Social Determinants of Inuit Health in Canada
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Safeguarding the Arctic Why the U.S
Safeguarding the Arctic Why the U.S. Must Lead in the High North By Cathleen Kelly and Miranda Peterson January 22, 2015 “As the United States assumes the Chairmanship of the Arctic Council, it is more important than ever that we have a coordinated national effort that takes advantage of our combined expertise and efforts in the Arctic region to promote our shared values and priorities.” — President Obama, Executive Order on Enhancing Coordination of National Efforts in the Arctic, January 21, 20151 While many Americans do not consider the United States to be an Arctic nation, Alaska—which constitutes 16 percent of the country’s landmass and sits on the Arctic Circle—puts the country solidly in that category.2 Consequently, it is with good reason that the United States has a seat on the Arctic Council. As Arctic warming accelerates, U.S. leadership in the High North is key not only to the public health and safety of Americans and other people in the region, but also to U.S. national security and the fate of the planet. In just three months, U.S. Secretary of State John Kerry will become chairman of the Arctic Council. The two-year position rotates among the eight Arctic nations3—Canada, Finland, Iceland, Norway, Russia, Sweden, the United States, and Denmark, including Greenland and the Faroe Islands—and is a powerful platform for shaping how the risks and opportunities of increasing commercial activity at the top of the world are managed. To ready the administration for Secretary Kerry’s turn to hold the Arctic Council gavel from 2015 to 2017, President Barack Obama recently issued an executive order to better coordinate national efforts in the Arctic.4 The executive order is the latest signal from the White House that President Obama and Secretary Kerry are focused on preparing the nation for dramatic changes in the Arctic and protecting U.S. -

The Need for Fast Near-Term Climate Mitigation to Slow Feedbacks and Tipping Points
The Need for Fast Near-Term Climate Mitigation to Slow Feedbacks and Tipping Points Critical Role of Short-lived Super Climate Pollutants in the Climate Emergency Background Note DRAFT: 27 September 2021 Institute for Governance Center for Human Rights and & Sustainable Development (IGSD) Environment (CHRE/CEDHA) Lead authors Durwood Zaelke, Romina Picolotti, Kristin Campbell, & Gabrielle Dreyfus Contributing authors Trina Thorbjornsen, Laura Bloomer, Blake Hite, Kiran Ghosh, & Daniel Taillant Acknowledgements We thank readers for comments that have allowed us to continue to update and improve this note. About the Institute for Governance & About the Center for Human Rights and Sustainable Development (IGSD) Environment (CHRE/CEDHA) IGSD’s mission is to promote just and Originally founded in 1999 in Argentina, the sustainable societies and to protect the Center for Human Rights and Environment environment by advancing the understanding, (CHRE or CEDHA by its Spanish acronym) development, and implementation of effective aims to build a more harmonious relationship and accountable systems of governance for between the environment and people. Its work sustainable development. centers on promoting greater access to justice and to guarantee human rights for victims of As part of its work, IGSD is pursuing “fast- environmental degradation, or due to the non- action” climate mitigation strategies that will sustainable management of natural resources, result in significant reductions of climate and to prevent future violations. To this end, emissions to limit temperature increase and other CHRE fosters the creation of public policy that climate impacts in the near-term. The focus is on promotes inclusive socially and environmentally strategies to reduce non-CO2 climate pollutants, sustainable development, through community protect sinks, and enhance urban albedo with participation, public interest litigation, smart surfaces, as a complement to cuts in CO2. -
Arctic Report Card 2018 Effects of Persistent Arctic Warming Continue to Mount
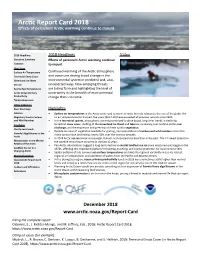
