Somalia Nutrition Cluster Geo-Tagging: Capacity Assessment
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
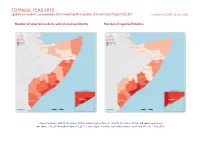
SOMALIA, YEAR 2019: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 22 June 2020
SOMALIA, YEAR 2019: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 22 June 2020 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; Ethiopia/Somalia bor- der status: CIA, 2014; incident data: ACLED, 13 June 2020; coastlines and inland waters: Smith and Wessel, 1 May 2015 SOMALIA, YEAR 2019: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 22 JUNE 2020 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Battles 1131 458 2154 Conflict incidents by category 2 Explosions / Remote 621 228 1221 Development of conflict incidents from 2010 to 2019 2 violence Violence against civilians 530 358 640 Methodology 3 Strategic developments 140 6 16 Conflict incidents per province 4 Protests 78 2 2 Riots 19 3 5 Localization of conflict incidents 4 Total 2519 1055 4038 Disclaimer 6 This table is based on data from ACLED (datasets used: ACLED, 13 June 2020). Development of conflict incidents from 2010 to 2019 This graph is based on data from ACLED (datasets used: ACLED, 13 June 2020). 2 SOMALIA, YEAR 2019: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 22 JUNE 2020 Methodology on what level of detail is reported. Thus, towns may represent the wider region in which an incident occured, or the provincial capital may be used if only the province The data used in this report was collected by the Armed Conflict Location & Event is known. -

Afmadow District Detailed Site Assessment Lower Juba Region, Somalia
Afmadow district Detailed Site Assessment Lower Juba Region, Somalia Introduction Location map The Detailed Site Assessment (DSA) was triggered in the perspectives of different groups were captured2. KI coordination with the Camp Coordination and Camp responses were aggregated for each site. These were then Management (CCCM) Cluster in order to provide the aggregated further to the district level, with each site having humanitarian community with up-to-date information on an equal weight. Data analysis was done by thematic location of internally displaced person (IDP) sites, the sectors, that is, protection, water, sanitation and hygiene conditions and capacity of the sites and the humanitarian (WASH), shelter, displacement, food security, health and needs of the residents. The first round of the DSA took nutrition, education and communication. place from October 2017 to March 2018 assessing a total of 1,843 sites in 48 districts. The second round of the DSA This factsheet presents a summary of profiles of assessed sites3 in Afmadow District along with needs and priorities of took place from 1 September 2018 to 31 January 2019 IDPs residing in these sites. As the data is captured through assessing a total of 1778 sites in 57 districts. KIs, findings should be considered indicative rather than A grid pattern approach1 was used to identify all IDP generalisable. sites in a specific area. In each identified site, two key Number of assessed sites: 14 informants (KIs) were interviewed: the site manager or community leader and a women’s representative, to ensure Assessed IDP sites in Afmadow4 Coordinates: Lat. 0.6, Long. -

SOMALIA Food Security Outlook October 2018 to May 2019
SOMALIA Food Security Outlook October 2018 to May 2019 Deyr rainfall expected to sustain current outcomes, except in some pastoral areas KEY MESSAGES Current food security outcomes, October 2018 • Food security has continued to improve throughout Somalia since the 2018 Gu. Most northern and central livelihood zones are Stressed (IPC Phase 2), while southern livelihood zones are Minimal (IPC Phase 1) or Stressed (IPC Phase 2). In October, humanitarian assistance continued to prevent worse outcomes in Guban Pastoral and northwestern Northern Inland Pastoral (NIP) livelihood zones, where Crisis! (IPC Phase 3!) and Stressed! (IPC Phase 2!) outcomes persist, respectively. Northwest Agropastoral and most IDP settlements are also in Crisis (IPC Phase 3). • Contrary to earlier forecasts, Deyr seasonal rainfall is now expected to be below-average despite the development of a weak El Niño. Overall, favorable soil moisture is anticipated to prevent large declines in Deyr crop production and rangeland resources, and current outcomes are likely to be sustained in most livelihood zones through May 2019. In Addun Pastoral, Coastal Deeh Pastoral and Fishing, and northeastern NIP livelihood zones, however, deterioration in pasture and water resources is likely to lead to Crisis (IPC Phase 3) outcomes during Source: FEWS NET and FSNAU FEWS NET and FSNAU classification is IPC-compatible. IPC- the 2019 pastoral lean season. compatible analysis follows key IPC protocols but does not necessarily reflect a consensus of national food security partners. • In the absence of food assistance, deterioration to Emergency (IPC Phase 4) in Guban Pastoral livelihood zone and to Crisis (IPC Phase 3) in northwestern NIP livelihood zone is likely. -

