VPDs, decrease the spread of related diseases, and improve child survival prospects (as children, particularly those under five years old, are more likely than adults to die from VPDs). Recently, a global resurgence of certain VPDs has caused concern among public health officials and drawn attention to the challenges of vaccine hesitancy and stigma. For example, polio continues to elude global eradication and remains endemic in three countries. In 2019 measles has seen a resurgence in some middle- and high-income countries due to a variety of factors, including reluctance among some individuals and religious communities to vaccinate their children. -
HPV and Adolescent Vaccine Toolkit: Clinician Guide Contents
HPV and Adolescent Vaccine Toolkit: Clinician Guide CONTENTS I. 2018 IMMUNIZATION SCHEDULES & SCREENING RESOURCES Recommended & Catch-up Immunization Schedule (Birth-18 Years) Lists the ages or age range each vaccine is recommended. Schedules are updated annually. Please visit https://www.cdc.gov/vaccines/schedules/ for the most up-to-date schedules. Clinician FAQ: CDC Recommendations for HPV Vaccine 2-Dose Schedules Helps explain the new HPV vaccine recommendation for adolescents (2 doses recommended for adolescents starting the series before their 15th birthday; 3 doses recommended for adolescents starting the series after their 15th birthday) and provides tips for talking to parents about the change. HPV 2-Dose Decision Tree Follow the decision tree chart to determine whether your patient needs two or three doses of HPV vaccine. II. ADDRESSING VACCINE HESITANCY Talking to Parents About the HPV Vaccine A collection of questions parents may have surrounding the HPV vaccine and responses healthcare providers can use to address the concerns. Let’s Talk Vaccines: A Guide to Conversations About Immunizations Parents ask tough questions! Use this resource from Northwest Vax to provide a strong recommendation using the Ask. Acknowledge. Advise model. III. BEST PRACTICES AND STRATEGIES FOR IMPROVING IMMUNIZATION COVERAGE RATES Strategies for Improving Adolescent Immunization Coverage Rates Use the strategies in this AAP resource to help your practice improve adolescent immunization coverage rates among your patients. Documenting Parental Refusal to Have Their Children Vaccinated Provides tips from the AAP on ways to communicate with and educate parents who refuse immunizations. Includes a template for use by health care providers to document refusals. -
General Vaccine Information
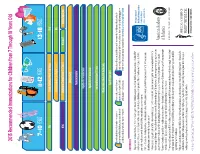
2015 Recommended Immunizations for Children from 7 Through 18 Years Old 7–10 YEARS 11-12 YEARS 13-18 YEARS Tdap 1 Tetanus, Diphtheria, Pertussis (Tdap) Vaccine Tdap Human Papillomavirus (HPV) Vaccine (3 Doses)2 HPV MCV4 Meningococcal Conjugate Vaccine (MCV4) Dose 13 MCV4 Dose 13 Booster at age 16 years Influenza (Yearly)4 Pneumococcal Vaccine5 Hepatitis A (HepA) Vaccine Series6 Hepatitis B (HepB) Vaccine Series Inactivated Polio Vaccine (IPV) Series Measles, Mumps, Rubella (MMR) Vaccine Series Varicella Vaccine Series These shaded boxes indicate when the vaccine is These shaded boxes indicate the These shaded boxes indicate the vaccine is recommended for children with certain health recommended for all children unless your doctor tells vaccine should be given if a child is conditions that put them at high risk for serious diseases. Note that healthy children can get the you that your child cannot safely receive the vaccine. catching-up on missed vaccines. HepA series6. See vaccine-specific recommendations at www.cdc.gov/vaccines/pubs/ACIP-list.htm. FOOTNOTES 1 Tdap vaccine is recommended at age 11 or 12 to protect against tetanus, diphtheria and pertussis. If your child has not received any or all of the DTaP vaccine series, or if you don’t know if your child has received these shots, your child needs a single dose of Tdap when they are 7 -10 years old. Talk to your child’s health care provider to find out if they need additional catch-up vaccines. 2 All 11 or 12 year olds – both girls and boys – should receive 3 doses of HPV vaccine to protect against HPV-related disease.