Public Governing Body Papers 12 July 2016
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Council Tax Setting and Statutory Resolutions 2020/21 PDF 270 KB
Report ____________________________________________________________________ To the Chair and Members of Date: 5th March 2020 Council COUNCIL TAX SETTING AND STATUTORY RESOLUTIONS 2020/21 EXECUTIVE SUMMARY 1. This report sets out how the Council Tax is calculated and makes recommendations regarding Doncaster’s Council Tax requirement for 2020/21. 2. It is proposed that Doncaster Council’s element of the Band D Council Tax charge is increased by 3.99% (1.99% Council Tax increase and a further 2.00% increase through the Government`s Social Care precept) to £1,405.35 (£936.90 for a Band A). 3. The overall increase will mean an additional £53.92 for Band D Council Tax per annum, £1.04 per week (£35.95 for Band A per annum, £0.69 per week). EXEMPT REPORT 4. Not applicable. RECOMMENDATIONS 5. Council is requested to approve a Band D Council Tax for 2020/21 of £1,405.35 for Doncaster Council services. Council is also requested to pass the appropriate Statutory Resolutions, as set out and recommended at Appendix B, which incorporate the Council Taxes of the Joint Authorities and which, taken together with Doncaster's 3.99% increase, represent a 3.66% increase from the 2019/20 Council Tax for Doncaster residents. WHAT DOES THIS MEAN FOR THE CITIZENS OF DONCASTER? 6. The citizens of Doncaster can expect to see their Council Tax for Council services increase by 3.99%. The Police and Fire increases are 2.00% and 1.99% respectively, making an overall increase of 3.66% (see table at paragraph 22). 7. The average Parish Council Tax across the whole Doncaster Council area has increased by 3.11%. -
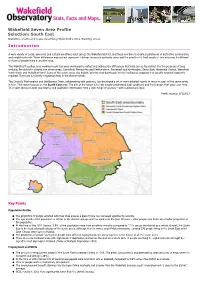
South East Statistics, Charts and Maps Describing Wakefield's Area Working Areas
InstantAtlas™ Server 6 Wakefield Seven Area Profile Selection: South East Statistics, charts and maps describing Wakefield's Area Working areas. Introduction A wide variety of social, economic and cultural conditions exist across the Wakefield district, and these combine to create a patchwork of distinctive communities and neighbourhoods. These differences may prompt agencies to deliver services in particular ways and the priorities for local people in one area may be different to those of people living in another area. The Wakefield Together area working model has been developed to reflect and address the differences that exist across the district. For the purposes of area working, the district is divided into seven areas: Castleford; Normanton and Featherstone; Pontefract and Knottingley; South East; Wakefield Central; Wakefield North West; and Wakefield Rural. Some of the seven areas also include ‘priority neighbourhoods’ where intelligence suggests that specific targeted support is required. There are 12 priority neighbourhoods in the district overall. The Council’s Performance and Intelligence Team, collaborating with partners, has developed a set of more detailed reports to focus on each of the seven areas in turn. This report focuses on the South East area. The aim of the report is to help people understand local conditions and the changes that occur over time. The report draws on both quantitative and qualitative information from a wide range of sources – both national and local. Profile created: 9/1/2017 Key Points Population Profile The proportion of people satisfied with their local area as a place to live has increased significantly recently. The age profile of the population is similar to the district average and has aged over the past 10 years - older people now make up a higher proportion of the population. -

The Pennine Lower and Middle Coal Measures Formations of the Barnsley District
