BOTSWANA Country Operational Plan COP20
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

B-E.00353.Pdf
© University of Hamburg 2018 All rights reserved Klaus Hess Publishers Göttingen & Windhoek www.k-hess-verlag.de ISBN: 978-3-933117-95-3 (Germany), 978-99916-57-43-1 (Namibia) Language editing: Will Simonson (Cambridge), and Proofreading Pal Translation of abstracts to Portuguese: Ana Filipa Guerra Silva Gomes da Piedade Page desing & layout: Marit Arnold, Klaus A. Hess, Ria Henning-Lohmann Cover photographs: front: Thunderstorm approaching a village on the Angolan Central Plateau (Rasmus Revermann) back: Fire in the miombo woodlands, Zambia (David Parduhn) Cover Design: Ria Henning-Lohmann ISSN 1613-9801 Printed in Germany Suggestion for citations: Volume: Revermann, R., Krewenka, K.M., Schmiedel, U., Olwoch, J.M., Helmschrot, J. & Jürgens, N. (eds.) (2018) Climate change and adaptive land management in southern Africa – assessments, changes, challenges, and solutions. Biodiversity & Ecology, 6, Klaus Hess Publishers, Göttingen & Windhoek. Articles (example): Archer, E., Engelbrecht, F., Hänsler, A., Landman, W., Tadross, M. & Helmschrot, J. (2018) Seasonal prediction and regional climate projections for southern Africa. In: Climate change and adaptive land management in southern Africa – assessments, changes, challenges, and solutions (ed. by Revermann, R., Krewenka, K.M., Schmiedel, U., Olwoch, J.M., Helmschrot, J. & Jürgens, N.), pp. 14–21, Biodiversity & Ecology, 6, Klaus Hess Publishers, Göttingen & Windhoek. Corrections brought to our attention will be published at the following location: http://www.biodiversity-plants.de/biodivers_ecol/biodivers_ecol.php Biodiversity & Ecology Journal of the Division Biodiversity, Evolution and Ecology of Plants, Institute for Plant Science and Microbiology, University of Hamburg Volume 6: Climate change and adaptive land management in southern Africa Assessments, changes, challenges, and solutions Edited by Rasmus Revermann1, Kristin M. -
Status of Wildlife Populations and Land Degradation in Botswana’S Forest Reserves and Chobe District
_______________________________________________________________________________ STATUS OF WILDLIFE POPULATIONS AND LAND DEGRADATION IN BOTSWANA’S FOREST RESERVES AND CHOBE DISTRICT Michael Chase Elephants Without Borders PO Box 682 Kasane Tel: ++267 6250505 Email: [email protected] April 2013 STATUS OF WILDLIFE POPULATIONS AND LAND DEGRADATION IN BOTSWANA’S FOREST RESERVES AND CHOBE DISTRICT Michael Chase 1,2 April 2013 1 Elephants Without Borders, P.O. Box 682, Kasane, Botswana, and 2 San Diego Zoo Institute for Conservation Research, 15600 San Pasqual Valley Road, Escondido, CA 92027-7000, U.S.A. Forest Conservation Botswana Elephants Without Borders Zoological Society of San Diego This survey was conducted jointly by Elephants Without Borders, Forest Conservation Botswana and, the Zoological Society of San Diego. The opinions expressed in this report are those of the author and do not necessarily represent those of Forest Conservation Botswana, the Zoological Society of San Diego or any of the donors who have helped fund this aerial survey. No part of this report may be reproduced without the prior written permission of the author and copyright owner(s). ii ACKNOWLEDGMENTS This wildlife aerial survey of the Chobe District was flown by Elephants Without Borders, and largely funded through a grant from Forest Conservation Botswana (FCB 000018). Additional funding was received from Zoological Society of San Diego, Botswana Wildlife Management Association, Mr. Brett Warren and Family, Mutual and Federal Insurance Botswana and Madeleine and Jerry Delman Cohen. I appreciate the assistance provided by Mr. E.B. Moabi, and Ms. M. Bolele from the Ministry of Environment, Wildlife and Tourism. DWNP personnel, Dr. Cyril Taolo, Fredrick Dipotso and Chobe National Park officers and wildlife scouts are recognized for their help. -

The Decline in the Role of Chieftainship in Elections Geoffrey Barei Democracy Research Project University of Botswana
