Evaluating Disinfectants for Use Against the COVID-19 Virus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Chemical Disinfectants for Biohazardous Materials (3/21)
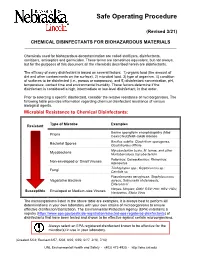
Safe Operating Procedure (Revised 3/21) CHEMICAL DISINFECTANTS FOR BIOHAZARDOUS MATERIALS ____________________________________________________________________________ Chemicals used for biohazardous decontamination are called sterilizers, disinfectants, sanitizers, antiseptics and germicides. These terms are sometimes equivalent, but not always, but for the purposes of this document all the chemicals described herein are disinfectants. The efficacy of every disinfectant is based on several factors: 1) organic load (the amount of dirt and other contaminants on the surface), 2) microbial load, 3) type of organism, 4) condition of surfaces to be disinfected (i.e., porous or nonporous), and 5) disinfectant concentration, pH, temperature, contact time and environmental humidity. These factors determine if the disinfectant is considered a high, intermediate or low-level disinfectant, in that order. Prior to selecting a specific disinfectant, consider the relative resistance of microorganisms. The following table provides information regarding chemical disinfectant resistance of various biological agents. Microbial Resistance to Chemical Disinfectants: Type of Microbe Examples Resistant Bovine spongiform encephalopathy (Mad Prions Cow) Creutzfeldt-Jakob disease Bacillus subtilis; Clostridium sporogenes, Bacterial Spores Clostridioides difficile Mycobacterium bovis, M. terrae, and other Mycobacteria Nontuberculous mycobacterium Poliovirus; Coxsackievirus; Rhinovirus; Non-enveloped or Small Viruses Adenovirus Trichophyton spp.; Cryptococcus sp.; -

Decontamination of Rooms, Medical Equipment and Ambulances Using an Aerosol of Hydrogen Peroxide Disinfectant B.M
Journal of Hospital Infection (2006) 62, 149–155 www.elsevierhealth.com/journals/jhin Decontamination of rooms, medical equipment and ambulances using an aerosol of hydrogen peroxide disinfectant B.M. Andersena,*, M. Rascha, K. Hochlina, F.-H. Jensenb, P. Wismarc, J.-E. Fredriksend aDepartment of Hospital Infection, Ulleva˚l University Hospital, Oslo, Norway bDivision of Pre-hospital Care, Ulleva˚l University Hospital, Oslo, Norway cDepartment of Medical Equipment, Ulleva˚l University Hospital, Oslo, Norway dHealth and Environment AS, Oslo, Norway Received 17 November 2004; accepted 1 July 2005 KEYWORDS Summary A programmable device (Sterinis, Gloster Sante Europe) Room decontamina- providing a dry fume of 5% hydrogen peroxide (H2O2) disinfectant was tion; Ambulance tested for decontamination of rooms, ambulances and different types of decontamination; medical equipment. Pre-set concentrations were used according to the Medical equipment decontamination; volumes of the rooms and garages. Three cycles were performed with Hydrogen peroxide increasing contact times. Repetitive experiments were performed using fume decontamina- Bacillus atrophaeus (formerly Bacillus subtilis) Raven 1162282 spores to tion; Spore test control the effect of decontamination; after a sampling plan, spore strips were placed in various positions in rooms, ambulances, and inside and outside the items of medical equipment. Decontamination was effective in 87% of 146 spore tests in closed test rooms and in 100% of 48 tests in a surgical department when using three cycles. One or two cycles had no effect. The sporicidal effect on internal parts of the medical equipment was only 62.3% (220 tests). When the devices were run and ventilated during decontamination, 100% (57/57) of spore strips placed inside were decontaminated. -