The Pennine Lower and Middle Coal Measures formations of the Barnsley district Geology & Landscape Southern Britain Programme Internal Report IR/06/135 BRITISH GEOLOGICAL SURVEY GEOLOGY & LANDSCAPE SOUTHERN BRITAIN PROGRAMME INTERNAL REPORT IR/06/135 The Pennine Lower and Middle Coal Measures formations of the Barnsley district The National Grid and other R D Lake Ordnance Survey data are used with the permission of the Controller of Her Majesty’s Stationery Office. Editor Licence No: 100017897/2005. E Hough Keywords Pennine Lower Coal Measures Formation; Pennine Middle Coal Measures Formation; Barnsley; Pennines. Bibliographical reference R D LAKE & E HOUGH (EDITOR).. 2006. The Pennine Lower and Middle Coal Measures formations of the Barnsley district. British Geological Survey Internal Report,IR/06/135. 47pp. Copyright in materials derived from the British Geological Survey’s work is owned by the Natural Environment Research Council (NERC) and/or the authority that commissioned the work. You may not copy or adapt this publication without first obtaining permission. Contact the BGS Intellectual Property Rights Section, British Geological Survey, Keyworth, e-mail [email protected]. You may quote extracts of a reasonable length without prior permission, provided a full acknowledgement is given of the source of the extract. Maps and diagrams in this book use topography based on Ordnance Survey mapping. © NERC 2006. All rights reserved Keyworth, Nottingham British Geological Survey 2006 BRITISH GEOLOGICAL SURVEY The full range of Survey publications is available from the BGS British Geological Survey offices Sales Desks at Nottingham, Edinburgh and London; see contact details below or shop online at www.geologyshop.com Keyworth, Nottingham NG12 5GG The London Information Office also maintains a reference 0115-936 3241 Fax 0115-936 3488 collection of BGS publications including maps for consultation. -

Otc Medicines Independent Report Prepared by Standout Media Limited for South Yorkshire and Bassetlaw Ics
OTC MEDICINES INDEPENDENT REPORT PREPARED BY STANDOUT MEDIA LIMITED FOR SOUTH YORKSHIRE AND BASSETLAW ICS DECEMBER 2018 2 OTC MEDICINES INDEPENDENT REPORT Contents Introduction and purpose 3 About the South Yorkshire and Bassetlaw area and its population 4 Who was involved? 5 About the insight and engagement campaign 6 Who were our target audiences? 7 Methodology 7 Toolkits 9 About the people who engaged with us 11 Patient and public survey 14 What did the patients and public tell us? 16 Staff engagement 19 Community engagement 21 Social media 22 Website statistics 24 How our insight campaign compares 26 What we propose – next steps 27 Awards 29 Appendices Appendix 1 – SYB ICS partner organisations 30 Appendix 2 – Rotherham CCG Start Well, Choose Well, Stay Well campaign assets 32 Appendix 3 – SYB ICS Citizens’ Panel 33 Appendix 4 – Patient and public survey results in graphs 34 Appendix 5 – Prescriber survey results in graphs 41 Appendix 6 – Doncaster prescriber survey results 45 Appendix 7 – Barnsley consultation report 67 Appendix 8 – GP practices by CCG area 89 Appendix 9 – Community pharmacies by CCG area 95 Appendix 10 – Parish councils by CCG area 105 Appendix 11 – Libraries by CCG area 107 Appendix 12 – Community centres by CCG area 109 Appendix 13 – ONS data by CCG area 112 Appendix 14 – MPs by CCG area 117 Appendix 15 – Comms toolkit 118 3 OTC MEDICINES INDEPENDENT REPORT Introduction and purpose In early 2018 NHS England carried out a public consultation on reducing prescribing of over the counter (OTC) medicines for minor, short-term health concerns which could save the NHS high costs and encourage more people to self-care. -

Doncaster Cycling Map
6 A 6 N V T O 4 W 3 E B Bentley Moor E A R N H 2 E 8 L O Wood N R M E 2 C TH OA R D A OR D M N L IN W E I D E V S A N P L I V E BO E L EADO F T N IV O A M W IE S U R R N F H E E D T E H F V E L U R BE T E AR I Dunscroft M A R S L O UM EN O LO M L W V N O W C PA A NT A UTTERW R E RK G O L E N Y ORT T R W E Barnby Dun O R AV H UT U S Adwick D U D O A T EN L B Y R B U R AD A E M E WIC S IV A E K LA Common V T E C T NE E F N T A 9 H E U H V C PO 1 E S E A H N E C E R A AVE D I GTON I K T ENNIN R YN IN O K C L N U GSLE A I Y V Adwick Pk E T R E E B V L O N N D A A A A U LA Jun Sch A W D O C E K E L R K Barnby Dun Frickley OOD N E A R U V B E L W A A R T A E N E E S R E V T N A S N N A Common H V E R E C E H A Park Hill N U T A N F T A B D Playing Fields O SB U IN W D U E Almholme Hooton R Y SW Outwood IC A Grange AVENUE ADWICK K R 49 50 51 52 53 W54 55 56 57 Shaftholme 58 59 60 61 62 63 64 L M Town and country maps with hundreds of miles of routes E A A N Academy S N E T E N Grumble Hurst H Pagnell R H LA O I A O G N L R B LE STREET L M R G I OO P L S O T V O North Ridge L O E S O L R L E CLAYT U LAN V N A NE AN L ON L ALK H LA E E A ANE N GE B Community E R TPT SHAFT ME G PO ID E N HOL H C N R D R C D N O Q C E A E L E E A E Lound Hill L L X R S U E N A School T O S U K R RT E N 'S O D N L O T N M D G E A N O E A A S E B N ECT R V R Plantation R E O O N V S L V R ND U O O U L O R O A R A I I Toll Bar R E T A N L A V R O D ENT N M L R T A ESC D Almholme Field I E I G E A V R E D A EW E E O E C N V V T D IV E D I V I T G N S E E R R Prim Sch -

