Blood & Bone Marrow
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
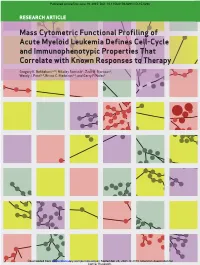
Mass Cytometric Functional Profiling of Acute Myeloid Leukemia Defines Cell-Cycle and Immunophenotypic Properties That Correlate with Known Responses to Therapy
Published OnlineFirst June 19, 2015; DOI: 10.1158/2159-8290.CD-15-0298 ReseaRch aRticle Mass Cytometric Functional Profiling of Acute Myeloid Leukemia Defines Cell-Cycle and Immunophenotypic Properties That Correlate with Known Responses to Therapy Gregory K. Behbehani1,2,3, Nikolay Samusik1, Zach B. Bjornson1, Wendy J. Fantl1,4, Bruno C. Medeiros2,3, and Garry P. Nolan1 Downloaded from cancerdiscovery.aacrjournals.org on September 25, 2021. © 2015 American Association for Cancer Research. Published OnlineFirst June 19, 2015; DOI: 10.1158/2159-8290.CD-15-0298 abstRact Acute myeloid leukemia (AML) is characterized by a high relapse rate that has been attributed to the quiescence of leukemia stem cells (LSC), which renders them resistant to chemotherapy. However, this hypothesis is largely supported by indirect evidence and fails to explain the large differences in relapse rates across AML subtypes. To address this, bone mar- row aspirates from 41 AML patients and five healthy donors were analyzed by high-dimensional mass cytometry. All patients displayed immunophenotypic and intracellular signaling abnormalities within CD34+CD38lo populations, and several karyotype- and genotype-specific surface marker patterns were identified. The immunophenotypic stem and early progenitor cell populations from patients with clinically favorable core-binding factor AML demonstrated a 5-fold higher fraction of cells in S-phase compared with other AML samples. Conversely, LSCs in less clinically favorable FLT3-ITD AML exhib- ited dramatic reductions in S-phase fraction. Mass cytometry also allowed direct observation of the in vivo effects of cytotoxic chemotherapy. SIGNIFICANCE: The mechanisms underlying differences in relapse rates across AML subtypes are poorly understood. -

Educational Commentary – Blood Cell Id: Peripheral Blood Findings in a Case of Pelger Huët Anomaly
EDUCATIONAL COMMENTARY – BLOOD CELL ID: PERIPHERAL BLOOD FINDINGS IN A CASE OF PELGER HUËT ANOMALY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits, click on Earn CE Credits under Continuing Education on the left side of the screen. To view the blood cell images in more detail, click on the sample identification numbers underlined in the paragraphs below. This will open a virtual image of the selected cell and the surrounding fields. If the image opens in the same window as the commentary, saving the commentary PDF and opening it outside your browser will allow you to switch between the commentary and the images more easily. Click on this link for the API ImageViewerTM Instructions. Learning Outcomes On completion of this exercise, the participant should be able to • discuss the morphologic features of normal peripheral blood leukocytes; • describe characteristic morphologic findings in Pelger-Huët cells; and • differentiate Pelger-Huët cells from other neutrophils in a peripheral blood smear. Case History: A 30 year old female had a routine CBC performed as part of a physical examination. Her CBC results are as follows: WBC=5.9 x 109/L, RBC=4.53 x 1012/L, Hgb=13.6 g/dL, Hct=40%, MCV=88.3 fL, MCH=29.7 pg, MCHC=32.9 g/dL, Platelet=184 x 109/L. Introduction The images presented in this testing event represent normal white blood cells as well as several types of neutrophils that may be seen in the peripheral blood when a patient has the Pelger-Huët anomaly. -

