Somalia Country Programme Evaluation – 2018 - 2020
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Somalia General
SOMALIA GENERAL . UN-Habitat is active in all the Somali regions with a current portfolio of approximately USD 40 million. UN-Habitat Somalia Program which is delivered in post-conflict Somalia, clearly fits into the UN-Habitat Risk Reduction and Rehabilitation sub-program. However, program activities can be nicely placed in almost any of UN-Habitat’s sub-programs. There is a renewed focus on Mogadishu with presently two projects running. Politically advocated but not yet practical re-location to Mogadishu will be linked to new programme recruitments. Presently, UN-Habitat has a small presence in Mogadishu through national staff and international consultants and constant missions by international staff. Existing and well established field offices are in Garowe, Bossaso (Puntland), and Hargeisa (Somaliland). Excellent cooperation exists with all Somali Administrations at central and local levels. UN-Habitat is an active member of the UN Country Team and works in support of the New Deal and the Somalia Governments Six-point Programme. JPLG, UN-Habitat Mandate implemented in Somalia Joint Programme on Local Governance & Decentralised Service Delivery Under this five-UN-Agency Joint Programme, UN-Habitat’s role covers activities which fit perfectly into its mandate: urban planning, land governance and legislation, municipal finance including GIS- based property taxation, solid waste management, and capacity building of local governments including personnel and physical infrastructure, Program delivers in all regions of Somalia, including Somaliland -
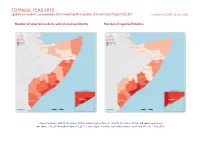
SOMALIA, YEAR 2019: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 22 June 2020
SOMALIA, YEAR 2019: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 22 June 2020 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; Ethiopia/Somalia bor- der status: CIA, 2014; incident data: ACLED, 13 June 2020; coastlines and inland waters: Smith and Wessel, 1 May 2015 SOMALIA, YEAR 2019: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 22 JUNE 2020 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Battles 1131 458 2154 Conflict incidents by category 2 Explosions / Remote 621 228 1221 Development of conflict incidents from 2010 to 2019 2 violence Violence against civilians 530 358 640 Methodology 3 Strategic developments 140 6 16 Conflict incidents per province 4 Protests 78 2 2 Riots 19 3 5 Localization of conflict incidents 4 Total 2519 1055 4038 Disclaimer 6 This table is based on data from ACLED (datasets used: ACLED, 13 June 2020). Development of conflict incidents from 2010 to 2019 This graph is based on data from ACLED (datasets used: ACLED, 13 June 2020). 2 SOMALIA, YEAR 2019: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 22 JUNE 2020 Methodology on what level of detail is reported. Thus, towns may represent the wider region in which an incident occured, or the provincial capital may be used if only the province The data used in this report was collected by the Armed Conflict Location & Event is known. -

Rethinking the Somali State
Rethinking the Somali State MPP Professional Paper In Partial Fulfillment of the Master of Public Policy Degree Requirements The Hubert H. Humphrey School of Public Affairs The University of Minnesota Aman H.D. Obsiye May 2017 Signature below of Paper Supervisor certifies successful completion of oral presentation and completion of final written version: _________________________________ ____________________ ___________________ Dr. Mary Curtin, Diplomat in Residence Date, oral presentation Date, paper completion Paper Supervisor ________________________________________ ___________________ Steven Andreasen, Lecturer Date Second Committee Member Signature of Second Committee Member, certifying successful completion of professional paper Table of Contents Introduction ........................................................................................................................... 3 Methodology .......................................................................................................................... 5 The Somali Clan System .......................................................................................................... 6 The Colonial Era ..................................................................................................................... 9 British Somaliland Protectorate ................................................................................................. 9 Somalia Italiana and the United Nations Trusteeship .............................................................. 14 Colonial -

Somalia Hunger Crisis Response.Indd
WORLD VISION SOMALIA HUNGER RESPONSE SITUATION REPORT 5 March 2017 RESPONSE HIGHLIGHTS 17,784 people received primary health care 66,256 people provided with KEY MESSAGES 24,150,700 litres of safe drinking water • Drought has led to increased displacement education. In Somaliland more than 118 of people in Somalia. In February 2017 schools were closed as a result of the alone, UNHCR estimates that up to looming famine. 121,000 people were displaced. • Urgent action at this stage has a high • There is a sharp increase in the number of chance of saving over 300,000 children Acute Water Diarrhoea (AWD/cholera) who are acutely malnourished as well cases. From January to March, 875 AWD as over 6 million people facing possible cases and 78 deaths were recorded in starvation across the country. 22,644 Puntland, Somaliland and Jubaland. • Despite encouraging donor contributions, • There is an urgent need to scale up the Somalia humanitarian operational people provided with support for health interventions in the plan is less than 20% funded (UNOCHA, South West State (SWS) especially FTS, 7th March 2017). Approximately 5,917 in districts that have been hard hit by US$825 million is required to reach 5.5 NFI kits outbreaks of Acute Watery Diarrhoea million Somalis facing possible famine until (AWD). Only few agencies have funding June 2017. to support access to health care services. • More than 6 million people or over 50% • According to Somaliland MOH, high of Somalia’s population remain in crisis cases of measles, diarrhea and pneumonia and face possible famine if aid does not have been reported since November as match the scale of need between now main health complications caused by the and June 2017. -