Frickley Mews Extra Care Opening the Door to Independent Living
FRICKLEY MEWS EXTRA CARE COLLIERS PLACE, OFF WESTFIELD LANE, SOUTH ELMSALL Opening the door to independent living A member of the Together Housing Group Extra Care living Frickley Mews is a new housing development of self-contained two-bedroom apartments available to rent. The development has been sensitively designed to allow people over the age of 50, who have an assessed need for care and support including those living with dementia, to remain independent in their own home for as long as possible. The apartments are available for single people or couples. Couples are able to stay together as long as one of them meets the eligibility criteria. Situated in Colliers Place, off Westfield Lane in South Elmsall, this state-of-the-art development consists of 67 apartments. Other facilities include a hairdresser and beauty salon, restaurant and coffee bar. Frickley Mews has been designed to be fully accessible and dementia friendly. The development will provide a 24-hour, seven days per week on-site team to meet care and support needs. The cost of the rent and service charge at Frickley Mews and the care and support package will be discussed in more detail on application. People may be entitled to help with these costs. Peace of mind with Extra Care Frickley Mews is an Extra Care development. Frickley Mews is a mixed community of people with a range of needs and abilities, This means tenants can continue to live including people living with impairments, independently in their own apartments with frailties, disabilities and dementia. It is a the reassurance that there is a care and place that provides a culture of respect support team on hand. -

Agenda Item 4
Agenda Item 4 SHEFFIELD CITY COUNCIL Individual Cabinet Member Decision Report of: Executive Director, Place __________________________________________________________________ Date: 9 June 2016 __________________________________________________________________ Subject: Sheffield 20mph Speed Limit Strategy: Responses to a proposal to introduce a 20mph speed limit in Greystones and Whirlow __________________________________________________________________ Author of Report: Simon Nelson __________________________________________________________________ Summary: This report describes the response from residents to the proposed introduction of a 20mph speed limit in Greystones and Whirlow, reports the receipt of objections and sets out the Council’s response. __________________________________________________________________ Reasons for Recommendations: Reducing the speed of traffic in residential areas will, in the long term, reduce the number and severity of accidents, reduce the fear of accidents, encourage sustainable modes of travel and contribute towards the creation of a more pleasant, cohesive environment. The introduction of a 20mph speed limit in this area would be in-keeping with the City’s approved 20mph Speed Limit Strategy. Having considered the objections to the principle of introducing a 20mph speed limit in Greystones and Whirlow the officer view is that the reasons set out in this report for making the Speed Limit Order outweigh the objections. Consideration has been given to objections to the inclusion of a number of specific roads within the Greystones and Whirlow 20mph speed limit area (see paragraph 4.13). Of these it is recommended that the objections to the inclusion of Bents Road and Knowle Lane be upheld. Recommendations: 7.1 Make the Greystones and Whirlow 20mph Speed Limit Order in accordance with the Road Traffic Regulation Act 1984, omitting Bents Road and Knowle Lane from that Order. -
