Botswana : Epidemiological Fact Sheets on HIV/AIDS and Sexually
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

B-E.00353.Pdf
© University of Hamburg 2018 All rights reserved Klaus Hess Publishers Göttingen & Windhoek www.k-hess-verlag.de ISBN: 978-3-933117-95-3 (Germany), 978-99916-57-43-1 (Namibia) Language editing: Will Simonson (Cambridge), and Proofreading Pal Translation of abstracts to Portuguese: Ana Filipa Guerra Silva Gomes da Piedade Page desing & layout: Marit Arnold, Klaus A. Hess, Ria Henning-Lohmann Cover photographs: front: Thunderstorm approaching a village on the Angolan Central Plateau (Rasmus Revermann) back: Fire in the miombo woodlands, Zambia (David Parduhn) Cover Design: Ria Henning-Lohmann ISSN 1613-9801 Printed in Germany Suggestion for citations: Volume: Revermann, R., Krewenka, K.M., Schmiedel, U., Olwoch, J.M., Helmschrot, J. & Jürgens, N. (eds.) (2018) Climate change and adaptive land management in southern Africa – assessments, changes, challenges, and solutions. Biodiversity & Ecology, 6, Klaus Hess Publishers, Göttingen & Windhoek. Articles (example): Archer, E., Engelbrecht, F., Hänsler, A., Landman, W., Tadross, M. & Helmschrot, J. (2018) Seasonal prediction and regional climate projections for southern Africa. In: Climate change and adaptive land management in southern Africa – assessments, changes, challenges, and solutions (ed. by Revermann, R., Krewenka, K.M., Schmiedel, U., Olwoch, J.M., Helmschrot, J. & Jürgens, N.), pp. 14–21, Biodiversity & Ecology, 6, Klaus Hess Publishers, Göttingen & Windhoek. Corrections brought to our attention will be published at the following location: http://www.biodiversity-plants.de/biodivers_ecol/biodivers_ecol.php Biodiversity & Ecology Journal of the Division Biodiversity, Evolution and Ecology of Plants, Institute for Plant Science and Microbiology, University of Hamburg Volume 6: Climate change and adaptive land management in southern Africa Assessments, changes, challenges, and solutions Edited by Rasmus Revermann1, Kristin M. -

The Decline in the Role of Chieftainship in Elections Geoffrey Barei Democracy Research Project University of Botswana
The African e-Journals Project has digitized full text of articles of eleven social science and humanities journals. This item is from the digital archive maintained by Michigan State University Library. Find more at: http://digital.lib.msu.edu/projects/africanjournals/ Available through a partnership with Scroll down to read the article. Pula: Botswana Journal of African Studies, Vol.14 No,1 (2000) The decline in the role of chieftainship in elections Geoffrey Barei Democracy Research Project University of Botswana Abstract This article focuses on three districts of Botswana, namely Central District, Ngwaketse District and Kgatleng District. It argues that as a result of the role played by the institution of chieftainship in elections, certain voting paltems that are discussed in the conceptual framework can be associated with it. The extent to which chieftainship has influenced electoral outcomes varies from one area to another. Introduction Chieftainship was the cornerstone of Botswana's political life, both before and during the colonial era, After independence in 1966 the institution underwent drastic reforms in terms of role, influence and respect Despite the introduction of a series of legislation by the post-colonial government that has curtailed and eroded the power of chiefs, it still plays a crucial role in the lives of ordinary people in rural areas, Sekgoma (1993:413) argues that the reform process that has affected chieftainship so far is irreversible, The government is not under pressure to repeal parts of the Acts that -

