Genome-Wide Postnatal Changes in Immunity Following Fetal Inflammatory Response
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Identification of ROBO2 As a Potential Locus Associated with Inhaled
Journal of Personalized Medicine Article Identification of ROBO2 as a Potential Locus Associated with Inhaled Corticosteroid Response in Childhood Asthma Natalia Hernandez-Pacheco 1,2,3,*,†, Mario Gorenjak 4 , Jiang Li 5 , Katja Repnik 4,6, Susanne J. Vijverberg 7,8,9, Vojko Berce 4,10 , Andrea Jorgensen 11, Leila Karimi 12 , Maximilian Schieck 13,14, Lesly-Anne Samedy-Bates 15,16, Roger Tavendale 17, Jesús Villar 3,18,19 , Somnath Mukhopadhyay 17,20, Munir Pirmohamed 21 , Katia M. C. Verhamme 12, Michael Kabesch 13, Daniel B. Hawcutt 22,23, Steve Turner 24 , Colin N. Palmer 17, Kelan G. Tantisira 5,25, Esteban G. Burchard 15,16, Anke H. Maitland-van der Zee 7,8,9 , Carlos Flores 1,3,26,27 , Uroš Potoˇcnik 4,6,*,‡ and Maria Pino-Yanes 2,3,27,‡ 1 Research Unit, Hospital Universitario N.S. de Candelaria, Universidad de La Laguna, Carretera General del Rosario 145, 38010 Santa Cruz de Tenerife, Spain; cfl[email protected] 2 Genomics and Health Group, Department of Biochemistry, Microbiology, Cell Biology and Genetics, Universidad de La Laguna, Avenida Astrofísico Francisco Sánchez s/n, Faculty of Science, Apartado 456, 38200 San Cristóbal de La Laguna, Spain; [email protected] 3 CIBER de Enfermedades Respiratorias, Instituto de Salud Carlos III, Avenida de Monforte de Lemos, 5, 28029 Madrid, Spain; [email protected] 4 Center for Human Molecular Genetics and Pharmacogenomics, Faculty of Medicine, University of Maribor, Taborska Ulica 8, 2000 Maribor, Slovenia; [email protected] (M.G.); [email protected] (K.R.); [email protected] -
Supplementary Data
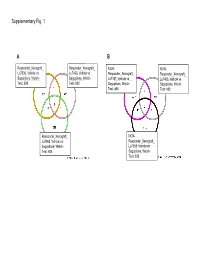
Supplementary Fig. 1 A B Responder_Xenograft_ Responder_Xenograft_ NON- NON- Lu7336, Vehicle vs Lu7466, Vehicle vs Responder_Xenograft_ Responder_Xenograft_ Sagopilone, Welch- Sagopilone, Welch- Lu7187, Vehicle vs Lu7406, Vehicle vs Test: 638 Test: 600 Sagopilone, Welch- Sagopilone, Welch- Test: 468 Test: 482 Responder_Xenograft_ NON- Lu7860, Vehicle vs Responder_Xenograft_ Sagopilone, Welch - Lu7558, Vehicle vs Test: 605 Sagopilone, Welch- Test: 333 Supplementary Fig. 2 Supplementary Fig. 3 Supplementary Figure S1. Venn diagrams comparing probe sets regulated by Sagopilone treatment (10mg/kg for 24h) between individual models (Welsh Test ellipse p-value<0.001 or 5-fold change). A Sagopilone responder models, B Sagopilone non-responder models. Supplementary Figure S2. Pathway analysis of genes regulated by Sagopilone treatment in responder xenograft models 24h after Sagopilone treatment by GeneGo Metacore; the most significant pathway map representing cell cycle/spindle assembly and chromosome separation is shown, genes upregulated by Sagopilone treatment are marked with red thermometers. Supplementary Figure S3. GeneGo Metacore pathway analysis of genes differentially expressed between Sagopilone Responder and Non-Responder models displaying –log(p-Values) of most significant pathway maps. Supplementary Tables Supplementary Table 1. Response and activity in 22 non-small-cell lung cancer (NSCLC) xenograft models after treatment with Sagopilone and other cytotoxic agents commonly used in the management of NSCLC Tumor Model Response type -

Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva
UCSF UC San Francisco Previously Published Works Title Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva. Permalink https://escholarship.org/uc/item/95h5g8mq Journal Cell reports, 33(7) ISSN 2211-1247 Authors Saitou, Marie Gaylord, Eliza A Xu, Erica et al. Publication Date 2020-11-01 DOI 10.1016/j.celrep.2020.108402 Peer reviewed eScholarship.org Powered by the California Digital Library University of California HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Cell Rep Manuscript Author . Author manuscript; Manuscript Author available in PMC 2020 November 30. Published in final edited form as: Cell Rep. 2020 November 17; 33(7): 108402. doi:10.1016/j.celrep.2020.108402. Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva Marie Saitou1,2,3, Eliza A. Gaylord4, Erica Xu1,7, Alison J. May4, Lubov Neznanova5, Sara Nathan4, Anissa Grawe4, Jolie Chang6, William Ryan6, Stefan Ruhl5,*, Sarah M. Knox4,*, Omer Gokcumen1,8,* 1Department of Biological Sciences, University at Buffalo, The State University of New York, Buffalo, NY, U.S.A 2Section of Genetic Medicine, Department of Medicine, University of Chicago, Chicago, IL, U.S.A 3Faculty of Biosciences, Norwegian University of Life Sciences, Ås, Viken, Norway 4Program in Craniofacial Biology, Department of Cell and Tissue Biology, School of Dentistry, University of California, San Francisco, CA, U.S.A 5Department of Oral Biology, School of Dental Medicine, University at Buffalo, The State University of New York, Buffalo, NY, U.S.A 6Department of Otolaryngology, School of Medicine, University of California, San Francisco, CA, U.S.A 7Present address: Weill-Cornell Medical College, Physiology and Biophysics Department 8Lead Contact SUMMARY Salivary proteins are essential for maintaining health in the oral cavity and proximal digestive tract, and they serve as potential diagnostic markers for monitoring human health and disease. -

1 Proteins of the XMRV Retrovirus Implicated in Chronic Fatigue
1 Proteins of the XMRV retrovirus implicated in chronic fatigue syndrome and prostate cancer are homologous to human proteins relevant to both conditions. C.J.Carter Flat 4, 20 Upper Maze Hill, Saint-Leonards on Sea , East Sussex, TN38 OLG [email protected] The XMRV retrovirus has been implicated in chronic fatigue syndrome and prostate cancer. A homology search comparing retroviral with human proteins revealed short contiguous amino acid strings (typically 5-8 aa) matching human proteins whose dysfunction might be expected to cause fatigue, including mitochondrial proteins related to oxidative phosphorylation, glutamate receptors and their synaptic scaffolds, muscular acetylcholine receptor scaffolds and structural proteins, components of the immune system, and phosphatidylinositol signalling inter alia. Viral proteins are also homologous to members of the oestrogen, peroxisome proliferator, and CREB activated receptor networks, all of which are implicated in prostate cancer, and to a protein, SRCAP, that controls the expression of the prostate- specific antigen. These short matches are often predicted to be antigenic, and antibodies to XMRV proteins may target their human homologues. This is supported by the presence of autoantibodies to muscarinic receptors , vimentin and LAMINB1 (all XMRV homologues) in chronic fatigue syndrome sufferers. Homologous XMRV proteins might also interfere with the protein interactomes of their human homologues. Viral mimicry of human proteins is extensive and often relevant to disease. For example Epstein-Barr viral proteins aligns with multiple sclerosis autoantigens, while HIV-1 proteins align with several components of the immune system. Mutant proteins in Huntington’s disease and cystic fibrosis also align with proteins from common phages or viruses. -