Here to Them, We Risk Eventing Being Prohibited
Frickley Park FRICKLEY PARK HORSE TRIALS Horse Trials 24th - 26th July 2020 2019 BE100 Yorkshire Challenge Champion Hannah Atkinson on Icarus Frickley Park Horse Trials By kind permission @FrickleyParkHT of Charlie & Jayne Warde-Aldam @frickleyparkhorsetrials Welcome to Frickley Thank you so much for coming to Frickley Park in truly exceptional circumstances. These are not normal times and it was only 5 weeks ago that we were trying to gauge whether we would be able to run Frickley (1) or not. As it has transpired, we have enjoyed exceptional entries as people rush back to eventing and we are hopeful of making donations to our charities, the Yorkshire Air Ambulance and the Eye Department at Sheffield’s Children Hospital, once the final expenses have been paid off. The venue is looking different from previous fixtures; no marquee, no secretaries and no crowds enjoying this amazing parkland. However, despite these changes, we still offer what Frickley has become famous for; great grass arenas, proper XC courses and a friendly welcome. A huge thank you for making this happen must also go to our loyal sponsors, led by title sponsor Savills. Without their support, we would never have been able to put on this fixture. Whilst we have lost some costs as a result of the ‘new look’ eventing, the need to comply with the rules on dealing with Covid-19 have added many others. We really hope that this is for one year only and we can return with the full Frickley experience in 2021. Finally, please could everyone comply in full with the protocols issued by British Eventing. -

South Elmsall and South Kirkby Ward
InstantAtlas™ Server 6 Wakefield Ward Profile Selection: South Elmsall and South Kirkby Ward Introduction The Wakefield district is divided into 21 wards, with each ward being represented by three councillors. Councillors are elected by residents of the district and are responsible for making decisions about local services and budgets, such as Council Tax, on behalf of the local community. Each councillor serves for a period of four years. The ward boundaries are reviewed periodically, and the current boundaries were last altered in 2004. South Elmsall and South Kirkby Ward is situated in the far south east of the district. The ward contains the small towns of South Kirkby and South Elmsall. There are significant industrial estates at Langthwaite Grange, South Kirkby, and at Dale Lane, South Elmsall. The East Coast Mainline railway runs through the middle of the ward. Selected landmarks: South Elmsall Market Frickley Country Park Profile created: 9/1/2017 Population Profile Population Size The most accurate population estimates are produced every ten years from the Census. These are updated annually using administrative data to produce mid- year population estimates. The mid-2014 estimates show that the size of the resident population in South Elmsall and South Kirkby Ward is 17,757 people. The tables below shows the percentage breakdown by age groups and gender. The actual number of people in each age group is shown in brackets. Population Size South Elmsall and South Kirkby Ward Total population (2014) 17,757 people Total male population -
UK Coal Resource for New Exploitation Technologies Final Report
UK Coal Resource for New Exploitation Technologies Final Report Sustainable Energy & Geophysical Surveys Programme Commissioned Report CR/04/015N BRITISH GEOLOGICAL SURVEY Commissioned Report CR/04/015N UK Coal Resource for New Exploitation Technologies Final Report *Jones N S, *Holloway S, +Creedy D P, +Garner K, *Smith N J P, *Browne, M.A.E. & #Durucan S. 2004. *British Geological Survey +Wardell Armstrong # Imperial College, London The National Grid and other Ordnance Survey data are used with the permission of the Controller of Her Majesty’s Stationery Office. Ordnance Survey licence number GD 272191/1999 Key words Coal resources, UK, maps, undergound mining, opencast mining, coal mine methane, abandoned mine methane, coalbed methane, underground coal gasification, carbon dioxide sequestration. Front cover Cleat in coal Bibliographical reference