Enhanced Enrolment of Pastoralists in the Implementation and Evaluation of the UNICEF-FAO-WFP Resilience Strategy in Somalia
Enhanced enrolment of pastoralists in the implementation and evaluation of the UNICEF-FAO-WFP Resilience Strategy in Somalia Prepared for UNICEF Eastern and Southern Africa Regional Office (ESARO) by Esther Schelling, Swiss Tropical and Public Health Institute UNICEF ESARO JUNE 2013 Enhanced enrolment of pastoralists in the implementation and evaluation of UNICEF-FAO-WFP Resilience Strategy in Somalia © United Nations Children's Fund (UNICEF), Nairobi, 2013 UNICEF Eastern and Southern Africa Regional Office (ESARO) PO Box 44145-00100 GPO Nairobi June 2013 The report was prepared for UNICEF Eastern and Southern Africa Regional Office (ESARO) by Esther Schelling, Swiss Tropical and Public Health Institute. The contents of this report do not necessarily reflect the policies or the views of UNICEF. The text has not been edited to official publication standards and UNICEF accepts no responsibility for errors. The designations in this publication do not imply an opinion on legal status of any country or territory, or of its authorities, or the delimitation of frontiers. For further information, please contact: Esther Schelling, Swiss Tropical and Public Health Institute, University of Basel: [email protected] Eugenie Reidy, UNICEF ESARO: [email protected] Dorothee Klaus, UNICEF ESARO: [email protected] Cover photograph © UNICEF/NYHQ2009-2301/Kate Holt 2 Table of Contents Foreword ........................................................................................................................................................................... -

Protection Cluster Update Weekly Report
Protection Cluster Update Funded by: The People of Japan Weeklyhttp://www.shabelle.net/article.php?id=4297 Report 23 th September 2011 European Commission IASC Somalia •Objective Protection Monitoring Network (PMN) Humanitarian Aid This update provides information on the protection environment in Somalia, including apparent violations of Human Rights and International Humanitarian Law as reported during the last two weeks through the IASC Somalia Protection Cluster monitoring systems. Incidents mentioned in this report are not exhaustive. They are intended to highlight credible reports in order to inform and prompt programming and advocacy initiatives by the humanitarian community and national authorities. General Overview Heavy fighting in southern regions between Al Shabaab and Transitional Federal Government (TFG) has led to heightened protection concerns throughout the reporting period. In Ceel Waaq, 43 people were killed and almost 80 wounded and an unknown number displaced following fighting between the TFG and Al Shabaab forces.1 The civilian population continues to face insecurity due to the ongoing conflict compounded by limited access to basic services and humanitarian support. In other regions, the famine has continued to take its toll on the Somali population. This week the United Nations Children Fund (UNICEF) stated that Somalia has the worst international mortality rate for children. 2 Furthermore, local sources in the district of Eldher town, Galgaduud region reported that 30 people had died as a result of starvation and -

Somalia Country Programme Evaluation – 2018 - 2020
Map of Somalia1 Evaluation Team Name Position / Thematic Areas Moses Lusih Team Leader/ Population Dynamics Kalid Mohamed Sexual and Reproductive Health and Rights Ibrahim Mohamed Adolescents and Youth Jane Kiragu Gender Equality and Women‟s Empowerment 1 The boundaries and names shown and the designations used on the maps on this site do not imply official endorsement or acceptance by the United Nations Population Fund. Somalia Country Programme Evaluation – 2018 - 2020 Acknowledgement The Evaluation Team wishes to thank UNFPA for the opportunity to successfully undertake the Somalia third Country Programme Evaluation. We are particularly grateful to the UNFPA Somalia staff members who, despite other pressing commitments in their responsibilities, were so responsive and gave us all the support that we needed to accomplish our work. We appreciate the CO leadership, led by the Country Representative, Anders Thomsen and his deputy, Walter Mendonca-Filho for their support and contribution to the successful implementation of the CPE. We particularly recognize the invaluable support of the M & E Specialist, Dr. Haider Rasheed and Ms. Stephanie Mugure for successful field coordination and facilitation of our virtual interview sessions, respectively; as well as the ASRO M&E Adviser, Dr. Olugbemiga Adelakin for the invaluable support and guidance during the CPE. We appreciate the participation of members of the Evaluation Reference Group, especially those who took time to provide comments towards improving the quality of the CPE design and report. We would also like to acknowledge the contributions made by the UNFPA CO staff and stakeholders, without whom the CPE would not have been successful. The information provided, despite other commitments, was very useful in enriching this report and providing feedback to the CO. -