(12) Patent Application Publication (10) Pub. No.: US 2003/0198970 A1 Roberts (43) Pub
US 2003O19897OA1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2003/0198970 A1 Roberts (43) Pub. Date: Oct. 23, 2003 (54) GENOSTICS clinical trials on groups or cohorts of patients. This group data is used to derive a Standardised method of treatment (75) Inventor: Gareth Wyn Roberts, Cambs (GB) which is Subsequently applied on an individual basis. There is considerable evidence that a significant factor underlying Correspondence Address: the individual variability in response to disease, therapy and FINNEGAN, HENDERSON, FARABOW, prognosis lies in a person's genetic make-up. There have GARRETT & DUNNER been numerous examples relating that polymorphisms LLP within a given gene can alter the functionality of the protein 1300 ISTREET, NW encoded by that gene thus leading to a variable physiological WASHINGTON, DC 20005 (US) response. In order to bring about the integration of genomics into medical practice and enable design and building of a (73) Assignee: GENOSTIC PHARMA LIMITED technology platform which will enable the everyday practice (21) Appl. No.: 10/206,568 of molecular medicine a way must be invented for the DNA Sequence data to be aligned with the identification of genes (22) Filed: Jul. 29, 2002 central to the induction, development, progression and out come of disease or physiological States of interest. Accord Related U.S. Application Data ing to the invention, the number of genes and their configu rations (mutations and polymorphisms) needed to be (63) Continuation of application No. 09/325,123, filed on identified in order to provide critical clinical information Jun. 3, 1999, now abandoned. concerning individual prognosis is considerably less than the 100,000 thought to comprise the human genome. -

Bioactive Peptides Hidden in Human Salivary Proteins
Journal of Oral Biosciences 59 (2017) 71–79 Contents lists available at ScienceDirect Journal of Oral Biosciences journal homepage: www.elsevier.com/locate/job Review Bioactive peptides hidden in human salivary proteins Eiichi Saitoh a,n, Masayuki Taniguchi b, Akihito Ochiai b, Tetsuo Kato c, Akane Imai d, Satoko Isemura d a Graduate School of Technology, Niigata Institute of Technology, 1719 Fujihashi, Kashiwazaki, Niigata 945-1195, Japan b Department of Materials Science and Technology, Graduate School of Science and Technology, Niigata University, Niigata 950-2181, Japan c Laboratory of Chemistry, Tokyo Dental College, Tokyo 101-0062, Japan d Department of Dental Hygiene, The Nippon Dental University College at Niigata, Niigata 951-8580, Japan article info abstract Article history: Background: Extensive peptidomic studies of human saliva have resulted in considerable advances in the field Received 28 September 2016 of proteomics. As the next generation in salivary research, a comprehensive understanding of the biological Received in revised form functions of in vivo peptides generated by proteolysis in the oral cavity has been long awaited. A cyclopedic 4 November 2016 functional analysis of salivary peptides may bring promising therapeutic agents and novel clinical applications. Accepted 17 November 2016 Highlight: (1) This review article refers to bioactive peptides hidden in salivary parent proteins. (2) Functions of Available online 5 December 2016 the peptides as anti-microbial, anti-viral, wound-closing, and anti-pain are described. (3) Biological sig- Keywords: nificances of the repeated structures in salivary proline-rich proteins are emphasized. Human salivary proteome Conclusion: Human salivary proteins have the ability to generate bioactive peptides upon proteolytic cleavage. -