Jones N S, Holloway S, Creedy D P, Garner K, Smith N J P, Browne, M.A.E. & Durucan S. 2004. UK Coal Resource for New Exploitation Technologies. Final Report. British Geological Survey Commissioned Report CR/04/015N. © NERC 2004 Keyworth, Nottingham British Geological Survey 2004 BRITISH GEOLOGICAL SURVEY The full range of Survey publications is available from the BGS Keyworth, Nottingham NG12 5GG Sales Desks at Nottingham and Edinburgh; see contact details 0115-936 3241 Fax 0115-936 3488 below or shop online at www.thebgs.co.uk e-mail: [email protected] The London Information Office maintains a reference collection www.bgs.ac.uk of BGS publications including maps for consultation. Shop online at: www.thebgs.co.uk The Survey publishes an annual catalogue of its maps and other publications; this catalogue is available from any of the BGS Sales Murchison House, West Mains Road, Edinburgh EH9 3LA Desks. -

West Yorkshire Geology Trust Newsletter
West Yorkshire Geology Trust Newsletter Editorial It has been a busy summer and the enthusiasts on the committee have been getting out to look at West Yorkshire's significant geological sites, as you can see from some of the reports. They would like you to take part in this activity, by visiting a nearby Local Geological Site and filling in a monitoring form for us. Please get in touch using the email address [email protected]. We also try to ensure that we are notified about any planning applications which might threaten any of our sites, so that we can suggest work with various authorities to find ways in which they can be protected, so let us know if you become aware of any misuse of geological sites. Thanks to Gareth Martin for producing a full and interesting newsletter and we hope that we will be able to publicise guided walks around some of our best sites during next spring and summer. Frickley Country Park visit On 13th February Tony Felski of WYGT led a very well attended guided walk to Frickley Country Park in South Elmsall. While there are no geological exposures this magnificent country park, the site of the old Frickley Colliery, has been developed to incorporate geological features into the landscape as well as indications of its past coal mining heritage. One such example are the large mounds on the hill at eastern end representing the stromatolites which formed in the tropical seas which covered West Yorkshire during the late Permian when the Cadeby Formation limestone was deposited (right hand photo below). -

Residential Development Opportunity Doncaster
Residential Development Opportunity Doncaster Broadlands Farm, Church Field Road, Clayton, Doncaster, DN5 7DP For Sale . The site extends to approximately 0.76 acres (0.309 hectares) . Stone built farmhouse, traditional barns and outbuildings . Full Planning Permission for a scheme of three dwellings . Located in a rural position between Doncaster, Wakefield and Barnsley . Benefits from excellent proximity to Junctions 37 & 38 A1 (M) . Offers are invited to be provided on an unconditional basis . Viewings strictly by appointment only savills.co.uk Location The site is situated in a rural location in the picturesque south Yorkshire village of Clayton, approximately 9 miles north west of Doncaster town centre. The development site is well placed for access to the national motorway network. Junctions 37 and 38 of the A1 (M) are situated within approximately 6 miles north and south respectively, providing excellent motorway links regionally and nationally. Doncaster is situated on the East Coast mainline, providing a regular rail service to London in under 1 hour 45 minutes. All Saints C of E Primary School in the neighbouring village of Hooton Pagnell has an Ofsted rating of ‘Outstanding’. The town of South Elmsall is approximately 4 miles to the north and is well serviced with a range of amenities, including an Asda superstore and Jet petrol station as well as South Elmsall/Moorthorpe Railway Station. Surrounding the site lies open agricultural land to the north, which is in the present Vendor’s ownership. There are a collection of period residential properties to the north and north west of the boundary. Church Field Road runs along the southern site boundary.