ETV6 Mutations and Loss in AML-M0
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Minimal Residual Disease Detection in Childhood Precursor–B-Cell Acute Lymphoblastic Leukemia: Relation to Other Risk Factors
Leukemia (2003) 17, 1566–1572 & 2003 Nature Publishing Group All rights reserved 0887-6924/03 $25.00 www.nature.com/leu Minimal residual disease detection in childhood precursor–B-cell acute lymphoblastic leukemia: relation to other risk factors. A Children’s Oncology Group study MJ Borowitz1, DJ Pullen2, JJ Shuster3,4, D Viswanatha5, K Montgomery6, CL Willman5 and B Camitta7 1Johns Hopkins Medical Institutions, USA; 2University of Mississippi, USA; 3University of Florida, Gainesville FL, USA; 4Children’s Oncology Group, Arcadia, CA, USA; 5University of New Mexico, USA; 6Genzyme Genetics, Santa Fe, NM; and 7Milwaukee Childrens Hospital, USA Minimal residual disease (MRD) can be detected in the marrows prognostic significance at several time points. MRD levels at the of children undergoing chemotherapy either by flow cytometry end of induction are highly prognostic. Since intensification of or polymerase chain reaction. In this study, we used four-color therapy after successful induction can improve the outcome of flow cytometry to detect MRD in 1016 children undergoing 33 therapy on Children’s Oncology Group therapeutic protocols many patients with adverse prognostic features, it is possible for precursor–B-cell ALL. Compliance was excellent, with that a similar approach might benefit patients with MRD. For follow-up samples received at the end of induction on nearly these reasons, we have chosen to focus our MRD studies on 95% of cases; sensitivity of detection at this time point was at end-of-induction therapy. least 1/10,000 in more than 90% of cases. Overall, 28.6% of Although MRD and other measures of early response to patients had detectable MRD at the end of induction. -

Ubiquitin-Mediated Control of ETS Transcription Factors: Roles in Cancer and Development
International Journal of Molecular Sciences Review Ubiquitin-Mediated Control of ETS Transcription Factors: Roles in Cancer and Development Charles Ducker * and Peter E. Shaw * Queen’s Medical Centre, School of Life Sciences, University of Nottingham, Nottingham NG7 2UH, UK * Correspondence: [email protected] (C.D.); [email protected] (P.E.S.) Abstract: Genome expansion, whole genome and gene duplication events during metazoan evolution produced an extensive family of ETS genes whose members express transcription factors with a conserved winged helix-turn-helix DNA-binding domain. Unravelling their biological roles has proved challenging with functional redundancy manifest in overlapping expression patterns, a common consensus DNA-binding motif and responsiveness to mitogen-activated protein kinase signalling. Key determinants of the cellular repertoire of ETS proteins are their stability and turnover, controlled largely by the actions of selective E3 ubiquitin ligases and deubiquitinases. Here we discuss the known relationships between ETS proteins and enzymes that determine their ubiquitin status, their integration with other developmental signal transduction pathways and how suppression of ETS protein ubiquitination contributes to the malignant cell phenotype in multiple cancers. Keywords: E3 ligase complex; deubiquitinase; gene fusions; mitogens; phosphorylation; DNA damage 1. Introduction Citation: Ducker, C.; Shaw, P.E. Cell growth, proliferation and differentiation are complex, concerted processes that Ubiquitin-Mediated Control of ETS Transcription Factors: Roles in Cancer rely on careful regulation of gene expression. Control over gene expression is maintained and Development. Int. J. Mol. Sci. through signalling pathways that respond to external cellular stimuli, such as growth 2021, 22, 5119. https://doi.org/ factors, cytokines and chemokines, that invoke expression profiles commensurate with 10.3390/ijms22105119 diverse cellular outcomes. -

Hsa-Mir-125B-2 Is Highly Expressed in Childhood ETV6&Sol;RUNX1
Leukemia (2010) 24, 89–96 & 2010 Macmillan Publishers Limited All rights reserved 0887-6924/10 $32.00 www.nature.com/leu ORIGINAL ARTICLE Hsa-mir-125b-2 is highly expressed in childhood ETV6/RUNX1 (TEL/AML1) leukemias and confers survival advantage to growth inhibitory signals independent of p53 N Gefen1,2,8, V Binder1,3,8, M Zaliova4, Y Linka3, M Morrow6, A Novosel3, L Edry5, L Hertzberg1,2,7, N Shomron5, O Williams6, J Trka4, A Borkhardt3 and S Izraeli1,2 1Section of Functional Genomics and Leukemia Research, Department of Pediatric Hemato-Oncology, Sheba Medical Center, Tel-Hashomer, Israel; 2Department of Human Molecular Genetics and Biochemistry, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel; 3Department of Pediatric Hematology, Oncology and Immunology, Heinrich Heine University, Duesseldorf, Germany; 4Department of Pediatric Hematology and Oncology, Second Faculty of Medicine, Charles University and University Hospital Motol, Childhood Leukemia Investigation Prague, Prague, Czech Republic; 5Department of Cell and Developmental Biology, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel; 6Institute of Child Health, University College London, London, UK and 7Department of Physics of Complex Systems, Weizmann Institute of Science, Rehovot, Israel MicroRNAs (miRNAs) regulate the expression of multiple characterized by an intrachromosomal amplification of a small proteins in a dose-dependent manner. We hypothesized that region within the long arm of chr 21 (iAMP21) around the increased expression of miRNAs encoded on chromosome 21 4 (chr 21) contribute to the leukemogenic function of trisomy 21. RUNX1 locus. In contrast to ETV6/RUNX1 and HHD ALL, it is The levels of chr 21 miRNAs were quantified by qRT–PCR in associated with poor prognosis. -