SOMALIA Food Security Outlook October 2018 to May 2019
SOMALIA Food Security Outlook October 2018 to May 2019 Deyr rainfall expected to sustain current outcomes, except in some pastoral areas KEY MESSAGES Current food security outcomes, October 2018 • Food security has continued to improve throughout Somalia since the 2018 Gu. Most northern and central livelihood zones are Stressed (IPC Phase 2), while southern livelihood zones are Minimal (IPC Phase 1) or Stressed (IPC Phase 2). In October, humanitarian assistance continued to prevent worse outcomes in Guban Pastoral and northwestern Northern Inland Pastoral (NIP) livelihood zones, where Crisis! (IPC Phase 3!) and Stressed! (IPC Phase 2!) outcomes persist, respectively. Northwest Agropastoral and most IDP settlements are also in Crisis (IPC Phase 3). • Contrary to earlier forecasts, Deyr seasonal rainfall is now expected to be below-average despite the development of a weak El Niño. Overall, favorable soil moisture is anticipated to prevent large declines in Deyr crop production and rangeland resources, and current outcomes are likely to be sustained in most livelihood zones through May 2019. In Addun Pastoral, Coastal Deeh Pastoral and Fishing, and northeastern NIP livelihood zones, however, deterioration in pasture and water resources is likely to lead to Crisis (IPC Phase 3) outcomes during Source: FEWS NET and FSNAU FEWS NET and FSNAU classification is IPC-compatible. IPC- the 2019 pastoral lean season. compatible analysis follows key IPC protocols but does not necessarily reflect a consensus of national food security partners. • In the absence of food assistance, deterioration to Emergency (IPC Phase 4) in Guban Pastoral livelihood zone and to Crisis (IPC Phase 3) in northwestern NIP livelihood zone is likely. -

Somalia (Puntland & Somaliland)
United Nations Development Programme GENDER EQUALITY AND WOMEN’S EMPOWERMENT IN PUBLIC ADMINISTRATION SOMALIA (PUNTLAND & SOMALILAND) CASE STUDY TABLE OF CONTENTS KEY FACTS .................................................................................................................................. 2 ACKNOWLEDGEMENTS ............................................................................................................ 3 EXECUTIVE SUMMARY.............................................................................................................. 4 METHODOLOGY ........................................................................................................................ 6 CONTEXT .................................................................................................................................... 7 Socio-economic and political context .............................................................................................. 7 Gender equality context....................................................................................................................... 8 Public administration context .......................................................................................................... 12 WOMEN’S PARTICIPATION IN PUBLIC ADMINISTRATION .................................................16 POLICY AND IMPLEMENTATION REVIEW ............................................................................18 Post-Conflict Reconstruction and Development Programme ................................................ -

Galkayo Urban Baseline Profile
L I V E L I H OLivelihood O D Baseline Profile - Galkayo Urban FSNAU BASELINE Food Security and Nutrition Analysis Unit - Somalia P R O F I L E Issued October, 2010 Galkayo Urban HISTORICAL TIMELINE GALKAYO AND SURROUNDING LiVELIHOOD ZONES GALKAYO HISTORICAL TIMELINE 2005-2009 Food DJIBOUTI Awdal Sanag Year Security Events, Effects, and Reponses Woq. Galbeed Bari Ranking Togdheer Sool Below Average Year: Prolonged Nugal drought; influx of IDPs; decline of food prices; influx of destitute pastoralists; Jariban Mudug Goldogob Galgadud political problems in southern Galkayo Bakol Galkayo Hiran (split of Galmudug); Improved security GAALKACYO Gedo 2009 2 situation compared to previous M. Shabelle Bay conflicts between the North and Banadir L. Shabelle South Galkayo, despite of organized Juba and targeted killings in the reference year.; replacement of CARE by WFP and 50% reduction of food aid. Food Security and Nutrition Analysis Unit - Somalia http://www.fsnau.org P.O. Box 1230 Village Market, Nairobi, Kenya Email: [email protected] tel: 254-20-4000000 fax:254-20-4000555 FSNAU is managed by FAO The boundaries and names on these maps do not imply official endorsement or acceptance by the United Nations. Below Average Year: Drought; The regional & District boundaries reflect those endorsed by the Government of the Republic of Somalia in 1986. insecurity/piracy; inflation; food aid; influx of rural destitute and Hobyo 2008 2 ensuing tensions; suspension of CARE activities; lifting of roadblocks; establishment of IRC office in Galkayo; high food prices. Bad Year: Drought; inflation; insecurity; IDPs influx; water shortage and water trucking from Addun Pastoral: Mixed sheep & goats, camel 2007 2 Belet Weyne; high water price; Awdal border & coastal towns: Petty trading, fishing, salt mining printing of Somali bank note; poor purchasing power; expansion of Central regions Agro-Pastoral: Cowpea, sheep & goats, camel, cattle town; and increased social services. -