Arctic Report Card 2018 Effects of persistent Arctic warming continue to mount 2018 Headlines 2018 Headlines Video Executive Summary Effects of persistent Arctic warming continue Contacts to mount Vital Signs Surface Air Temperature Continued warming of the Arctic atmosphere Terrestrial Snow Cover and ocean are driving broad change in the Greenland Ice Sheet environmental system in predicted and, also, Sea Ice unexpected ways. New emerging threats Sea Surface Temperature are taking form and highlighting the level of Arctic Ocean Primary uncertainty in the breadth of environmental Productivity change that is to come. Tundra Greenness Other Indicators River Discharge Highlights Lake Ice • Surface air temperatures in the Arctic continued to warm at twice the rate relative to the rest of the globe. Arc- Migratory Tundra Caribou tic air temperatures for the past five years (2014-18) have exceeded all previous records since 1900. and Wild Reindeer • In the terrestrial system, atmospheric warming continued to drive broad, long-term trends in declining Frostbites terrestrial snow cover, melting of theGreenland Ice Sheet and lake ice, increasing summertime Arcticriver discharge, and the expansion and greening of Arctic tundravegetation . Clarity and Clouds • Despite increase of vegetation available for grazing, herd populations of caribou and wild reindeer across the Harmful Algal Blooms in the Arctic tundra have declined by nearly 50% over the last two decades. Arctic • In 2018 Arcticsea ice remained younger, thinner, and covered less area than in the past. The 12 lowest extents in Microplastics in the Marine the satellite record have occurred in the last 12 years. Realms of the Arctic • Pan-Arctic observations suggest a long-term decline in coastal landfast sea ice since measurements began in the Landfast Sea Ice in a 1970s, affecting this important platform for hunting, traveling, and coastal protection for local communities. -

GREENLAND Summer and Winter Adventures
GREENLAND summer and winter adventures Greenland summer and winter adventures 1 Greenland with Albatros Travel With a strong foothold in Kangerlussuaq, we can provide your clients with a seamless experience of Greenland. Three Table of decades ago, we were one of the first travel operators to venture into the arctic wilderness of Greenland. Today, we CONTENTS have cemented our presence there in the form of a local office, restaurant, gift shop and two hostels. 2 INTRODUCTION 4-5 YOUR GATEWAY TO GREEENLAND Find out more about our Greenland operations on page 4. 8-9 SHIP: OCEAN DIAMOND Why Albatros 6-7 SUMMER TOURS Greenland holds a special place in our hearts here at Albatros Travel. With headquarters 8-9 GREENLAND’S MAGICAL MIDNIGHT SUN in Copenhagen, Denmark, our connection to this vast continent is like that of all Danes. 10-11 MAGNIFICENT GREENLAND The joint history has been murky and at times dark. However, we are determined to show - ICE SHEET AND ICEBERGS guests from abroad how incredibly beautiful and untouched Greenland is. 12-13 SUMMER IN ICELAND AND ILULISSAT We cherish the wide, open spaces, the long, dark winters only brightened by the sparkling 14-15 TREASURES OF SOUTH GREENLAND snow, breathtaking northern lights (the aurora borealis), the short, and surprisingly green summers lit by the midnight sun, the seemingly endless icescapes and the warmth of the 16-17 WINTER TOURS Greenlandic people. Yes, the list is long and we could go on. 18-19 WINTER WONDERLAND IN GREENLAND We don’t just know Greenland’s history, the names of its birds, wildlife and its nature. -
Changes in Snow, Ice and Permafrost Across Canada
CHAPTER 5 Changes in Snow, Ice, and Permafrost Across Canada CANADA’S CHANGING CLIMATE REPORT CANADA’S CHANGING CLIMATE REPORT 195 Authors Chris Derksen, Environment and Climate Change Canada David Burgess, Natural Resources Canada Claude Duguay, University of Waterloo Stephen Howell, Environment and Climate Change Canada Lawrence Mudryk, Environment and Climate Change Canada Sharon Smith, Natural Resources Canada Chad Thackeray, University of California at Los Angeles Megan Kirchmeier-Young, Environment and Climate Change Canada Acknowledgements Recommended citation: Derksen, C., Burgess, D., Duguay, C., Howell, S., Mudryk, L., Smith, S., Thackeray, C. and Kirchmeier-Young, M. (2019): Changes in snow, ice, and permafrost across Canada; Chapter 5 in Can- ada’s Changing Climate Report, (ed.) E. Bush and D.S. Lemmen; Govern- ment of Canada, Ottawa, Ontario, p.194–260. CANADA’S CHANGING CLIMATE REPORT 196 Chapter Table Of Contents DEFINITIONS CHAPTER KEY MESSAGES (BY SECTION) SUMMARY 5.1: Introduction 5.2: Snow cover 5.2.1: Observed changes in snow cover 5.2.2: Projected changes in snow cover 5.3: Sea ice 5.3.1: Observed changes in sea ice Box 5.1: The influence of human-induced climate change on extreme low Arctic sea ice extent in 2012 5.3.2: Projected changes in sea ice FAQ 5.1: Where will the last sea ice area be in the Arctic? 