The African e-Journals Project has digitized full text of articles of eleven social science and humanities journals. This item is from the digital archive maintained by Michigan State University Library. Find more at: http://digital.lib.msu.edu/projects/africanjournals/ Available through a partnership with Scroll down to read the article. Pula: Botswana Journal of African Studies, Vol.14 No,1 (2000) The decline in the role of chieftainship in elections Geoffrey Barei Democracy Research Project University of Botswana Abstract This article focuses on three districts of Botswana, namely Central District, Ngwaketse District and Kgatleng District. It argues that as a result of the role played by the institution of chieftainship in elections, certain voting paltems that are discussed in the conceptual framework can be associated with it. The extent to which chieftainship has influenced electoral outcomes varies from one area to another. Introduction Chieftainship was the cornerstone of Botswana's political life, both before and during the colonial era, After independence in 1966 the institution underwent drastic reforms in terms of role, influence and respect Despite the introduction of a series of legislation by the post-colonial government that has curtailed and eroded the power of chiefs, it still plays a crucial role in the lives of ordinary people in rural areas, Sekgoma (1993:413) argues that the reform process that has affected chieftainship so far is irreversible, The government is not under pressure to repeal parts of the Acts that -

Social and Economie Change in a Tswana Village
social and economie change in a tswana village k. f. m. kooi j ma n SOCIAL AND ECONOMIC CHANCE IN A TSWANA VILLAGE Kunnie Kooijman AFRIKA - STUDIECENTRUM LEIDEN 11 ABSTRACT This dissertation is a descriptive study of Bokaa, a village of 1976 inhabitants situated in the Kgatleng district of Botswana. Bokaa was selected for an analysis and description of social and economie change since relatively much is known of the Kgatleng of thirty to forty years ago through the justly famous writings of Isaac Schapera and since the village has had relatively much contact with modernizing influences. It was not intended to present' a static picture of a 'before' and an 'after' but rather to isolate the processes of change which have led to the present social structure. By means of historical records, oral tradition and lifehistories it was possible to analyse the major historical processes which have taken place since 1892, the date the village was founded. The social and economie structure of Bokaa today was studied by means of participant observation, a questionnaire, interviewing, the collection of case-studies and genealogies, and the consultation of the relevant literature. The major conclusions of the study are that the corporate groups of the traditional social structure are breaking down and that the growth of individualism has become a significant feature of the society. In economie activities this is apparent because kinship co-operation has largely diappeared and individuals make their own arrangements with the aim of realising the greatest benefit to themselves. In the kinship realm it is noticeable since the coporate unity of the ward, family- group and lineage segment has weakened considerably and since individuals increasingly seek to manipulate their kinship bonds and duties to their own advantage. -