12P Deletion Spectrum Syndrome: a New Case Report Reinforces The
Leyser et al. Molecular Cytogenetics (2016) 9:75 DOI 10.1186/s13039-016-0278-0 CASE REPORT Open Access 12p deletion spectrum syndrome: a new case report reinforces the evidence regarding the potential relationship to autism spectrum disorder and related developmental impairments Marcio Leyser1*, Bruno Leonardo Dias1, Ana Luiza Coelho1, Marcio Vasconcelos2 and Osvaldo J. M. Nascimento2 Abstract Background: Autism Spectrum Disorders (ASD) now encompass a broad heterogeneous group of people who present in the early developmental years with a wide range of social and communication deficits, which are typically also associated with complex repetitive behaviors and circumscribed interests. The target goal is to heighten readers’ perception into the trend to personalize the distinct autistic and related developmental conditions encompassing the 12p region. Case Presentation: This is a case-report of a 4-year-old male who presented the core signs of ASD, which were thought to be related to a rare 12p13.2 deletion. We further reviewed the literature in order to outline the related developmental conditions in the 12p region. Aside from this patient reported here, we found an additional number of 43 cases described in the medical literature since 1974, that have been related to deletions in the 12p region. However, to the best of our knowledge, none of the previous had been specifically linked to the 12p13.2 band. Conclusions: The 12p deletion spectrum is rarely described as part of the selective genotypes thought to be related to ASD. Even inside of a small piece of the puzzle, there might be ample variation in the behavioral and clinical phenotypes of children and adults presenting with this particular genetic profile. -

PB #ISAG2017 1 @Isagofficial #ISAG2017 #ISAG2017
Bioinformatics · Comparative Genomics · Computational Biology Epigenetics · Functional Genomics · Genome Diversity · Geno Genome Sequencing · Immunogenetics · Integrative Geno · Microbiomics · Population Genomics · Systems Biolog Genetic Markers and Selection · Genetics and Dis Gene Editing · Bioinformatics · Comparative Computational Biology · Epigenetics · Fun Genome Diversity · Genome Sequeng Integrative Genomics · Microbiom Population Genomics · Syste Genetic Markers and Sel Genetics and Disease Gene Editing · Bi O’Brien Centre for Science Bioinformati and O’Reilly Hall, University College Dublin, Dublin, Ireland ABSTRACTMINI PROGRAMME BOOK www.isag.us/2017 PB #ISAG2017 1 @isagofficial #ISAG2017 #ISAG2017 Contents ORAL PRESENTATIONS 1 Animal Forensic Genetics Workshop 1 Applied Genetics and Genomics in Other Species of Economic Importance 3 Domestic Animal Sequencing and Annotation 5 Genome Edited Animals 8 Horse Genetics and Genomics 9 Avian Genetics and Genomics 12 Comparative MHC Genetics: Populations and Polymorphism 16 Equine Genetics and Thoroughbred Parentage Testing Workshop 19 Genetics of Immune Response and Disease Resistance 20 ISAG-FAO Genetic Diversity 24 Ruminant Genetics and Genomics 28 Animal Epigenetics 31 Cattle Molecular Markers and Parentage Testing 33 Companion Animal Genetics and Genomics 34 Microbiomes 37 Pig Genetics and Genomics 40 Novel, Groundbreaking Research/Methodology Presentation 44 Applied Genetics of Companion Animals 44 Applied Sheep and Goat Genetics 45 Comparative and Functional Genomics 47 Genetics -