Nutrition Update’
NUTRITION UPDATE N U FOR Food Security Assessment Food and Agriculture Unit for Somalia SOMALIA Organisation [email protected] April 2001 NUTRITION ISSUES IN SOMALIA While the effects of the ‘livestock ban’ are undoubtedly having a negative effect on the economy of Somaliland and Puntland, there has been no evidence so far of deterioration in the nutritional status of the population. So far little qualitative information is available from the populations most likely to be affected i.e. the poor in urban areas, the displaced and the poor/very poor pastoralists. There is however, some reluctance among parties involved with these groups to undertake nutrition surveys although some are now considering the idea. Because organisations often undertake nutrition surveys only when malnutrition is already evident, surveys in Somalia are strongly associated with subsequent food aid; indeed the interest in undertaking nutrition surveys has diminished considerably since the food security situation in south and central Somalia has improved over the past six months or so. As a result of this, we have inadequate information on what ‘normal’ levels of malnutrition are in the various populations and will continue to have difficulty in interpreting malnutrition rates produced in times of crisis. FSAU nutritionists and food security specialists are willing to provide technical support to any organisation or government authority wishing to undertake a nutrition survey, as in the recent survey in Jamame. In response to comments and requests from readers, sections that provide general information on issues affecting nutrition in Somalia and BOSSASO DJIBOUTI â similar countries have been expanded while Had aaftimo AWDAL LUGHAYE â CEERI GAABO Ú Ú BER BERA Ú Badh an â ISKUSH UBAN maintaining reports on specific Boon ÚGarga ara GALBEED SANAG Ú â Huddisa BOROMA Ú Dacarb udhu g âÚ CÚEEL AFWEYN BARI GEBIL EY Ú SHEIKH DHARAR â Ú geographical areas. -

Puntland Sub-National Food Security Cluster Meeting
Puntland Sub-National Food Security Cluster Meeting 26th November 2014 SOMALIA Agenda • Introduction • Security updates and partner contribution • Presentation of summary district level information by response objective and review of gaps per district August 2013 • AOB SOMALIA Access Constraints & Implications on Operations To be completed for every meeting SOMALIA Review of FSC Responses for Puntland (October 2014) SOMALIA Cluster Members Responses by Response Priority Region Improved Access To Livelihood Safety Net Responses Food Investment No. of No. of No. of No. of No. of No. of beneficiaries partners who beneficiaries partners who beneficiaries partners who Reached Reported Reached Reported Reached Reported Bari 750 1 44,766 3 13,767 1 Nugaal 0 0 21,222 1 11,120 1 Sool 0 0 11,394 2 10,618 1 Sanaag 750 1 26,988 2 11,201 1 Mudug 0 0 36,558 3 14,303 1 Togdheer 0 0 1,956 2 7,660 SOMALIA1 District Level Response Improved Access to Food Activity Breakdown(1/2) – Planned and Actual – Emergency Relief Assistance Region District Cash (Food/Cash/Voucher Planned Actual Bari Aluula 0 0 Bender Beila 900 300 Bossaso 7,500 0 Gardo 450 450 Iskushuban 0 0 Qandala 0 0 Burtinle Nugaal 0 0 Eyl 0 0 Garowe 900 0 SOMALIA District Level Response Improved Access to Food Activity Breakdown(2/2) – Planned and Actual – Emergency Relief Assistance Region District (Food/Cash/ Voucher) Planned Actual Sanaag Badhan 2,970 552 El Afwein 0 0 Erigavo 198 198 Sool Caynabo 0 0 Lasanod 23,880 0 Taleh 0 0 Xudun 0 0 Mudug Galdogob 0 0 Galkayo 0 0 Jariban 0 0 Togdheer Buhodle -