Department of Road Transport and Safety Offices
DEPARTMENT OF ROAD TRANSPORT AND SAFETY OFFICES AND SERVICES MOLEPOLOLE • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Transport Inspectorate Tel: 5920148 Fax: 5910620 P/Bag 52 Molepolole Next to Molepolole Police MOCHUDI • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Transport Inspectorate P/Bag 36 Mochudi Tel : 5777127 Fax : 5748542 White House GABORONE Headquarters BBS Mall Plot no 53796 Tshomarelo House (Botswana Savings Bank) 1st, 2nd &3rd Floor Corner Lekgarapa/Letswai Road •Registration & Licensing of vehicles and drivers •Road safety (Public Education) Tel: 3688600/62 Fax : Fax: 3904067 P/Bag 0054 Gaborone GABORONE VTS – MARUAPULA • Registration & Licensing of vehicles and drivers • Driver Examination (Theory & Practical Tests) • Vehicle Examination Tel: 3912674/2259 P/Bag BR 318 B/Hurst Near Roads Training & Roads Maintenance behind Maruapula Flats GABORONE II – FAIRGROUNDS • Registration & Licensing of vehicles and drivers • Driver Examination : Theory Tel: 3190214/3911540/3911994 Fax : P/Bag 0054 Gaborone GABORONE - OLD SUPPLIES • Registration & Licensing of vehicles and drivers • Transport Permits • Transport Inspectorate Tel: 3905050 Fax :3932671 P/Bag 0054 Gaborone Plot 1221, Along Nkrumah Road, Near Botswana Power Corporation CHILDREN TRAFFIC SCHOOL •Road Safety Promotion for children only Tel: 3161851 P/Bag BR 318 B/Hurst RAMOTSWA •Registration & Licensing of vehicles and drivers •Driver Examination (Theory & Practical -
Directory of Financial Institutions Operating in Botswana As at December 31, 2019
PAPER 4 BANK OF BOTSWANA DIRECTORY OF FINANCIAL INSTITUTIONS OPERATING IN BOTSWANA AS AT DECEMBER 31, 2019 PREPARED AND DISTRIBUTED BY THE BANKING SUPERVISION DEPARTMENT BANK OF BOTSWANA Foreword This directory is compiled and distributed by the Banking Supervision Department of the Bank of Botswana. While every effort has been made to ensure the accuracy of the information contained in this directory, such information is subject to frequent revision, and thus the Bank accepts no responsibility for the continuing accuracy of the information. Interested parties are advised to contact the respective financial institutions directly for any information they require. This directory excludes collective investment undertakings and International Financial Services Centre non-bank entities, whose regulation and supervision falls within the purview of the Non-Bank Financial Institutions Regulatory Authority. Lesedi S Senatla DIRECTOR BANKING SUPERVISION DEPARTMENT 2 DIRECTORY OF FINANCIAL INSTITUTIONS OPERATING IN BOTSWANA TABLE OF CONTENTS 1. CENTRAL BANK ..................................................................................................................................... 5 2. COMMERCIAL BANKS ........................................................................................................................... 7 2.1 ABSA BANK BOTSWANA LIMITED ........................................................................................................... 7 2.2 AFRICAN BANKING CORPORATION OF BOTSWANA LIMITED .................................................................. -

The Big Governance Issues in Botswana