5.4: Glaciers and ice caps 5.4.1: Observed changes in glaciers and ice caps 5.4.2: Projected changes in glaciers and ice caps 5.5: Lake and river ice 5.5.1: Observed changes in lake and river ice 5.5.2: Projected changes in lake and river ice 5.6: Permafrost 5.6.1: Observed changes in permafrost 5.6.2: Projected changes in permafrost 5.7: Discussion This chapter presents evidence that snow, ice, and permafrost are changing across Canada because of increasing temperatures and changes in precipitation. -

Heterogeneous CO2 and CH4 Content of Glacial Meltwater from the Greenland Ice Sheet and Implications for Subglacial Carbon Processes
The Cryosphere, 15, 1627–1644, 2021 https://doi.org/10.5194/tc-15-1627-2021 © Author(s) 2021. This work is distributed under the Creative Commons Attribution 4.0 License. Heterogeneous CO2 and CH4 content of glacial meltwater from the Greenland Ice Sheet and implications for subglacial carbon processes Andrea J. Pain1,a, Jonathan B. Martin1, Ellen E. Martin1, Åsa K. Rennermalm2, and Shaily Rahman1,b 1Department of Geological Sciences, University of Florida, Gainesville, FL 32611, USA 2Department of Geography, Rutgers, The State University of New Jersey, Piscataway NJ 08854, USA anow at: University of Maryland Center for Environmental Science, Horn Point Lab, Cambridge, MD 21613, USA bnow at: Department of Marine Science, University of Southern Mississippi, Stennis Space Center, MS 39529, USA Correspondence: Andrea J. Pain ([email protected]) Received: 18 June 2020 – Discussion started: 3 July 2020 Revised: 22 February 2021 – Accepted: 24 February 2021 – Published: 1 April 2021 Abstract. Accelerated melting of the Greenland Ice Sheet Sheet. Future work should constrain the extent and controls has increased freshwater delivery to the Arctic Ocean and of heterogeneity to improve our understanding of the impact amplified the need to understand the impact of Greenland of Greenland Ice Sheet melt on Arctic greenhouse gas bud- Ice Sheet meltwater on Arctic greenhouse gas budgets. We gets, as well as the role of continental ice sheets in green- evaluate subglacial discharge from the Greenland Ice Sheet house gas variations over glacial–interglacial timescales. for carbon dioxide (CO2) and methane (CH4) concentrations and δ13C values and use geochemical models to evaluate sub- glacial CH4 and CO2 sources and sinks. -
Lands' End to the Arctic
BOOKS & ARTS COMMENT Greenland’s ice cap, pictured here in a photo by US clothing retailer and research patron Gary Comer, serves as a vast climate-change archive. CLIMATE CHANGE Lands’ End to the Arctic Henry Pollack relishes a climate-science narrative with an intrepid and passionate businessman at its heart. wo narratives make up the fabric of to retrace the path of the east coast of North America, to enter the The Fate of Greenland. The polar- Vitus Bering in his Northwest Passage at its eastern portal in research perspectives of well-known 1728 voyage through Baffin Bay. Sixteen days later, Turmoil G. COMER Tclimate scientists form the main thread, the Bering Strait into emerged into the Beaufort Sea, north of woven through with a posthumous tribute to the Arctic Ocean. Alaska, the first private vessel in modern Gary Comer. Comer, founder of US clothing Comer invited natu- times to traverse the Northwest Passage unas- manufacturer Lands’ End, became a patron ralist Philip Conkling sisted by an icebreaker. Roughly a century of climate science in his later years, in a most and me to join him earlier, it had taken Roald Amundsen three unusual way. on that voyage, which years to make that voyage. A native of Chicago, Illinois, Comer had began, as did Bering’s, In an interview in the Chicago Tribune The Fate of as a young man crewed on sailing vessels in Kamchatka, the Greenland: Magazine shortly after this historic 2001 trav- large and small, developing a passion for massive volcanic pen- Lessons from erse, Comer said: “All along the way we were remote places. -