Safer Disinfectant Use in Child Care and Schools During the COVID-19 Pandemic
Safer Disinfectant Use in Child Care and Schools During the COVID-19 Pandemic Vickie Leonard, PhD Environmental Health in Early Care and Educaon Project, Western States Pediatric Environmental Health Specialty Unit (WSPEHSU) 1 Why Should We Be Concerned about Environmental Health in ECE? 2 Why Should We Be Concerned about Environmental Health in ECE? • There are 8 million children in child care centers in the U.S. A child may spend up to 12,500 hours in an ECE facility. A million child care providers work in these centers in the U.S. Half are child-bearing age. • Many toxicants found in child care facilities are not addressed in state child care health and safety regulations. • No agency at the state or federal level is charged with ensuring children’s health and safety in and around schools and ECE facilities. • No systematic means exists for collecting data on environmental exposures in these buildings. • Teachers have more protection in these buildings (unions, OSHA) than children do 3 Why Should We Be Concerned about Environmental Health in ECE? • Many people think that adults and children are exposed to, and affected by, toxic chemicals in the same way. • This is not the case. • Children • have higher exposures to toxicants in the environment, • are more vulnerable to the effects of those toxicants than adults. 4 Cleaning and Disinfec?ng Products: A Major Source of Exposure in Child Care and Schools • Products used to clean, sanitize and disinfect child care facilities and schools are a good example of the pervasive and unregulated use of toxic chemicals that put the health of our children at risk. -

FDA-2015-N-0101; and FDA-2016-N-0124
DE PARTMENT OF HEALTH AND HUMAN SERVICES Food and Drug Administration Silver Spring MD 20993 November 18, 2020 Docket Nos. FDA-1975-N-0012; FDA-2015-N-0101; and FDA-2016-N-0124 The American Cleaning Institute Attention: James Kim, PhD Vice President, Science and Regulatory Affairs 1401 H Street, N.W. Suite 700 Washington, D.C. 20005 Re: Benzalkonium Chloride, Benzethonium Chloride, Chloroxylenol, Ethanol, and Povidone-Iodine Dear Dr. Kim: This letter responds to The American Cleaning Institute’s (ACI’s) July 14, 2020 communication regarding the deferral from final rulemaking under the over-the-counter (OTC) Drug Review on benzalkonium chloride, benzethonium chloride, chloroxylenol, ethanol, and povidone-iodine for use in nonprescription (often referred to as over-the-counter or OTC) consumer antiseptic wash, health care antiseptic, and consumer antiseptic rub drug products. In March 2016, FDA issued letters granting requests to defer three active ingredients— benzalkonium chloride, benzethonium chloride, and chloroxylenol—from inclusion in the final rulemaking for the December 2013 proposed rule for OTC consumer antiseptic washes (78 FR 76444). Similarly, in January 2017, FDA issued letters granting requests to defer six active ingredients—benzalkonium chloride, benzethonium chloride, chloroxylenol, ethanol, povidone- iodine, and isopropyl alcohol—from inclusion in the final rulemaking for the May 2015 proposed rule for OTC health care antiseptics (80 FR 25166). In October 2017, FDA issued letters granting requests to defer three active -

Silver As a Drinking-Water Disinfectant
Silver as a drinking-water disinfectant Silver as a drinking-water disinfectant Alternative drinking-water disinfectants: silver ISBN 978-92-4-151369-2 © World Health Organization 2018 Some rights reserved. This work is available under the Creative Commons Attribution- NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. Alternative drinking-water disinfectants: bromine, iodine and silver. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris. Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. -