Social and Economie Change in a Tswana Village
social and economie change in a tswana village k. f. m. kooi j ma n SOCIAL AND ECONOMIC CHANCE IN A TSWANA VILLAGE Kunnie Kooijman AFRIKA - STUDIECENTRUM LEIDEN 11 ABSTRACT This dissertation is a descriptive study of Bokaa, a village of 1976 inhabitants situated in the Kgatleng district of Botswana. Bokaa was selected for an analysis and description of social and economie change since relatively much is known of the Kgatleng of thirty to forty years ago through the justly famous writings of Isaac Schapera and since the village has had relatively much contact with modernizing influences. It was not intended to present' a static picture of a 'before' and an 'after' but rather to isolate the processes of change which have led to the present social structure. By means of historical records, oral tradition and lifehistories it was possible to analyse the major historical processes which have taken place since 1892, the date the village was founded. The social and economie structure of Bokaa today was studied by means of participant observation, a questionnaire, interviewing, the collection of case-studies and genealogies, and the consultation of the relevant literature. The major conclusions of the study are that the corporate groups of the traditional social structure are breaking down and that the growth of individualism has become a significant feature of the society. In economie activities this is apparent because kinship co-operation has largely diappeared and individuals make their own arrangements with the aim of realising the greatest benefit to themselves. In the kinship realm it is noticeable since the coporate unity of the ward, family- group and lineage segment has weakened considerably and since individuals increasingly seek to manipulate their kinship bonds and duties to their own advantage. -
Kgatleng SUB District
Kgatleng SUB District VOL 5.0 KGATLENG SUB DISTRICT Population and Housing Census 2011 Selected Indicators for Villages and Localities ii i Population and Housing Census 2011 [ Selected indicators ] Kgatleng Sub District Population and Housing Census 2011 [Selected Indicators] Kgatleng Sub District 3 Table of Contents Kgatleng Sub District Population And Housing Census 2011: Selected Indicators For Villages And Localities Preface 3 VOL 5,0 1.0 Background and Commentary 6 1.1 Background to the Report 6 Published by 1.2 Importance of the Report 6 STATISTICS BOTSWANA Private Bag 0024, Gaborone 2.0 Population Distribution 6 Phone: (267)3671300, 3.0 Population Age Structure 6 Fax: (267) 3952201 Email: [email protected] 3.1 The Youth 7 Website: www.cso.gov.bw/cso 3.2 The Elderly 7 4.0 Annual Growth Rate 7 5.0 Household Size 7 COPYRIGHT RESERVED 6.0 Marital Status 8 7.0 Religion 8 Extracts may be published if source is duly acknowledged 8.0 Disability 9 9.0 Employment and Unemployment 9 10.0 Literacy 10 ISBN: 978-99968-429-7-9 11.0 Orphan-hood 10 12.0 Access to Drinking Water and Sanitation 10 12.1 Access to Portable Water 10 12.2 Access to Sanitation 11 13.0 Energy 11 13.1 Source of Fuel for Heating 11 13.2 Source of Fuel for Lighting 12 13.3 Source of Fuel for Cooking 12 14.0 Projected Population 2011 – 2026 13 Annexes 14 iii Population and Housing Census 2011 [ Selected indicators ] Kgatleng Sub District Population and Housing Census 2011 [Selected Indicators] Kgatleng Sub District 1 FIGURE 1: MAP OF KATLENG DISTRICT Preface This report follows our strategic resolve to disaggregate the 2011 Population and Housing Census report, and many of our statistical outputs, to cater for specific data needs of users. -
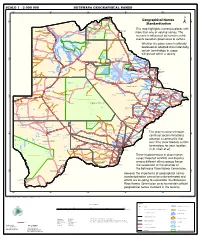
Geographical Names Standardization BOTSWANA GEOGRAPHICAL
SCALE 1 : 2 000 000 BOTSWANA GEOGRAPHICAL NAMES 20°0'0"E 22°0'0"E 24°0'0"E 26°0'0"E 28°0'0"E Kasane e ! ob Ch S Ngoma Bridge S " ! " 0 0 ' ' 0 0 ° Geographical Names ° ! 8 !( 8 1 ! 1 Parakarungu/ Kavimba ti Mbalakalungu ! ± n !( a Kakulwane Pan y K n Ga-Sekao/Kachikaubwe/Kachikabwe Standardization w e a L i/ n d d n o a y ba ! in m Shakawe Ngarange L ! zu ! !(Ghoha/Gcoha Gate we !(! Ng Samochema/Samochima Mpandamatenga/ This map highlights numerous places with Savute/Savuti Chobe National Park !(! Pandamatenga O Gudigwa te ! ! k Savu !( !( a ! v Nxamasere/Ncamasere a n a CHOBE DISTRICT more than one or varying names. The g Zweizwe Pan o an uiq !(! ag ! Sepupa/Sepopa Seronga M ! Savute Marsh Tsodilo !(! Gonutsuga/Gonitsuga scenario is influenced by human-centric Xau dum Nxauxau/Nxaunxau !(! ! Etsha 13 Jao! events based on governance or culture. achira Moan i e a h hw a k K g o n B Cakanaca/Xakanaka Mababe Ta ! u o N r o Moremi Wildlife Reserve Whether the place name is officially X a u ! G Gumare o d o l u OKAVANGO DELTA m m o e ! ti g Sankuyo o bestowed or adopted circumstantially, Qangwa g ! o !(! M Xaxaba/Cacaba B certain terminology in usage Nokaneng ! o r o Nxai National ! e Park n Shorobe a e k n will prevail within a society a Xaxa/Caecae/Xaixai m l e ! C u a n !( a d m a e a a b S c b K h i S " a " e a u T z 0 d ih n D 0 ' u ' m w NGAMILAND DISTRICT y ! Nxai Pan 0 m Tsokotshaa/Tsokatshaa 0 Gcwihabadu C T e Maun ° r ° h e ! 0 0 Ghwihaba/ ! a !( o 2 !( i ata Mmanxotae/Manxotae 2 g Botet N ! Gcwihaba e !( ! Nxharaga/Nxaraga !(! Maitengwe -