HARAAD REEB (Quenching the Thirst) II FINAL REPORT October 2013
HARAAD REEB (Quenching the Thirst) II FINAL REPORT October 2013 – April 2016 1 Figure1: Girls are now happy to fetch water a kiosks that located closer to their homes 2 3 Project Title Haraad Reeb- Quenching the Thirst II Contract No 2013.1822.9 Report Title Interim Final report Project Period Oct- 2013-April 2016 (1/10/2013-31/04/2016) Recipient Organisation CARE Germany Local Counterpart CARE Somalia Country office Contents` TERMS AND ACRONYMS ................................................................................................ 63 I. INTRODUCTION .......................................................................................................... 94 II. BACKGROUND ......................................................................................................... 105 III. SUMMARY…………………………………………………………………………………………7 III.IMPLEMENTATION ................................................................................................. 128 IV. IMPACT ................................................................................................................... 2318 V. APPRAISAL OF IMPLEMENTED ACTIVITIES ................................................ 5752 ANNEX1: ANNUAL WORK PLAN ............................................................................ 6359 4 5 TERMS AND ACRONYMS ACD Assistant Country Director AM Area Manager Berked Under ground water harvesting storage BH Borehole CAAC Catchment Area Advisory Committee CD Country Director CFW Cash for Work CLTS Community Led Total Sanitation DFID Department for -

AWDAL REGION - Borama District
p AWDAL REGION - Borama District 42°45'E 43°0'E 43°15'E N N ' ' 0 0 3 3 ° ° 0 0 1 LUGHAYE 1 ZEYLAC Ali Gala(P28-001) ! Dabo Dilaac(Q28-001) ! Fiqi Aadan(R27-001) ! Caro-Wareen(R30-001) ! Xariirad(S19-001) ! Ceel Dacar Jif(S26-001) Fadhi Aroor-Seel(S20-001) Baxay(S22-001) Budhuq(S24-001) ! ! ! ! Fadhiwanag(S29-002) Xun(S29-001) Dhagaxa ! ! Gor Madow(T27-001) Ali-Heley(T27-002) Dhoobo(T28-002) Goray(T25-001) ! ! ! Baki ! (!! Weeraar(T28-001) ! N Darya N ' ' 5 Dheere(T20-001) 5 ! 1 1 ° ° 0 Dix-Gudban(U24-001) BORAMA 0 Gargoorey(U24-002) !! 1 1 Xalimaale(V25-001) ! Boon(V24-001) ! Badanbed(V28-001) ! Hagoogane(V30-001) ! Daray Culaacule(W23-002) !Beden ! Quruxsan(W28-001) Cabaasa(W23-003) Bed(W28-002) Dhidhiid(W23-001) ! Abaase ! Dhadheer(W27-001) ! Abasse ! Xamarta Gaagaab(X27-002) ! Cabaasa(X28-001) Dur-Dur Cad(X30-001) BAKI ! Qolqol(X24-001) Cadaad(X27-001) ! ! Wanbarta ! Ciye(X25-002) Quljed(X23-001) ! ! Qolqol(X25-001) ! Cara-Cad(Y24-002) Cadaad(Y28-001) !! Dibriyo Maleh Xeego(Y28-002) Hego (Maraaley)(Y24-003) Jirjir(Y24-001) ! Baki(Y28-003) Nadhi(Y27-001) Maraalay, ! Shakal(Y30-001) !Abakor Maraaley(Z23-001) Cadaawe(Z30-001) ! ! Taw Sheikh Tawle(Z27-001) ! Huways(Z25-001) Dibrio N ! Ando N ' Meleh(Z26-001) ' 0 ! Bait(A28-001) 0 ° ! ° 0 0 1 Fulin-Fulka(A25-002) 1 ! Dagmo!-Laqas(A24-001) ! Sattawa(A25-001) Cara-Ga!ranug(A26-001) ! ! ! Daray-Macaane(A27-001) Tuur-Qaylo(A26-002) ! Tawtawle(A27-002) Fa!dhi-Cad(A28-002) ! Waraabe Dhammuug(B27-004) Fadhi ! ! Camuud(B27-001) Dareeray(B26-001) ! Xun(A29-001) Xasan ! Badhiile(B25!-004) Sog-Sogley(B25-003) -