Which Disinfectants Work Best Against C. Difficile?
Science at Your Doorstep WHICH DISINFECTANTS WORK BEST AGAINST C. DIFFICILE? Summary: In healthcare facilities, Clostridium difficile infections spread by transmission of bacterial spores. Appropriate sporicidal disinfectants are needed to prevent development of clusters and outbreaks. In this study, researchers in The Netherlands compared the effectiveness of 4 different disinfectant classes on killing distinctive C. difficile spores. They published their results in the respected journal, Antimicrobial Resistance & Infection Control. Hydrogen peroxide disinfectant wipes showed the highest bactericidal activity. Publication Description: According to the study, a dilution of sodium hypochlorite (chlorine bleach) has historically been used in hospitals to disinfect areas contaminated with C. difficile spores. But the authors state that “hypochlorite has to be used in excessive concentrations to be effective, thereby increasing its toxic and corrosive properties.” So the authors searched for alternative disinfectant types to eliminate C. difficile spores. The 4 different disinfectant compounds tested were: 1. Glucoprotamin 2. Hydrogen peroxide 3. Ethanol/propane/amino propyl glycine 4. Didecyldimonium chloride/benzalkonium chloride/biguanide (quat) Tiles were contaminated with a solution containing 5x106 CFU/ml spores of C. difficile. The tiles were left to dry for an hour and then wiped or sprayed with one of the sprays or wipes as intended by the manufacturers. After 5 minutes, microbiological cultures were performed. Conclusion: The authors concluded that for each active ingredient, the wipes performed better than the sprays. In general, impregnated cleaning/disinfection wipes performed better than ready-to-use sprays. Wipes with hydrogen peroxide showed the highest bactericidal activity. Reference: See article at: Antimicrobial Resistance & Infection Control; Volume 6, No. -

Infection Prevention & Control Chlorhexidine
Winnipeg Regional Health Authority Acute Care Infection Prevention & Control Manual INFECTION PREVENTION & CONTROL CHLORHEXIDINE GLUCONATE CONCENTRATION FOR HAND HYGIENE COMMUNICATION FORM PART 1: ISSUE & RECOMMENDATIONS Issue: The WRHA Infection Prevention and Control program (IP&C) was requested to research and recommend acceptable concentrations of chlorhexidine gluconate (CHG) (2% versus 4%) for hand hygiene in all programs within WRHA sites, to ensure appropriate products are being used, and facilitate standardization. Recommendations: Use 2% CHG hand cleansers for hand hygiene when antimicrobial hand soap is indicated. Do NOT use 4% CHG for hand hygiene as the minimal improvement in efficacy (from 2%), does not warrant the increased frequency of skin irritation and breakdown, which ultimately impedes effective hand hygiene practices. PART 2: BACKGROUND: DISCUSSION OF ISSUE, OPTIONS AND ANALYSIS & REFERENCES Discussion of Issue: There are several different hand hygiene products used within and between WRHA sites. All areas should adhere to recommended hand hygiene products, as determined by available evidence. There are differences in when specific hand hygiene products are indicated. It is important to identify the appropriate product to use for the appropriate reason, as supported by evidence. Options and Analysis: 1. CHG has a cumulative effect when applied to the skin. In hand hygiene, this effect remains and is sustained, especially when hand hygiene is repeated. 2% CHG is appropriate for hand antisepsis because of the cumulative effect.1 2. Literature regarding differences between 2% and 4% CHG identifies there is minimal difference in efficacy between 2% and 4% CHG for hand antisepsis and cleansing.2 3. The frequency of skin irritation is concentration dependent, with products containing 4% most likely to cause dermatitis when used frequently for hand antisepsis. -

U.S. EPA, Pesticide Product Label, 776 DISINFECTANT VIRUCIDE
, 1-ls-lf9 UNITED ST ATES ENVIRONMENTAL PROTECTION AGENCY Carroll Company 2900 West Kingsley Road Garland, TX 75041 Subject: 776 Disinfectant, Virucide and Cleaner EPA Registration No. 4313-22 Amendment Dated November 9, 1998 Attn: Linda Kirk Kirby Director, Regulatory Compliance The amendment referred to above, submitted in connection with registration under the Federal Insecticide, Fungicide and Rodenticide Act, as amended, is acceptable. A stamped copy of the label is enclosed for your records. Submit one (I) copy ofthe finished printed label before this product is released for shipment. If you have any questions concerning the comments in this letter, you should contact Zenobia Jones at (703) 308-6198. Sincerely, ) JJ~lvJHdL Velma Noble Product Manager 31 Regulatory Management Branch I Antimicrobial Division (751 OW) COHCURRI!HCI!S ::::} ·m·I~ .Q........ ................ - ....................................... -................................ _............................. DATE ) . \-1i.-9l1... ....... ................... ................. .................................................................................... OFFICIAL FILE COpy Primed Oft R~cye/~d Paper ~' '....,-. " DISINFECTANT, UIRUCIDE* AND CLEANER FOR HOSPITAL INSTITUTIONAL ACTIVE INGREDIENT: AND iNDUSTRIAL USE Alkyl (C14 50%, C12 40%, C16 10%) dimelhyl • benzyl ammonium chloride........... 3.3 Yo ·Hum8n immunodeficiency virus, Type 1 (HIV-l) INERT INGR~DIENTS .................. 96.7% KEEP OUT OF REACH OF CHILDREN DANGER See back panel for additional precautionary -