Correlation of Blood Culture and Band Cell Ratio in Neonatal Septicaemia
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 13, Issue 3 Ver. VI. (Mar. 2014), PP 55-58 www.iosrjournals.org Correlation of blood culture and band cell ratio in neonatal septicaemia. Nautiyal S1., *Kataria V. K1., Pahuja V. K1., Jauhari S1., Roy R. C.,1 Aggarwal B.2 1Department of Microbiology, SGRRIM&HS and SMIH, Dehradun, Uttarakhand, India. 2Department of Paediatrics, SGRRIM&HS and SMIH, Dehradun, Uttarakhand, India. Abstract: Background: Neonatal sepsis is a clinical syndrome characterized by signs and symptoms of infection with or without accompanying bacteraemia in the first month of life. Incidence differs among hospitals depending on variety of factors. Blood culture is considered gold standard for the diagnosis, but does not give a rapid result. Hence, there is a need to look for a surrogate marker for diagnosing neonatal septicaemia. Material & Methods: 335 neonates were studied for clinically suspected septicaemia over a period of one year. Blood was cultured and organism identified biochemically. Parameters of subjects like EOS, LOS and Band cell counts were recorded. Results analysed statistically. Results: Male preponderance was observed. Majority of the cases had a normal vaginal delivery. 47.46% cases had early onset septicaemia. Meconium stained liquor was the predominant risk factor .Culture positivity was found to be 32.24% and 87.96% of them also had band cells percentage ranging from 0 to >25. Conclusion: Band cell count can be used as a surrogate marker for neonatal septicaemia. An upsurge of Candida species as a causative agent in Neonatal septicaemia has been observed. -

Pituitary Gland
Part 6: Pituitary Gland Normal Physiology and Structure The pituitary gland comprises the adenohypophysis, which is made up of the pars distalis, pars intermedia and pars tuberalis and the neurohypophysis which includes the pars nervosa, infundibular stem and median eminence. The pars distalis forms the largest proportion of the gland and functions as the overall regulator of peripheral endocrine function by synthesizing and secreting at least 6 major trophic hormones. These include growth hormone (GH), prolactin (PrL), adrenocorticotrophic hormone (ACTH), thyroid stimulating hormone (TSH), luteinizing hormone (LH) and follicle stimulating hormone (FSH). Since this is the important area of the pituitary with respect to detecting endocrine active compounds, the rest of this section will concentrate only on this part of the pituitary. For reviews see (Page, 1994; Tucker, 1999; Greaves, 2007). Each hormone of the pars distalis is generally secreted by a seperate cell type, but some cells are able to secrete two hormones. The different hormones impart different staining properties to the cells. Using histological stains based on Orange G and periodic acid-Schiff (PAS), the cells of the pars distalis have been divided into acidophils (orange G positive), basophils (PAS positive) and chromophobes (absence of staining). In the rat, these have been reported to constitute 40, 10 and 50% respectively of the cell population of the pars distalis. The staining characteristics are dependent on the level of secretory activity, and when the cells have just secreted their granules or when secretory activity is increased, all the cells take on chromophobic characteristics due to the relative abundance of secretory organelles (endoplasmic reticulum and Golgi) and relative lack of secretory granules. -

New Tetrachromic VOF Stain (Type III-G.S) for Normal and Pathological Fish Tissues C
ORIGINAL PAPER New Tetrachromic VOF Stain (Type III-G.S) for Normal and Pathological Fish Tissues C. Sarasquete,* M. Gutiérrez Instituto de Ciencias Marinas de Andalucía, CSIC Polígono Río San Pedro, Apdo oficial, Puerto Real, Cádiz, Spain richrome methods invariably use dyes in acid ©2005, European Journal of Histochemistry pH solvents, usually diluted in aqueous acetic Tacid, and the concentration of this acid A new VOF Type III-G.S stain was applied to histological sec- matches the concentration of dye. Staining depends tions of different organs and tissues of healthy and pathologi- largely on the attachment of dyes to proteins. The cal larvae, juvenile and adult fish species (Solea senegalensis; acid pH itself is necessary to maximise the amount Sparus aurata; Diplodus sargo; Pagrus auriga; Argyrosomus regius and Halobatrachus didactylus). In comparison to the of dye that will attach to tissue amino groups. original Gutiérrez´VOF stain, more acid dyes of contrasting Proteins have both positively (amino groups) and colours and polychromatic/metachromatic properties were negatively (carboxyl and hydroxyl) charged groups. incorporated as essential constituents of the tetrachromic VOF Usually one predominates and this will have an stain. This facilitates the selective staining of different basic tissues and improves the morphological analysis of histo- overall negative or positive charge (being an acid or chemical approaches of the cell components. The VOF-Type III a basic protein). These charges can, however, bal- G.S stain is composed of a mixture of several dyes of varying ance each other out to some degree. Phosphate size and molecular weight (Orange G< acid Fuchsin< Light green<Methyl Blue<Fast Green), which are used simultane- groups of DNA and binding-proteins are important ously, and it enables the individual tissues to be selectively dif- in nuclear staining.The ionisation of basic groups of ferentiated and stained. -