S.No Region Districts 1 Awdal Region Baki
S.No Region Districts 1 Awdal Region Baki District 2 Awdal Region Borama District 3 Awdal Region Lughaya District 4 Awdal Region Zeila District 5 Bakool Region El Barde District 6 Bakool Region Hudur District 7 Bakool Region Rabdhure District 8 Bakool Region Tiyeglow District 9 Bakool Region Wajid District 10 Banaadir Region Abdiaziz District 11 Banaadir Region Bondhere District 12 Banaadir Region Daynile District 13 Banaadir Region Dharkenley District 14 Banaadir Region Hamar Jajab District 15 Banaadir Region Hamar Weyne District 16 Banaadir Region Hodan District 17 Banaadir Region Hawle Wadag District 18 Banaadir Region Huriwa District 19 Banaadir Region Karan District 20 Banaadir Region Shibis District 21 Banaadir Region Shangani District 22 Banaadir Region Waberi District 23 Banaadir Region Wadajir District 24 Banaadir Region Wardhigley District 25 Banaadir Region Yaqshid District 26 Bari Region Bayla District 27 Bari Region Bosaso District 28 Bari Region Alula District 29 Bari Region Iskushuban District 30 Bari Region Qandala District 31 Bari Region Ufayn District 32 Bari Region Qardho District 33 Bay Region Baidoa District 34 Bay Region Burhakaba District 35 Bay Region Dinsoor District 36 Bay Region Qasahdhere District 37 Galguduud Region Abudwaq District 38 Galguduud Region Adado District 39 Galguduud Region Dhusa Mareb District 40 Galguduud Region El Buur District 41 Galguduud Region El Dher District 42 Gedo Region Bardera District 43 Gedo Region Beled Hawo District www.downloadexcelfiles.com 44 Gedo Region El Wak District 45 Gedo -