I UNIVERSITY of BOTSWANA FACULTY of AGRICULTURE DEPARTMENT of ANIMAL SCIENCE and PRODUCTION MILK PRODUCTION and CAPRINE MASTITIS
UNIVERSITY OF BOTSWANA FACULTY OF AGRICULTURE DEPARTMENT OF ANIMAL SCIENCE AND PRODUCTION MILK PRODUCTION AND CAPRINE MASTITIS OCCURANCE IN THE PRODUCTION STAGE OF THE GABORONE REGION GOAT MILK VALUE CHAIN BY WAZHA MUGABE MASTER OF SCIENCE IN ANIMAL SCIENCE (ANIMAL MANAGEMENT SYSTEMS) JUNE 2015 i UNIVERSITY OF BOTSWANA FACULTY OF AGRICULTURE DEPARTMENT OF ANIMAL SCIENCE AND PRODUCTION MILK PRODUCTION AND CAPRINE MASTITIS OCCURANCE IN THE PRODUCTION STAGE OF THE GABORONE REGION GOAT MILK VALUE CHAIN BY WAZHA MUGABE A dissertation presented in partial fulfillment of the requirement for the degree of Master of Science in Animal Science (Animal Management Systems) Main Supervisor: Dr. G.S. Mpapho Co-Supervisors: Prof. J.M. Kamau Prof. S.J Nsoso Dr. W. Mahabile June 2015 ii ABSTRACT T1he first study was initiated with the objectives of analyzing the production stage of the goat milk value chain and prevalence of caprine mastitis and its impact on the value chain. The study was conducted in the Gaborone agricultural region of Botswana. The primary data was collected using a participatory survey from purposefully selected samples of 91 farmers, 4 traders and 220 consumers through self-administered questionnaires. The results show that 88% of the farmers were subsistence orientated meanwhile semi-commercial and commercial farmers constituted 11% and 1 % respectively. A mean milk yield of 1.18L /goat/ per day was produced across farms and this was mostly channeled towards the 88.6% of non-purchasing consumers for home consumption. The average lactation length in the region was 5.37 months, therefore affecting milk consumption and availability patterns. -

Scanned PDF[8.20
Handbook for District Sanitation Coordinators Authors: Kebadire Basaako Ronald D. Parker Robert B. Waller James G. Wilson Editor: John van Nostrand ! L ! G RA R Y, Uï Í E K • ' i AT i O M A L R ¿ F í : ; : íi i\ 0 E ir CCN'VRÎÏ Por? cc v':.'n.;r¡¡¡ v V/AÍÍÍK SUPPLY i AfvT! ¿A; i ) r.o. 93 ;;;o! 2. „•'•;-'' d AD í he '-¡ague t ,1 1 1 i A n T.I. (070) 81 49 11 ext. 1 T 1 / 1 '4 ¿ RN: ño C" l Lop<Q ) LO: N/8- i 1- lo HA 3O2, Washington, DC December 1983 ACKNOWLEDGEMENTS The authors wish to acknowledge, with thanks, the advice and assistance of the Council Secretaries and Staff of Kgatleng and Southern Districts, the United States Agency for International Development (USAID), and the Technology Advisory Group (TAG) operating under the United Nations Development Programme Interregional Project INT/81/047 (executed by the World Bank). INTRODUCTION TO TAG REPRINT COPY The "Handbook for District Sanitation Coordinators" was originally prepared by two members of the USAID-funded team that had assisted in the development and implementation of the Environmental Sanitation and Protection (ESPP) Pilot Project in Botswana. TAG has been closely involved with ESPP since its inception, through participation in USAID project development missions and through technical support to the Senior Public Health Engineer (SPHE) in the Ministry of Local Government and Lands (MLGL) - an expatriate provided by UNDP through its project BOT/79/003. The SPHE supervised the project. TAG missions and headquarters staff were also responsible for the editing and production of the handbook. -