MARCH 2021 THE BIG GOVERNANCE ISSUES IN BOTSWANA A CIVIL SOCIETY SUBMISSION TO THE AFRICAN PEER REVIEW MECHANISM Contents Executive Summary 3 Acknowledgments 7 Acronyms and Abbreviations 8 What is the APRM? 10 The BAPS Process 12 Ibrahim Index of African Governance Botswana: 2020 IIAG Scores, Ranks & Trends 120 CHAPTER 1 15 Introduction CHAPTER 2 16 Human Rights CHAPTER 3 27 Separation of Powers CHAPTER 4 35 Public Service and Decentralisation CHAPTER 5 43 Citizen Participation and Economic Inclusion CHAPTER 6 51 Transparency and Accountability CHAPTER 7 61 Vulnerable Groups CHAPTER 8 70 Education CHAPTER 9 80 Sustainable Development and Natural Resource Management, Access to Land and Infrastructure CHAPTER 10 91 Food Security CHAPTER 11 98 Crime and Security CHAPTER 12 108 Foreign Policy CHAPTER 13 113 Research and Development THE BIG GOVERNANCE ISSUES IN BOTSWANA: A CIVIL SOCIETY SUBMISSION TO THE APRM 3 Executive Summary Botswana’s civil society APRM Working Group has identified 12 governance issues to be included in this submission: 1 Human Rights The implementation of domestic and international legislation has meant that basic human rights are well protected in Botswana. However, these rights are not enjoyed equally by all. Areas of concern include violence against women and children; discrimination against indigenous peoples; child labour; over reliance on and abuses by the mining sector; respect for diversity and culture; effectiveness of social protection programmes; and access to quality healthcare services. It is recommended that government develop a comprehensive national action plan on human rights that applies to both state and business. 2 Separation of Powers Political and personal interests have made separation between Botswana’s three arms of government difficult. -
Kgatleng SUB District
Kgatleng SUB District VOL 5.0 KGATLENG SUB DISTRICT Population and Housing Census 2011 Selected Indicators for Villages and Localities ii i Population and Housing Census 2011 [ Selected indicators ] Kgatleng Sub District Population and Housing Census 2011 [Selected Indicators] Kgatleng Sub District 3 Table of Contents Kgatleng Sub District Population And Housing Census 2011: Selected Indicators For Villages And Localities Preface 3 VOL 5,0 1.0 Background and Commentary 6 1.1 Background to the Report 6 Published by 1.2 Importance of the Report 6 STATISTICS BOTSWANA Private Bag 0024, Gaborone 2.0 Population Distribution 6 Phone: (267)3671300, 3.0 Population Age Structure 6 Fax: (267) 3952201 Email: [email protected] 3.1 The Youth 7 Website: www.cso.gov.bw/cso 3.2 The Elderly 7 4.0 Annual Growth Rate 7 5.0 Household Size 7 COPYRIGHT RESERVED 6.0 Marital Status 8 7.0 Religion 8 Extracts may be published if source is duly acknowledged 8.0 Disability 9 9.0 Employment and Unemployment 9 10.0 Literacy 10 ISBN: 978-99968-429-7-9 11.0 Orphan-hood 10 12.0 Access to Drinking Water and Sanitation 10 12.1 Access to Portable Water 10 12.2 Access to Sanitation 11 13.0 Energy 11 13.1 Source of Fuel for Heating 11 13.2 Source of Fuel for Lighting 12 13.3 Source of Fuel for Cooking 12 14.0 Projected Population 2011 – 2026 13 Annexes 14 iii Population and Housing Census 2011 [ Selected indicators ] Kgatleng Sub District Population and Housing Census 2011 [Selected Indicators] Kgatleng Sub District 1 FIGURE 1: MAP OF KATLENG DISTRICT Preface This report follows our strategic resolve to disaggregate the 2011 Population and Housing Census report, and many of our statistical outputs, to cater for specific data needs of users. -

UNICEF Lesotho