FSNAU Monthly Brief
NO 11 : ISSUED NOVEMBER 2002 OCTOBER REPORT FSAU acknowledges the contribution of key partners FEWS NET, CARE, WFP, SC-UK, UNCU, UNDP FSAU REPORTS AND ACTIVITIES HIGHLIGHTS Gedo Region : The nutritional improvements seen in a recent survey conducted in Belet Hawa district are closely attributed to the level of relief food interventions. ** The FSAU FOCUS “2002 Gu Season However, the difficulty of recording changing population figures, mortality rates and and Food Security Implications” will be population movements continues to present obstacles in estimating future needs and disseminated via e-mail and distributed interventions. to FSAU users in mid-November. Copies Food Security in Sool Plateau Improves : There has been erratic and patchy will also be available at FSAU offices rainfall on the Sool Plateau, however, FSAU Field Monitors’ report that berkads are from [email protected] almost full so poorer pastoralist households are not having to spend large amounts of their income on the purchase of water. There has also been some improvement in **The field work for the FSAU Belet pasture. However there are still pockets (Sool of Eastern Sanag and Sool of Taleh Hawa Nutrition Survey with partners was district) which didn’t receive rain and these need to be monitored closely in the coming carried out between 18-24 October months. 2002. Preliminary information and Heavy Rains Fall in Belet Weyne (Hiran Region): Heavy rain fell throughout analysis is available in the October Issue Belet Weyne district between 21—27 October. This has enabled farmers to plant their of Nutrition Update. crops. Pasture has recovered. -
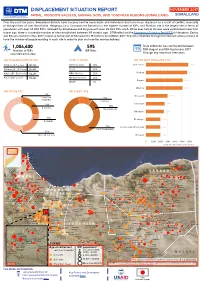
Somaliland Displacement Profile November 2017.Pdf
DISPLACEMENT SITUATION REPORT NOVEMBER 2017 AWDAL, WOQOOYI GALBEED, SANAAG, SOOL AND TOGDHEER REGIONS (SOMALILAND) SOMALILANDSOMALIA Over the past few years, Somaliland districts have become host to households and individuals that have been displaced as a result of conflict, insecurity or drought from all over Somaliland. Hargeysa, Laas Caanood and Borama has the highest number of IDPs, and Stadium site is the largest site in terms of population with over 34,000 IDPs, followed by Statehouse and Erigavo with over 25,000 IDPs each. While over half of all sites were established more than a year ago, there is a sizeable number of sites established between 1-9 months ago . DTM rolled out the Emergency Tracking Tool (ETT) in Hargeysa, Zeylac and Borama district in May 2017 scaled up to the rest of Somaliland’s 19 districts by October 2017. The data collected through this tool will allow partners to have the number of people residing in each site in order to plan and monitor service delivery. 1,004,400 595 Data collection was conducted between Number of IDPs IDP Sites 18th August and 18th September 2017 (rounded estimates) through key informant interviews AGE DISAGGREGATION OF IDPS PRIORITY NEEDS TOP TEN MOST POPULATED SITES * Children (0-5 years) 181,916 Drinking water 18% Children (6 - 18 Years) 269,431 Food 30% Adults (18 - 59 Years) 342,206 NFIs /Shelter 21% Elders (60+ years) 102,442 Medical services 24% WASH 7% AGE OF THE SITE IDP SITE BY TYPE 2% Less than 13% 3 months Planned 23% 10% 6 months Spontaneous 24% 9 months 77% Host Community -

“Breaking the Localisation Deadlock”
“Breaking the localisation deadlock” Review of Humanitarian Capacities, Power Relations and Localisation in the Somali Humanitarian System Author: Fernando Almansa (consultant) Copyright: 2020 Breaking the localisation deadlock | 2020 Contents EXECUTIVE SUMMARY 5 1. CONTEXT AND PURPOSE OF THE HUMANITARIAN CAPACITY REVIEW 9 2. APPROACH AND METHODOLOGY 9 3. HUMANITARIAN ACTORS AND THEIR TYPOLOGY 10 4. HUMANITARIAN CONTEXT AND VULNERABILITY IN SOMALIA AND SOMALILAND 15 5. HUMANITARIAN CAPACITY IN SOMALIA AND SOMALILAND 17 5.1. OVERALL GLOBAL CONTEXT CAPACITIES IN SOMALIA AND SOMALILAND 17 5.2 SOMALI NON-GOVERNMENTAL ORGANISATIONS HUMANITARIAN CAPACITIES 22 5.2.1 Somalia (South Central) Non-Governmental Organisations’ Humanitarian Capacities 22 5.2.2 Puntland Non-Governmental Organisations’ Humanitarian Capacities 28 5.2.3 Somaliland Non-Governmental Organisations’ Humanitarian Capacities 34 5.2.4 Overall Local Humanitarian NGOs 39 5.3 STATE INSTITUTIONS 42 5.3.1 Federal Government State institutions 42 5.3.2 Puntland State institutions 48 5.3.3 Somaliland State institutions 53 5.3.4 Overall state institutions 58 5.4 OVERALL ORGANISATIONAL HUMANITARIAN CAPACITIES 58 5.5 GENDER ANALYSIS OF ORGANISATIONAL HUMANITARIAN CAPACITIES 59 6 ORGANISATIONAL RELATIONS AND POWER ANALYSIS 62 7. SOMALIA’S HUMANITARIAN LOCALISATION AGENDA: OPPORTUNITIES AND BARRIERS 66 8. UPDATED SOMALIA AND SOMALILAND HUMANITARIAN PROFILE 72 9. RECOMMENDATIONS 74 ANNEX 1 INTERVIEWEES 78 ANNEX 2 METHODOLOGY 78 3 Breaking the localisation deadlock | 2020 Acronyms ANSA Armed