Land Cover Change – Ice Sheet Melt Case Study GREENLAND Chasing Ice
Unit 3: CHANGING THE LAND Land cover change – Ice Sheet Melt Case Study GREENLAND Chasing Ice https://youtube/hC3VTgIPoGU https://youtube/hC3VTgIPoGU LOCATION Greenland SIZE Location of major ice sheets Comparison of Antarctica’s & Greenland’s ice sheet features Comparison of Antarctica’s & Greenland’s ice sheet features Elevation with ice and snow Greenland FEATURES OF THE ICE SHEET • Greenland's Ice Cap actually consists of two domes of ice with a dip between them running across Greenland. • At its highest point, the Ice Cap is 3,200 metres above sea level, and its average thickness is approx. 2,135 metres – in fact, 65% of the ice surface is located more than 2,000 metres above sea level. • About a third of the ice lies below sea level, and this means that, if the ice melted, Greenland would actually be a ring-shaped country with a large lake in the middle. Ice sheet loss – the natural process Ice sheets flow outward from their dome-like centers, where they are generally thickest, and push ice outward until they encounter ocean. The ice sheet ice flow terminates at the ocean, as an ice tongue or ice shelf (fully floating thick permanent ice above the ocean). Stresses from ice flowing over bedrock causes fracturing, and at the front edge of the ice this fracturing leads to crevasses and eventually iceberg calving. The role of cryoconite The melting of ice in Greenland has been exacerbated by the discovery of increasing levels of cryoconite. This mineral begins as airborne sediment spread over ice by wind. -

Arctic Climate Feedbacks: Global Implications
for a living planet ARCTIC CLIMATE FEEDBACKS: GLOBAL IMPLICATIONS ARCTIC CLIMATE FEEDBACKS: GLOBAL IMPLICATIONS Martin Sommerkorn & Susan Joy Hassol, editors With contributions from: Mark C. Serreze & Julienne Stroeve Cecilie Mauritzen Anny Cazenave & Eric Rignot Nicholas R. Bates Josep G. Canadell & Michael R. Raupach Natalia Shakhova & Igor Semiletov CONTENTS Executive Summary 5 Overview 6 Arctic Climate Change 8 Key Findings of this Assessment 11 1. Atmospheric Circulation Feedbacks 17 2. Ocean Circulation Feedbacks 28 3. Ice Sheets and Sea-level Rise Feedbacks 39 4. Marine Carbon Cycle Feedbacks 54 5. Land Carbon Cycle Feedbacks 69 6. Methane Hydrate Feedbacks 81 Author Team 93 EXECUTIVE SUMMARY VER THE PAST FEW DECADES, the Arctic has warmed at about twice the rate of the rest of the globe. Human-induced climate change has Oaffected the Arctic earlier than expected. As a result, climate change is already destabilising important arctic systems including sea ice, the Greenland Ice Sheet, mountain glaciers, and aspects of the arctic carbon cycle including altering patterns of frozen soils and vegetation and increasing “Human-induced methane release from soils, lakes, and climate change has wetlands. The impact of these changes on the affected the Arctic Arctic’s physical systems, earlier than expected.” “There is emerging evidence biological and growing concern that systems, and human inhabitants is large and projected to grow arctic climate feedbacks throughout this century and beyond. affecting the global climate In addition to the regional consequences of arctic system are beginning climate change are its global impacts. Acting as the to accelerate warming Northern Hemisphere’s refrigerator, a frozen Arctic plays a central role in regulating Earth’s climate signifi cantly beyond system. -

Millions of Years of Greenland Ice Sheet History Recorded in Ocean Sediments
Umbruch 28.10.2011 21:21 Uhr Seite 141 Polarforschung 80 (3), 141 – 159, 2010 (erschienen 2011) Millions of Years of Greenland Ice Sheet History Recorded in Ocean Sediments by Jørn Thiede1,2, Catherine Jessen3, Paul Knutz3, Antoon Kuijpers3, Naja Mikkelsen3, Niels Nørgaard-Pedersen3, and Robert F. Spielhagen1 Abstract: Geological records from Tertiary and Quaternary terrestrial and glaciation, which is different from all previous well-docu- oceanic sections have documented the presence of ice caps and sea ice covers mented glacial events. The Greenland ice sheet is a remnant of both in the Southern and the Northern hemispheres since Eocene times, approximately since 45 Ma. In this paper focussing on Greenland we mainly the giant Northern Hemisphere last glacial maximum ice use the occurrences of coarse