Somalia Nutrition Cluster Geo-Tagging: Capacity Assessment
Somalia Nutrition Cluster Geo-tagging: Capacity Assessment Somalia Nutrition Cluster Geo-tagging: Capacity Assessment This report was written by Forcier Consulting for the Somali Nutrition Cluster. About the Somali Nutrition Cluster The Somali Nutrition Cluster (SNC) has been operational in Somalia since 2006, following the United Nation’s Humanitarian Country Team (HCT) recommendations of activating the cluster system to effectively coordinate the humanitarian partner’ work. The vision of SNC is to safeguard and improve the nutritional status of emergency-affected populations in Somalia. Led by UNICEF, the SNC consists of a network of about 100 part- ners, 80 per cent of which are national NGOs, mostly based in central and southern regions of Somalia. Its core purpose is to enable cluster-wide stakeholders and sub-national coordination mechanisms to have all the necessary capacity to achieve timely, quality and appropriate nutrition responses to emergencies. Twitter: @Nutrition_Som About Forcier Consulting Forcier Consulting was founded in response to the overwhelming demand for data, research and information in some of the most challenging environments in Africa. While we aim to produce reliable and high-quality research in these complex settings, we also make long-term invest- ments in building the capacity of national staff to serve as researchers and consultants. www.forcierconsulting.com/ Legal Notice and Disclaimer All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means with- out prior approval in writing from Forcier Consulting and the Somalia Nutrition Cluster. This report is not a legally binding document. -

Galkayo 1 Liegt Die Stadt Galkayo in Puntland Oder in Zent
Schnellrecherche der SFH-Länderanalyse vom 23. Juli 2015 zu Somalia: Galkayo Fragen an die SFH-Länderanalyse: Liegt die Stadt Galkayo in Puntland oder in Zentralsomalia? Wie ist die Sicherheitssituation in Galkayo? Die Informationen beruhen auf einer zeitlich begrenzten Recherche (Schnellrecher- che) in öffentlich zugänglichen Dokumenten, die uns derzeit zur Verfügung stehen. 1 Liegt die Stadt Galkayo in Puntland oder in Zentralsomalia? Galkayo ist eine zweigeteilte Stadt. In einem Addendum zu den UN High Commis- sioner for Refugees (UNHCR) Eligibility Guidelines aus dem Jahr 2010 stellte UNHCR im März 2012 klar, dass Galkayo eine zweigeteilte Stadt ist. Der Norden steht unter der Verwaltung von Puntland. Der Süden steht unter der Kontrolle der Verwaltung von Galmudug. Galkayo liegt zudem an der Grenze zwischen zwei grossen Klans, den Darod im Nor- den und den Hawiye im Süden. Der lokale Darod Klan ist der Majerteen Klan mit dem Omar Mohamud Sub-Klan. Der grösste lokale Hawiye Klan ist der Sa’ad Klan. UNHCR, März 2012: «With this Addendum, UNHCR provides further information on the city of Galkacyo (also referred to as Gaalkacyo, Galkayo, Galcayo, Galcaio). It should be considered as complementing the 2010 Somalia Eligibility Guidelines, which remain valid. This Addendum clarifies that the city of Galkacyo is a divided city, with two distinct, separate parts falling under two different geographical, political and administra- tive entities, which the original Guidelines did not say. Only in this regard does this Addendum affect the text of the 2010 Somalia Eligibility Guidelines. The current situation in the city of Galkacyo 3. The Mudug region lies at the heart of Somalia, bordered by Nugal to the north, Galgadud to the south, Ethiopia to the west and the Indian Ocean to the east. -

Situation Report 10- Somalia Hunger Crisis Response.Pdf
WORLD VISION SOMALIA HUNGER RESPONSE SITUATION REPORT No. 10 6 JULY 2017 SITUATION HIGHLIGHTS 6.7 million people in need of humanitarian and protection services 4 million children are in need of humanitarian assistance KEY MESSAGES • Worsening situation for children: • Health crisis: Access to water, $ 37M The humanitarian situation in Somalia sanitation and hygiene (WASH) required by World Vision for continues to deteriorate with an remains a challenge with over 4.5 humanitarian assistance estimated 4 million children in million people estimated to be in urgent need of assistance (UNICEF, need. Lack of these basic commodities June 2017). A recent assessment and services have led to major disease from FSNAU-FEWSNET indicates outbreaks with 53,015 cases of Acute an elevated risk of famine due to a Watery Diarrhoea (AWD) / Cholera combination of severe food insecurity, recorded since January 2017. Out of high acute malnutrition and high these 53% are children under age 5. 4.5 million disease burden (FSNAU/ FEWS NET, • Displaced by drought: More than people in need of water, 29th May 2017). 739,000 people, including 480,000 sanitation and hygiene services • Acute Malnutrition critical: Acute children, have been displaced due malnutrition levels remain critical, to drought since November 2016. particularly among the rural pastoralist Baidoa and Mogadishu have the population as well as Internally highest number of IDPs. Displaced Persons (IDPs). • Ongoing response: World Vision • Half the country’s population in urgent has assisted 380,596 people in need: Despite the rains in some parts drought-affected areas of Somaliland, 363,000 of Somalia, over 6.7 million people, Puntland, Jubaland and South West children under-5 are acutely more than half of the population, State since January 2017.