Estonian Statistics on Medicines 2016 1/41
Estonian Statistics on Medicines 2016 ATC code ATC group / Active substance (rout of admin.) Quantity sold Unit DDD Unit DDD/1000/ day A ALIMENTARY TRACT AND METABOLISM 167,8985 A01 STOMATOLOGICAL PREPARATIONS 0,0738 A01A STOMATOLOGICAL PREPARATIONS 0,0738 A01AB Antiinfectives and antiseptics for local oral treatment 0,0738 A01AB09 Miconazole (O) 7088 g 0,2 g 0,0738 A01AB12 Hexetidine (O) 1951200 ml A01AB81 Neomycin+ Benzocaine (dental) 30200 pieces A01AB82 Demeclocycline+ Triamcinolone (dental) 680 g A01AC Corticosteroids for local oral treatment A01AC81 Dexamethasone+ Thymol (dental) 3094 ml A01AD Other agents for local oral treatment A01AD80 Lidocaine+ Cetylpyridinium chloride (gingival) 227150 g A01AD81 Lidocaine+ Cetrimide (O) 30900 g A01AD82 Choline salicylate (O) 864720 pieces A01AD83 Lidocaine+ Chamomille extract (O) 370080 g A01AD90 Lidocaine+ Paraformaldehyde (dental) 405 g A02 DRUGS FOR ACID RELATED DISORDERS 47,1312 A02A ANTACIDS 1,0133 Combinations and complexes of aluminium, calcium and A02AD 1,0133 magnesium compounds A02AD81 Aluminium hydroxide+ Magnesium hydroxide (O) 811120 pieces 10 pieces 0,1689 A02AD81 Aluminium hydroxide+ Magnesium hydroxide (O) 3101974 ml 50 ml 0,1292 A02AD83 Calcium carbonate+ Magnesium carbonate (O) 3434232 pieces 10 pieces 0,7152 DRUGS FOR PEPTIC ULCER AND GASTRO- A02B 46,1179 OESOPHAGEAL REFLUX DISEASE (GORD) A02BA H2-receptor antagonists 2,3855 A02BA02 Ranitidine (O) 340327,5 g 0,3 g 2,3624 A02BA02 Ranitidine (P) 3318,25 g 0,3 g 0,0230 A02BC Proton pump inhibitors 43,7324 A02BC01 Omeprazole -