SABONET Report No 18
ii Quick Guide This book is divided into two sections: the first part provides descriptions of some common trees and shrubs of Botswana, and the second is the complete checklist. The scientific names of the families, genera, and species are arranged alphabetically. Vernacular names are also arranged alphabetically, starting with Setswana and followed by English. Setswana names are separated by a semi-colon from English names. A glossary at the end of the book defines botanical terms used in the text. Species that are listed in the Red Data List for Botswana are indicated by an ® preceding the name. The letters N, SW, and SE indicate the distribution of the species within Botswana according to the Flora zambesiaca geographical regions. Flora zambesiaca regions used in the checklist. Administrative District FZ geographical region Central District SE & N Chobe District N Ghanzi District SW Kgalagadi District SW Kgatleng District SE Kweneng District SW & SE Ngamiland District N North East District N South East District SE Southern District SW & SE N CHOBE DISTRICT NGAMILAND DISTRICT ZIMBABWE NAMIBIA NORTH EAST DISTRICT CENTRAL DISTRICT GHANZI DISTRICT KWENENG DISTRICT KGATLENG KGALAGADI DISTRICT DISTRICT SOUTHERN SOUTH EAST DISTRICT DISTRICT SOUTH AFRICA 0 Kilometres 400 i ii Trees of Botswana: names and distribution Moffat P. Setshogo & Fanie Venter iii Recommended citation format SETSHOGO, M.P. & VENTER, F. 2003. Trees of Botswana: names and distribution. Southern African Botanical Diversity Network Report No. 18. Pretoria. Produced by University of Botswana Herbarium Private Bag UB00704 Gaborone Tel: (267) 355 2602 Fax: (267) 318 5097 E-mail: [email protected] Published by Southern African Botanical Diversity Network (SABONET), c/o National Botanical Institute, Private Bag X101, 0001 Pretoria and University of Botswana Herbarium, Private Bag UB00704, Gaborone. -

Botswana Kweneng
Botswana Kweneng Kweneng District is located in the south-eastern part of Botswana. It borders Central District in northeast, Kgatleng District on the east, South-East District in southeast, Southern District in south, Kgalagadi District in the west, Ghanzi District in the north. The district is administered by a district administration and district council which are responsible for local administration. The seat of the district’s government is Molepolole.* Kweneng District Council (KwDC), through its Public Health Department is responsible for solid waste management in the district. KwDC provides waste collection and disposal services in some parts of the district. In other parts of the district, solid waste is collected by private operators under a franchise agreement with KwDC. In the district, there is one incineration facility (only for medical waste) and one engineered sanitary landfill located 30 kilometres from the district centre. The landfill is a regional landfill, i.e. solid waste from Kweneng District and other surrounding districts, including the capital Gaborone, are disposed at this landfill. Source: * Wikipedia, Kweneng District, accessed 15 April 2019, <https://en.wikipedia.org/wiki/Kweneng_District> Information Population 726,056 (2017) Population growth (annual %) N/A Area (km2)* 35,890 Climate Hot, semi-arid climate Main industries* Agriculture, mining, construction Currency** USD 1: BWP 10.65 (Botswana pula) (August 2018) Sources: * Wikipedia, Kweneng District, accessed 15 April 2019, <https://en.wikipedia.org/wiki/Kweneng_District> **Cuex.com Current SWM Situation Item Outline Institutional System Legal system The Waste Management Act (1998). Policy/Plan Currently, there is no waste management plan. Implementation KwDC provides sweeping, waste collection and disposal services. -