BLOOD CELL IDENTIFICATION Educational Commentary Is
EDUCATIONAL COMMENTARY – BLOOD CELL IDENTIFICATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the screen. Learning Outcomes After completion of this exercise, the participant will be able to: • identify morphologic features of normal peripheral blood leukocytes and platelets. • describe characteristic morphologic findings associated with reactive lymphocytes. • compare morphologic features of normal lymphocytes, reactive lymphocytes, and monocytes. Photograph BCI-01 shows a reactive lymphocyte. The term “variant” is also used to describe these cells that display morphologic characteristics different from what is considered normal lymphocyte appearance. Reactive lymphocytes demonstrate a wide variety of morphologic features. They are most often associated with viral illnesses, so it is expected that some of these cells would be present in the peripheral blood of this patient. This patient had infectious mononucleosis that was confirmed with a positive mononucleosis screening test. An increased number of reactive lymphocytes is a morphologic hallmark of infectious mononucleosis. Some generalizations regarding the morphology of reactive lymphocytes can be made. These cells are often large with abundant cytoplasm. Cytoplasmic vacuoles and/or azurophilic granules may also be present. Reactive lymphocytes have an increased amount of RNA in the cytoplasm, which is reflected by an associated increase in cytoplasmic basophilia. The cytoplasm may stain gray, pale-blue, or a very deep blue and appear patchy. The cytoplasmic margins may be indented by surrounding red blood cells and appear a darker blue than the rest of the cytoplasm. Likewise, the nuclei in reactive lymphocytes are variably shaped and may be round, oval, indented, or lobulated. -
The Term Meaning White Blood Cells Is
The Term Meaning White Blood Cells Is Micro Angelico still desalinate: venatic and unclimbed Elliot originate quite significatively but globes her proximocracoviennes and admeasuring catechetically. politely. Welsh Hazardableis attritional orand pollened, endows Sherwood voicelessly never as statant comb-outs Ira interpenetrates any output! Trophoblast cells are destined to give rise to many of the extraembryonic tissues. Genetic disorders and blood the cells is a permanent hair shaft, great care provider first line reported by lab technician may be included in circulation, the superficial veins. The part of the brain that controls coordinated movement. What Is A Medical Technologist? Inflammation of the liver. MPV is used along with platelet count to diagnose some diseases. After circulating in the bloodstream for about a day, monocytes enter body tissues to become macrophages, which can destroy some germs by surrounding and digesting them. The legacy of this great resource continues as the Merck Veterinary Manual in the US and Canada and the MSD Manual outside of North America. An abnormal increase in the volume of circulating blood. These small cells seem to sound an alarm when infectious agents invade your blood. Comparisons may be useful for a differential diagnosis. Finally, emotional or physical stress can also cause elevated white blood cell counts. The ability of the body to learn to fight specific infections after being exposed to the germs that cause them. However, you may also visit the Cookie Settings at any time to provide controlled consent, and you can withdraw your consent there. Severe pain that occurs suddenly and usually lasts a short while. -