Data Requirement Analysis and Data Mapping UNICEF Lesotho September 2018 PREPARED BY Ms. Paige Kirby Development Gateway, Inc. 1110 Vermont Ave NW Suite 500 Washington, DC 20008 USA Cover image: © UNICEF/UN04420/Marrion Table of Contents LIST OF ABBREVIATIONS 4 EXECUTIVE SUMMARY 5 I. INTRODUCTION 5 II. LESOTHO CONTEXT 6 III. DATA DEMAND 6 IV. DATA SUPPLY 7 V. DATA USE AND ECOSYSTEM OPPORTUNITIES 7 VI. CONCLUSION 7 INTRODUCTION 8 I. PROJECT BACKGROUND 8 A. DIAGNOSTIC REPORT OVERVIEW 8 II. PURPOSE AND INTENDED USE 9 LESOTHO CONTEXT 10 I. SITUATIONAL OVERVIEW 10 A. POLITICAL ECONOMY 11 II. STRATEGIC PRIORITIES AND PROCESSES 12 A. GOVERNMENT OF LESOTHO 12 B. UNICEF LESOTHO PROCESSES AND PRIORITIES 14 III. OTHER ECOSYSTEM ACTORS 16 IV. SECTION CONCLUSION 17 DATA DEMAND 18 I. INTRODUCTION 18 II. GOVERNMENT PRIORITIES 18 A. DATA DEMANDERS 18 B. DATA PRODUCERS 19 C. DATA DEMANDERS AND PRODUCERS 19 III. UNICEF PRIORITIES 21 A. OUTCOME AREA 1 22 B. OUTCOME AREA 2 23 C. OUTCOME AREA 3 24 D. OUTCOME AREA 4 25 IV. PROMINENT NEEDS 26 A. POLICY COMPLIANCE 26 B. LEADERSHIP 27 V. SECTION CONCLUSION 28 DATA SUPPLY 29 I. INTRODUCTION 29 II. EXISTING DATA SOURCES 29 | 2 A. GOVERNMENT DATA SOURCES 30 B. OTHER UNICEF DATA SOURCES 35 III. PROMINENT NEEDS 36 A. ACCESS 36 B. AVAILABILITY 37 C. TIMELINESS 39 D. QUALITY 40 E. CAPACITY 42 IV. SECTION CONCLUSION 44 DATA USE 45 I. INTRODUCTION 45 II. EXISTING PROCESSES 46 A. GOVERNMENT 46 B. UNICEF 46 C. MAPPING DEMAND AGAINST SUPPLY 46 III. PROMINENT NEEDS 48 A. CAPACITY 48 B. -
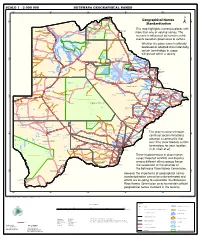
Geographical Names Standardization BOTSWANA GEOGRAPHICAL
SCALE 1 : 2 000 000 BOTSWANA GEOGRAPHICAL NAMES 20°0'0"E 22°0'0"E 24°0'0"E 26°0'0"E 28°0'0"E Kasane e ! ob Ch S Ngoma Bridge S " ! " 0 0 ' ' 0 0 ° Geographical Names ° ! 8 !( 8 1 ! 1 Parakarungu/ Kavimba ti Mbalakalungu ! ± n !( a Kakulwane Pan y K n Ga-Sekao/Kachikaubwe/Kachikabwe Standardization w e a L i/ n d d n o a y ba ! in m Shakawe Ngarange L ! zu ! !(Ghoha/Gcoha Gate we !(! Ng Samochema/Samochima Mpandamatenga/ This map highlights numerous places with Savute/Savuti Chobe National Park !(! Pandamatenga O Gudigwa te ! ! k Savu !( !( a ! v Nxamasere/Ncamasere a n a CHOBE DISTRICT more than one or varying names. The g Zweizwe Pan o an uiq !(! ag ! Sepupa/Sepopa Seronga M ! Savute Marsh Tsodilo !(! Gonutsuga/Gonitsuga scenario is influenced by human-centric Xau dum Nxauxau/Nxaunxau !(! ! Etsha 13 Jao! events based on governance or culture. achira Moan i e a h hw a k K g o n B Cakanaca/Xakanaka Mababe Ta ! u o N r o Moremi Wildlife Reserve Whether the place name is officially X a u ! G Gumare o d o l u OKAVANGO DELTA m m o e ! ti g Sankuyo o bestowed or adopted circumstantially, Qangwa g ! o !(! M Xaxaba/Cacaba B certain terminology in usage Nokaneng ! o r o Nxai National ! e Park n Shorobe a e k n will prevail within a society a Xaxa/Caecae/Xaixai m l e ! C u a n !( a d m a e a a b S c b K h i S " a " e a u T z 0 d ih n D 0 ' u ' m w NGAMILAND DISTRICT y ! Nxai Pan 0 m Tsokotshaa/Tsokatshaa 0 Gcwihabadu C T e Maun ° r ° h e ! 0 0 Ghwihaba/ ! a !( o 2 !( i ata Mmanxotae/Manxotae 2 g Botet N ! Gcwihaba e !( ! Nxharaga/Nxaraga !(! Maitengwe -

Geology and Paragenesis of the Boseto Copper Deposits, Kalahari