Transcriptome Profiling Reveals the Complexity of Pirfenidone Effects in IPF
ERJ Express. Published on August 30, 2018 as doi: 10.1183/13993003.00564-2018 Early View Original article Transcriptome profiling reveals the complexity of pirfenidone effects in IPF Grazyna Kwapiszewska, Anna Gungl, Jochen Wilhelm, Leigh M. Marsh, Helene Thekkekara Puthenparampil, Katharina Sinn, Miroslava Didiasova, Walter Klepetko, Djuro Kosanovic, Ralph T. Schermuly, Lukasz Wujak, Benjamin Weiss, Liliana Schaefer, Marc Schneider, Michael Kreuter, Andrea Olschewski, Werner Seeger, Horst Olschewski, Malgorzata Wygrecka Please cite this article as: Kwapiszewska G, Gungl A, Wilhelm J, et al. Transcriptome profiling reveals the complexity of pirfenidone effects in IPF. Eur Respir J 2018; in press (https://doi.org/10.1183/13993003.00564-2018). This manuscript has recently been accepted for publication in the European Respiratory Journal. It is published here in its accepted form prior to copyediting and typesetting by our production team. After these production processes are complete and the authors have approved the resulting proofs, the article will move to the latest issue of the ERJ online. Copyright ©ERS 2018 Copyright 2018 by the European Respiratory Society. Transcriptome profiling reveals the complexity of pirfenidone effects in IPF Grazyna Kwapiszewska1,2, Anna Gungl2, Jochen Wilhelm3†, Leigh M. Marsh1, Helene Thekkekara Puthenparampil1, Katharina Sinn4, Miroslava Didiasova5, Walter Klepetko4, Djuro Kosanovic3, Ralph T. Schermuly3†, Lukasz Wujak5, Benjamin Weiss6, Liliana Schaefer7, Marc Schneider8†, Michael Kreuter8†, Andrea Olschewski1, -

Long-Term Oral Administration of LLHK, LHK, and HK Alters Gene Expression Profile and Restores Age-Dependent Atrophy and Dysfunction of Rat Salivary Glands
biomedicines Article Long-Term Oral Administration of LLHK, LHK, and HK Alters Gene Expression Profile and Restores Age-Dependent Atrophy and Dysfunction of Rat Salivary Glands 1, 1, 1, 2 Yasuko Ishikawa * , Tomasz D Pieczonka y, Aneta M Bragiel-Pieczonka z, Harumichi Seta , Tadahiro Ohkuri 2, Yumi Sasanuma 2 and Yuji Nonaka 2 1 Department of Medical Pharmacology, Institute of Biomedical Sciences, Tokushima University Graduate School, 3-18-15, Kuramoto-cho, Tokushima 770-8504, Japan; [email protected] (T.D.P.); [email protected] (A.M.B.-P.) 2 Suntory Global Innovation Center Ltd., Suntory World Research Center, 8-1-1 Seika-cho, Soraku-gun, Kyoto 619-0284, Japan; [email protected] (H.S.); [email protected] (T.O.); [email protected] (Y.S.); [email protected] (Y.N.) * Correspondence: [email protected] or [email protected]; Tel.: +80-3928-9628 Present address: Center of New Technologies, University of Warsaw, Banacha 2c, 02-097 Warsaw, Poland. y Present address: Department of Clinical Cytology, Centre of Medical Postgraduate Education, Marymoncka z 99/103, 01-813 Warsaw, Poland. Received: 26 January 2020; Accepted: 18 February 2020; Published: 20 February 2020 Abstract: Xerostomia, also known as dry mouth, is caused by a reduction in salivary secretion and by changes in the composition of saliva associated with the malfunction of salivary glands. Xerostomia decreases quality of life. In the present study, we investigated the effects of peptides derived from β-lactoglobulin C on age-dependent atrophy, gene expression profiles, and the dysfunction of salivary glands. -

A Missense in HSF2BP Causing Primary Ovarian Insufficiency Affects