Geological Survey Department
( s MINISTRY OF COMMERCE, INDUSTRY AND WATER AFFAIRS ANNUAL REPORT OF THE GEOLOGICAL SURVEY DEPARTMENT FOR THE YEAR ENDED 31 ST DECEMBER 1968 • I GENERAL (a) Introduction The Geological Survey Department in the Republic of Botswana is a "non-integrated" element of the Ministry of Commerce, Industry and Water Affairs. Its headquarters are at Lobatse in southeastern Botswana, 4-7 miles south of the Botswana Government administrative headquarters at Gaborone. The fundamental aim of the Geological Survey is the assessment of the mineral resources and underground water supply resources of Botswana with the intention of stimulating the realisation of their economic poten~al. A necessary preliminary to the attainment of these objectives is a study of the rocks and the geological structure over the whole of the country. Regional geological mapping and the publication of maps and reports describing the geology of Botswana is thus the main, prime function of the Geological Survey Department. Mineral survey work is carried out and this includes field geological and geophysical survey of mineral occurrences supplemented by laboratory work; prospecting for new mineral deposits; render ing assistance to prospecting organisations and operating mines; and wherever possible fur thering interest in Botswana's mineral potential. A third major task of the Geological Survey is the development of underground water supplies and general hydrogeological survey. In underground water development work the Geological Survey carries out the siting of water boreholes after geological and geophysical investigations and then controls drilling of the selected sites to the stage where productive boreholes can be passed to another Department within the Ministry, which is responsible for equipping boreholes and for the maintenance of Government pumping units. -

List of Cities in Botswana
List of cities in Botswana The following is a list of cities and towns in Botswana with population of over 3,000 citizens. State capitals are shown in boldface. Population Female Rank Name District Census District [1] Male Population 2001. Population 1. Gaborone South-East District Gaborone 186,007 91,823 94,184 2. Francistown North-East District Francistown 83,023 40,134 42,889 3. Molepolole Kweneng District Kweneng East 62,739 28,617 34,122 4. Serowe Central District Central Serowe/Palapye 52,831 25,400 27,431 5. Selibe Phikwe Central District Selibe Phikwe 49,849 24,334 25,515 6. Maun North-West District Ngamiland East 49,822 23,714 26,108 7. Kanye Southern District Ngwaketse 48,143 22,451 25,692 8. Mahalapye Central District Central Mahalapye 43,538 21,120 22,418 9. Mogoditshane Kweneng District Kweneng East 40,753 20,972 19,781 10. Mochudi Kgatleng District Kgatleng 39,349 18,490 20,859 11. Lobatse South-East District Lobatse 29,689 14,202 15,487 12. Palapye Central District Central Serowe/Palapye 29,565 13,995 15,570 13. Ramotswa South-East District South East 25,738 12,027 13,711 14. Moshupa Southern District Ngwaketse 22,811 10,677 12,134 15. Tlokweng South-East District South East 22,038 10,568 11,470 16. Bobonong Central District Central Bobonong 21,020 9,877 11,143 17. Thamaga Kweneng District Kweneng East 20,527 9,332 11,195 18. Letlhakane Central District Central Boteti 19,539 9,848 9,691 19. -

Moswete N.Pdf
STAKEHOLDER PERSPECTIVES ON THE POTENTIAL FOR COMMUNITY-BASED ECOTOURISM DEVELOPMENT AND SUPPORT FOR THE KGALAGADI TRANSFRONTIER PARK IN BOTSWANA By NAOMI NOMSA MOSWETE A DISSERTATION PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY UNIVERSITY OF FLORIDA 2009 1 © 2009 Naomi Nomsa Moswete 2 To the memory of my beloved parents: Morwadi and Botha Moatshe, and to my husband, Mokgweetsi for his constant love and support during my academic journey. 3 ACKNOWLEDGMENTS My study program was made possible by the generous support of many individuals and organizations, which aided and financed this research. I am particularly indebted to the W.K. Kellogg Foundation via Leadership Initiatives for Southern Africa (LISA) without whom I could not have embarked on and completed this project. The study is a contribution to the Foundation’s mission in support of the development of healthy and sustainable rural communities in Southern Africa. I am deeply indebted to the Kellogg Foundation, which played a key role in all stages of my doctoral program – from course work to field data collection and analysis. I extend my sincere appreciation to all staff at AED in Botswana (Imelda, Disa, Thandi, Moniemang), and those in Washington DC, for the invaluable support they granted me throughout my academic and spiritual journeys. I would like to express my profound gratitude to Viwe Mtshontshi and Phillip Hesser for the patience, cooperation and kind support accorded me throughout my doctoral study at the University of Florida. I also thank the University of Botswana, which played an important role throughout this program.