GEOLOGY AND PARAGENESIS OF THE BOSETO COPPER DEPOSITS, KALAHARI COPPERBELT, NORTHWEST BOTSWANA by Wesley S. Hall A thesis submitted to the Faculty and the Board of Trustees of the Colorado School of Mines in partial fulfillment of the requirements for the degree of Master of Science (Geology) Golden, Colorado Date _________________________ Signed: ______________________________ Wesley S. Hall Signed: ______________________________ Dr. Murray W. Hitzman Thesis Advisor Golden, Colorado Date _________________________ Signed: ______________________________ Dr. John D. Humphrey Associate Professor and Head Department of Geology & Geological Engineering ii ABSTRACT Detailed lithostratigraphic, structural, and petrographic studies coupled with fluid inclusion and stable isotopic analyses and geochronological studies indicate that the Boseto copper deposits formed initially during diagenesis as metalliferous brines ascended along basin faults and moved along a stratigraphic redox boundary between continental red beds and an overlying reduced marine siliciclastic sequence. The hanging wall rocks to copper-silver ore zones comprise comprises a series of at least three stacked coarsening upwards cycles deposited in a deltaic depositional setting. Early copper mineralization may have been accompanied by regionally extensive albitization. Later multiple pulses of faulting and hydrothermal fluid flow associated with a southeast-vergent folding event in the Ghanzi-Chobe belt resulted in extensive networks of bedding-parallel and discordant quartz-carbonate-(Cu-Fe-sulfide) veins. This contractional deformation-related vein and shear system was responsible for significant remobilization of pre-existing vertically and laterally zoned copper sulfide minerals into high- grade zones by hot (250-300˚C), syn-orogenic, metamorphic-derived hydrothermal fluids. Orientation analysis indicates that the mineralized veins probably formed in association with a flexural slip folding processes. -

Toward Sustainable Conservation And
Human–Wildlife Interactions 12(2):220–232, Fall 2018 • digitalcommons.usu.edu/hwi Toward sustainable conservation and management of human–wildlife interactions in the Mmadinare Region of Botswana: villagers’ perceptions on challenges and prospects Oitshepile MmaB Modise, Department of Adult Education, University of Botswana, 4775 Notwane Rd., Gaborone, Botswana [email protected] Rebecca Nthogo Lekoko, Department of Adult Education, University of Botswana, 4775 Notwane Rd., Gaborone, Botswana Olekae Tsompi Thakadu, Okavango Research Institute, University of Botswana, 8173 Shorobe Rd., Sexaxa, Maun, Botswana Masego Ayo Mpotokwane, Department of Environmental Sciences, University of Botswana, 4775 Notwane Rd., Gaborone, Botswana Abstract: Human–wildlife conflicts are increasing globally. The increase in conflicts has been attributed to growing human and wildlife populations and a per capita increase in the consumption of natural resources. In Botswana, conflicts between humans and elephants (Loxodonta africana) are increasing. The growing human population (2.2 million) is encroaching on the animals’ already restricted range. Concomitantly, more elephants are adversely affecting arable agriculture production. To better understand the magnitude and intensity of human–wildlife interactions with elephants and other native wildlife species in Botswana, we collected data through community forum conducted July 17–18, 2017 at a “Kgotla” meeting in Mmadinare, a village in the Central District of Botswana. Mmadinare has experienced increased human–wildlife conflicts, mainly related to elephants. TheKgotla is the traditional community meeting place in Botswana villages. The Kgotla provides for freedom of expression, transparent debate, officialdom, and is the official seat for the village leaders. Issues discussed at the Kgotla are highly regarded, and individuals who have discussions do so seriously.