Release of Antimicrobial Agents from Glass Ionomer Cements
Y T E I C O S L BALKAN JOURNAL OF STOMATOLOGY A ISSN 1107 - 1141 IC G LO TO STOMA Release of Antimicrobial Agents from Glass Ionomer Cements SUMMARY Aleksandar Dimkov, Elizabeta Gjorgievska, The aim of this study was to determine the level of antimicrobial Aleksandar Fildishevski agents Benzalkonium Chloride and Cetylpyridinium Chloride released Faculty of Dentistry, Clinic for Pediatric and from ChemFlex, a conventional glass ionomer cement (GIC). The main null Preventive Dentistry, Skopje, FYROM hypothesis tested was that there is no release of antimicrobial agents into the surrounding medium. 3 groups of the conventional ChemFlex GIC of 5 samples each, with Benzalconium Chloride and CPC incorporated, were prepared - each group with a different percentage of the agents (1%, 2%, and 3%). The determination of the quantity of the antimicrobial agents was done by an UV- Spectrophotometer. The measurements were performed at 11 successive time intervals. The results of the statistical analysis point out that it is possible to incorporate these antimicrobial agents in conventional GIC, especially when the added percentage of the antimicrobial agents is 3%. ORIGINAL PAPERS (OP) Keywords: GIC; Antimicrobial Agents; UV-Spectrophotometry Balk J Stom, 2012; 16:84-89 Introduction application9. There are several studies dealing with the effect of incorporating chlorhexidine in different Because of the relatively frequent occurrence of concentrations and its combinations in GIC to improve recurrent caries after a restorative treatment, and because their antimicrobial properties10-14. of the huge number of cariogenic microorganisms There are only a few data in the literature referring existing in the oral cavity, which present a potential to the incorporation and release of other antimicrobial risk factor regarding the development of new carious components in GIC. -

Safer Disinfectant Use During the COVID-19 Pandemic
Safer Disinfectant Use During the COVID-19 Pandemic sing disinfectants on surfaces in your home or workplace can kill disease causing germs (bacteria and viruses), Ubut they may also have health risks. For example, many common disinfectants (like bleach, many disinfectant wipes) have chemicals in them that can cause or worsen asthma. no If someone If in your you can’t one is house If is or access safer sick at sick home: suspected products to be sick: Clean surfaces in your Clean surfaces, then disinfect If you don’t have access to a house with an all-purpose using one of the safer disinfec microfiber cloth, wash sponges or cleaner or soap, and a tants from the EPA’s Design for towels after every surface cleaned: microfiber cloth (available the Environment antimicrobial Clean sponges by online, in grocery stores pesticide list. and at big box stores). This washing in the dishwasher, or will get rid of most of the Look for these safer active soaking for one minute in germs on a surface and ingredients: 1/2 teaspoon of bleach, or avoids excess exposure to Citric Acid microwaving non-metallic, disinfectants. Hydrogen Peroxide soaking wet sponges for one minute. Disinfect after cleaning L-lactic acid surfaces that you touch Ethanol Wash towels in a basin or washing machine. when returning from Isopropanol the outdoors, prior to Peroxyacetic acid If you only have access to washing hands. or quaternary ammonia- Sodium Bisulfate. bleach based disinfectants: Apply to the surface and per the leave glistening wet for the Dilute disinfectants time listed on the product label. -

COVID-19: Guidelines on Disinfection of Common Public Places Including Offices
COVID-19: Guidelines on disinfection of common public places including offices Scope: This document aims to provide interim guidance about the environmental cleaning /decontamination of common public places including offices in areas reporting COVID-19. Coronavirus Disease 2019 (COVID -19) is an acute respiratory disease caused by a novel Coronavirus (SARS-CoV-2), transmitted in most instances through respiratory droplets, direct contact with cases and also through contaminated surfaces/objects. Though the virus survives on environmental surfaces for varied period of time, it gets easily inactivated by chemical disinfectants. In view of the above, the following guidelines are to be followed, especially in areas reporting COVID-19. For ease of implementation the guideline divided these areas into (i) indoor areas, (ii) outdoor areas and (iii) public toilets. 1. Indoor areas including office spaces Office spaces, including conference rooms should be cleaned every evening after office hours or early in the morning before the rooms are occupied. If contact surface is visibly dirty, it should be cleaned with soap and water prior to disinfection. Prior to cleaning, the worker should wear disposable rubber boots, gloves (heavy duty), and a triple layer mask. Start cleaning from cleaner areas and proceed towards dirtier areas. All indoor areas such as entrance lobbies, corridors and staircases, escalators, elevators, security guard booths, office rooms, meeting rooms, cafeteria should be mopped with a disinfectant with 1% sodium hypochlorite