RESEARCH ARTICLE A missense in HSF2BP causing primary ovarian insufficiency affects meiotic recombination by its novel interactor C19ORF57/BRME1 Natalia Felipe-Medina1†, Sandrine Caburet2,3†, Fernando Sa´ nchez-Sa´ ez1, Yazmine B Condezo1, Dirk G de Rooij4, Laura Go´ mez-H1, Rodrigo Garcia-Valiente1, Anne Laure Todeschini2,3, Paloma Duque1, Manuel Adolfo Sa´ nchez-Martin5,6, Stavit A Shalev7,8, Elena Llano1,9, Reiner A Veitia2,3,10*, Alberto M Penda´ s1* 1Molecular Mechanisms Program, Centro de Investigacio´n del Ca´ncer and Instituto de Biologı´a Molecular y Celular del Ca´ncer (CSIC-Universidad de Salamanca), Salamanca, Spain; 2Universitede Paris, Paris Cedex, France; 3Institut Jacques Monod, Universitede Paris, Paris, France; 4Reproductive Biology Group, Division of Developmental Biology, Department of Biology, Faculty of Science, Utrecht University, Utrecht, Netherlands; 5Transgenic Facility, Nucleus platform, Universidad de Salamanca, Salamanca, Spain; 6Departamento de Medicina, Universidad de Salamanca, Salamanca, Spain; 7The Genetic Institute, "Emek" Medical Center, Afula, Israel; 8Bruce and Ruth Rappaport Faculty of Medicine, Technion, Haifa, Israel; 9Departamento de Fisiologı´a y Farmacologı´a, Universidad de Salamanca, Salamanca, Spain; 10Universite´ Paris-Saclay, Institut de Biologie F. Jacob, Commissariat a` l’Energie Atomique, Fontenay aux Roses, France *For correspondence: [email protected] (RAV); [email protected] (AMP) Abstract Primary Ovarian Insufficiency (POI) is a major cause of infertility, but its etiology remains poorly understood. Using whole-exome sequencing in a family with three cases of POI, we †These authors contributed equally to this work identified the candidate missense variant S167L in HSF2BP, an essential meiotic gene. Functional analysis of the HSF2BP-S167L variant in mouse showed that it behaves as a hypomorphic allele Competing interests: The compared to a new loss-of-function (knock-out) mouse model. -

(12) United States Patent (10) Patent No.: US 7,919,467 B2 Ramakrishna Et Al
US0079 19467B2 (12) United States Patent (10) Patent No.: US 7,919,467 B2 Ramakrishna et al. (45) Date of Patent: Apr. 5, 2011 (54) CYTOTOXICT-LYMPHOCYTE-INDUCING OTHER PUBLICATIONS IMMUNOGENS FOR PREVENTION, Smith et al. (Nature Biotechnology 15:1222-1223 (1997)).* TREATMENT, AND DIAGNOSIS OF CANCER Brenner (Trends in Genetics 15:132-133 (1999)).* Voskoglou-Nomikos (Clin. Can. Res. 9:4227-4239 (2003)).* (75) Inventors: Venky Ramakrishna, Riegelsville, PA Dennis (Nature 442:739-741 (2006)).* (US); Mark M. Ross, Charlottesville, Cespcles et al. (Clin. Transl. Oncol. 8(5):318-329 (2006)).* VA (US); Ramila Philip, Ivyland, PA Talmadge et al. (Am. J. Pathol 170(3):793-804 (2007)).* (US); Lorraine H. Keller, Pipersville, clinicaltrials.gov search (ImmunoVaccine Technologies, Inc., pp. PA (US) 1-3; Jan. 29, 2011).* Adachiet al., 1992, Nucleic Acids Research, vol. 20, pp. 5297-5303. (73) Assignee: Immunotope, Inc., Doylestown, PA Boon, T. et al., Ann. Rev. Immunol. 12:337-365 (1994). Celluzzi, C. M. et al., J. Exp. Med., 183:283-287 (1996). (US) European Search Report, dated Jan. 26, 2005. Gilboa, E., Immunity, 11:263-270 (1999). (*) Notice: Subject to any disclaimer, the term of this Gluzman, Cell, 23:175 (1981). patent is extended or adjusted under 35 Harding, C. H. III, Eur, J. Immunol. 22:1865-1869 (1992). U.S.C. 154(b) by 560 days. Henderson R. A. etal, DirectIdentification of an Endogenous Peptide Reognized by Multiple HLA-A2.1 Specific Cytotoxic T Cells, (21) Appl. No.: 11/426,161 National Academy of Sciences, vol. 90, pp. 10275-10279 (Nov. 1993). (22) Filed: Jun.