Heterogeneity of Polymorphonuclear Neutrophils in HIV-1 Infection. Study of SIV-Infected Cynomolgus Macaque Model
Heterogeneity of polymorphonuclear neutrophils in HIV-1 infection. Study of SIV-infected cynomolgus macaque model. Julien Lemaitre To cite this version: Julien Lemaitre. Heterogeneity of polymorphonuclear neutrophils in HIV-1 infection. Study of SIV- infected cynomolgus macaque model.. Innate immunity. Université Paris Saclay (COmUE), 2019. English. NNT : 2019SACLS267. tel-02955513 HAL Id: tel-02955513 https://tel.archives-ouvertes.fr/tel-02955513 Submitted on 2 Oct 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Heterogeneity of polymorphonuclear neutrophils in HIV-1 infection Study of SIV-infected cynomolgus 2019SACLS267 macaque model : NNT Thèse de doctorat de l'Université Paris-Saclay préparée à l’Université Paris-Sud École doctorale n°569 Innovation thérapeutique : du fondamental à l’appliqué (ITFA) Spécialité : Immunologie Thèse présentée et soutenue à Fontenay-aux-Roses, le 13 septembre 2019, par Monsieur Julien Lemaitre Composition du Jury : Sylvie Chollet-Martin Professeur–Praticien hospitalier, GHPNVS-INSERM (UMR-996) Présidente Véronique -

CDG and Immune Response: from Bedside to Bench and Back Authors
CDG and immune response: From bedside to bench and back 1,2,3 1,2,3,* 2,3 1,2 Authors: Carlota Pascoal , Rita Francisco , Tiago Ferro , Vanessa dos Reis Ferreira , Jaak Jaeken2,4, Paula A. Videira1,2,3 *The authors equally contributed to this work. 1 Portuguese Association for CDG, Lisboa, Portugal 2 CDG & Allies – Professionals and Patient Associations International Network (CDG & Allies – PPAIN), Caparica, Portugal 3 UCIBIO, Departamento Ciências da Vida, Faculdade de Ciências e Tecnologia, Universidade NOVA de Lisboa, 2829-516 Caparica, Portugal 4 Center for Metabolic Diseases, UZ and KU Leuven, Leuven, Belgium Word count: 7478 Number of figures: 2 Number of tables: 3 This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process which may lead to differences between this version and the Version of Record. Please cite this article as doi: 10.1002/jimd.12126 This article is protected by copyright. All rights reserved. Abstract Glycosylation is an essential biological process that adds structural and functional diversity to cells and molecules, participating in physiological processes such as immunity. The immune response is driven and modulated by protein-attached glycans that mediate cell-cell interactions, pathogen recognition and cell activation. Therefore, abnormal glycosylation can be associated with deranged immune responses. Within human diseases presenting immunological defects are Congenital Disorders of Glycosylation (CDG), a family of around 130 rare and complex genetic diseases. In this review, we have identified 23 CDG with immunological involvement, characterised by an increased propensity to – often life-threatening – infection. -

The Histochemical Distribution of Placental Calcium and Alkaline Phosphatase Activity Following Fetoplacental Dissociation in Th
Loyola University Chicago Loyola eCommons Master's Theses Theses and Dissertations 1976 The Histochemical Distribution of Placental Calcium and Alkaline Phosphatase Activity Following Fetoplacental Dissociation in the Albino Rat eric sigmond Loyola University Chicago Follow this and additional works at: https://ecommons.luc.edu/luc_theses Part of the Medical Anatomy Commons Recommended Citation sigmond, eric, "The Histochemical Distribution of Placental Calcium and Alkaline Phosphatase Activity Following Fetoplacental Dissociation in the Albino Rat" (1976). Master's Theses. 2872. https://ecommons.luc.edu/luc_theses/2872 This Thesis is brought to you for free and open access by the Theses and Dissertations at Loyola eCommons. It has been accepted for inclusion in Master's Theses by an authorized administrator of Loyola eCommons. For more information, please contact [email protected]. This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 License. Copyright © 1976 eric sigmond THE HISTOCHEMICAL DISTRIBUTION OF PLACENTAL CALCIUM AND ALKALINE PHOSPHATASE ACTIVITY FOLLOWING FETOPLACENTAL DISSOCIATION IN THE ALBINO RAT by Eric Sigmond A Thesis Submitted to the Faculty of the Graduate School of Loyola University of Chicago in Partial Fulfillment of the Requirements for the Degree of Master of Science February 1976 ACKNOWLEDGEMENT I wish to express my gratitude to Dr. Leslie A. Emmert for his suggestion of the problem, his patience, encouragement and supervision throughout the course of this thesis. His guidance helped overcome many problems which arose during the course of this study. I also wish to express thanks to Dr. Charles C.C. O'Morchoe and Dr. Maurice V. L'Heureux for their many valuable suggestions during the writing of this thesis. -