ice-rafted debris (IRD) in Quaternary and sheets (in our region composed of the Greenland Ice Sheet Tertiary ocean sediment cores to conclude on age and origin of the glaciers/ice with the adjacent Innuitian Ice Sheet to the West, which again sheets, which once produced the icebergs transporting this material into the adjacent ocean. Deep-sea sediment cores with their records of ice-rafting from was connected to the North American Laurentide Ice Sheet) off NE Greenland, Fram Strait and to the south of Greenland suggest the more and represents hence a spectacular anomaly. The future of or less continuous existence of the Greenland ice sheet since 18 Ma, maybe these ice sheets is, because of political, socio-economic and much longer, and hence far beyond the stratigraphic extent of the Greenland ice cores. -
Arctic Report Card 2020 the Sustained Transformation to a Warmer, Less Frozen and Biologically Changed Arctic Remains Clear
Arctic Report Card 2020 The sustained transformation to a warmer, less frozen and biologically changed Arctic remains clear DOI: 10.25923/MN5P-T549X R.L. Thoman, J. Richter-Menge, and M.L. Druckenmiller; Eds. December 2020 Richard L. Thoman, Jacqueline Richter-Menge, and Matthew L. Druckenmiller; Editors Benjamin J. DeAngelo; NOAA Executive Editor Kelley A. Uhlig; NOAA Coordinating Editor www.arctic.noaa.gov/Report-Card How to Cite Arctic Report Card 2020 Citing the complete report or Executive Summary: Thoman, R. L., J. Richter-Menge, and M. L. Druckenmiller, Eds., 2020: Arctic Report Card 2020, https://doi.org/10.25923/mn5p-t549. Citing an essay (example): Frey, K. E., J. C. Comiso, L. W. Cooper, J. M. Grebmeier, and L. V. Stock, 2020: Arctic Ocean primary productivity: The response of marine algae to climate warming and sea ice decline. Arctic Report Card 2020, R. L. Thoman, J. Richter-Menge, and M. L. Druckenmiller, Eds., https://doi.org/10.25923/vtdn-2198. (Note: Each essay has a unique DOI assigned) Front cover photo credits Center: Yamal Peninsula wildland fire, Siberia, 2017 – Jeffrey T. Kerby, National Geographic Society, Aarhus Institute of Advanced Studies, Aarhus University, Aarhus, Denmark Top Left: Large blocks of ice-rich permafrost fall onto the beach along the Laptev Sea coast, Siberia, 2017 – Pier Paul Overduin, Alfred Wegner Institute for Polar and Marine Research, Potsdam, Germany Top Right: R/V Polarstern during polar night, MOSAiC Expedition, 2019 – Matthew Shupe, Cooperative Institute for Research in Environmental Sciences, University of Colorado and NOAA Physical Sciences Laboratory, Boulder, Colorado, USA Mention of a commercial company or product does not constitute an endorsement by NOAA/OAR. -

Consequences of the 2019 Greenland Ice Sheet Melt Episode on Albedo
remote sensing Article Consequences of the 2019 Greenland Ice Sheet Melt Episode on Albedo Arthur Elmes 1,* , Charlotte Levy 1 , Angela Erb 1, Dorothy K. Hall 2, Ted A. Scambos 3 , Nicolo DiGirolamo 4 and Crystal Schaaf 1 1 School for the Environment, University of Massachusetts Boston, 100 William T. Morrissey Blvd, Boston, MA 02125, USA; [email protected] (C.L.); [email protected] (A.E.); [email protected] (C.S.) 2 Earth System Science Interdisciplinary Center, University of Maryland, College Park, MD 20470, USA; [email protected] 3 Earth Science Observation Center, Cooperative Institute for Research in Environmental Sciences, University of Colorado Boulder, Boulder, CO 80303, USA; [email protected] 4 Science Systems and Applications, Inc., Lanham, MD 20706, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-304-906-7946 Abstract: In mid-June 2019, the Greenland ice sheet (GrIS) experienced an extreme early-season melt event. This, coupled with an earlier-than-average melt onset and low prior winter snowfall over western Greenland, led to a rapid decrease in surface albedo and greater solar energy absorption over the melt season. The 2019 melt season resulted in significantly more melt than other recent years, even compared to exceptional melt years previously identified in the moderate-resolution imaging spectroradiometer (MODIS) record. The increased solar radiation absorbance in 2019 warmed the surface and increased the rate of meltwater production. We use two decades of satellite-derived albedo from the MODIS MCD43 record to show a significant and extended decrease in albedo in Greenland during 2019.