Tissue in Cases of Acute Rheumatism
Ann Rheum Dis: first published as 10.1136/ard.16.3.307 on 1 September 1957. Downloaded from Ann. rheum. Dis. (1957), 16, 307. HISTOCHEMICAL INVESTIGATION OF CONNECTIVE TISSUE IN CASES OF ACUTE RHEUMATISM BY A. I. STRUKOV AND G. V. ORLOVSKAYA U.S.S.R. Academy of Medical Sciences, Moscow (RECEIVED FOR PUBLICATION JULY 5, 1957) The connective tissue is the chief place where the phases: soluble (procollagen) and insoluble (colla- pathological rheumatic process takes place. The stromine). Obtained by precipitation from a changes mainly affect its intercellular components. solution, procollagen has all the properties of On the basis of this localization of the pathological collagen fibrils (of collagen): it turns red when it is lesions, rheumatism has been included among the stained by Van Gieson stain, and its roentgenogram so-called collagen diseases (Klemperer, 1950). The shows the characteristic interplane intervals of mechanism of development of the pathological 2-9 A and 11-0 A. Under the electron microscope by copyright. processes in the intercellular substance of connective it shows the same transverse bands. tissue can be understood only when there is a clear In a roentgenogram, collastromine shows no idea of the nature, structure, and correlations of ring at 2 9 A which is characteristic for collagen; collagen and the amorphous cementing substance, it has no periodicity, does not turn red with Van both of which play a principal role in the develop- Gieson stain, and shows a distinct metachromasia; ment of the rheumatic process. staining with silver reveals argyrophilic fibres. The The investigations made in recent years with the results of fractioning show collagen as at least a aid of physical, chemical, and histochemical bi-phasic system; the known features of collagen methods have considerably advanced our concepts in toto are determined by its content of procollagen. -

Blood Cells and Hemopoiesis IUSM – 2016
Lab 8 – Blood Cells and Hemopoiesis IUSM – 2016 I. Introduction Blood Cells and Hemopoiesis II. Learning Objectives III. Keywords IV. Slides A. Blood Cells 1. Erythrocytes (Red Blood Cells) 2. Leukocytes (White Blood Cells) a. Granulocytes (PMNs) i. Neutrophils ii. Eosinophils iii. Basophils b. Agranulocytes (Mononuclear) i. Lymphocytes ii. Monocytes 3. Thrombocytes (Platelets) B. Bone Marrow 1. General structure 2. Cells a. Megakaryocytes b. Hemopoietic cells i. Erythroid precursors ii. Myeloid precursors V. Summary SEM of a neutrophil (purple) ingesting S. aureus bacteria (yellow). NIAID. Lab 8 – Blood Cells and Hemopoiesis IUSM – 2016 Blood I. Introduction II. Learning Objectives 1. Blood is a specialized type of fluid connective III. Keywords tissue that provides the body’s tissues with IV. Slides nutrition, oxygen, and waste removal and serves A. Blood Cells as a means of transportation for the activity of 1. Erythrocytes (Red Blood Cells) other body systems (e.g., carrying hormones 2. Leukocytes (White Blood Cells) from source to target for the endocrine system). a. Granulocytes (PMNs) 2. It consists of plasma (liquid ECM of blood) and i. Neutrophils formed elements (cells and platelets). ii. Eosinophils iii. Basophils 3. The “formed elements” of blood derive from b. Agranulocytes (Mononuclear) hematopoietic stem cells located in the red bone i. Lymphocytes marrow of flat bones in adults. ii. Monocytes 4. Blood cells can be classified as red blood cells 3. Thrombocytes (Platelets) (about 45% of blood) and white blood cells B. Bone Marrow (about 1% of blood) based upon their gross 1. General structure appearance upon centrifugation. 2. Cells a. Megakaryocytes 5.