Identification of ROBO2 As a Potential Locus Associated with Inhaled
Journal of Personalized Medicine Article Identification of ROBO2 as a Potential Locus Associated with Inhaled Corticosteroid Response in Childhood Asthma Natalia Hernandez-Pacheco 1,2,3,*,†, Mario Gorenjak 4 , Jiang Li 5 , Katja Repnik 4,6, Susanne J. Vijverberg 7,8,9, Vojko Berce 4,10 , Andrea Jorgensen 11, Leila Karimi 12 , Maximilian Schieck 13,14, Lesly-Anne Samedy-Bates 15,16, Roger Tavendale 17, Jesús Villar 3,18,19 , Somnath Mukhopadhyay 17,20, Munir Pirmohamed 21 , Katia M. C. Verhamme 12, Michael Kabesch 13, Daniel B. Hawcutt 22,23, Steve Turner 24 , Colin N. Palmer 17, Kelan G. Tantisira 5,25, Esteban G. Burchard 15,16, Anke H. Maitland-van der Zee 7,8,9 , Carlos Flores 1,3,26,27 , Uroš Potoˇcnik 4,6,*,‡ and Maria Pino-Yanes 2,3,27,‡ 1 Research Unit, Hospital Universitario N.S. de Candelaria, Universidad de La Laguna, Carretera General del Rosario 145, 38010 Santa Cruz de Tenerife, Spain; cfl[email protected] 2 Genomics and Health Group, Department of Biochemistry, Microbiology, Cell Biology and Genetics, Universidad de La Laguna, Avenida Astrofísico Francisco Sánchez s/n, Faculty of Science, Apartado 456, 38200 San Cristóbal de La Laguna, Spain; [email protected] 3 CIBER de Enfermedades Respiratorias, Instituto de Salud Carlos III, Avenida de Monforte de Lemos, 5, 28029 Madrid, Spain; [email protected] 4 Center for Human Molecular Genetics and Pharmacogenomics, Faculty of Medicine, University of Maribor, Taborska Ulica 8, 2000 Maribor, Slovenia; [email protected] (M.G.); [email protected] (K.R.); [email protected] -

Effect of the Philadelphia Chromosome on Minimal Residual Disease In
Leukemia (1997) 11, 1497–1500 1997 Stockton Press All rights reserved 0887-6924/97$12.00 Effect of the Philadelphia chromosome on minimal residual disease in acute lymphoblastic leukemia MJ Brisco1, PJ Sykes1, G Dolman1, S-H Neoh1, E Hughes1, L-M Peng2, G Tauro3, H Ekert3, I Toogood4, K Bradstock5 and AA Morley1 1Department of Haematology, Flinders Medical Centre, Bedford Park, South Australia; 2Department of Laboratory Medicine, School of Medicine, West China University of Medical Sciences, Chengdu, People’s Republic of China; 3Department of Haematology, Royal Childrens Hospital, Parkville, Victoria; 4Department of Haematology/Oncology, Womens and Childrens Hospital, North Adelaide, South Australia; and 5Department of Haematology, Westmead Hospital, Westmead, NSW, Australia The Philadelphia translocation is associated with a poor prog- number of leukemic cells remaining at the end of induction nosis in adults and children with acute lymphoblastic leukemia, provides a good approximation of the degree of drug resist- even though the majority of patients achieve remission. To test ance in vivo. the hypothesis that the translocation leads to drug resistance 6–10 in vivo, we studied 61 children and 20 adults with acute lym- Since the initial reports, a number of groups have phoblastic leukemia and used the level of minimal residual dis- developed sensitive methods to quantify minimal residual dis- ease at the end of induction as the measure of drug resistance ease (MRD) by use of the polymerase chain reaction (PCR). in vivo. In children -

REVIEW Clinical Relevance of Minimal Residual Disease Monitoring in Non
Leukemia (1999) 13, 1691–1695 1999 Stockton Press All rights reserved 0887-6924/99 $15.00 http://www.stockton-press.co.uk/leu REVIEW Clinical relevance of minimal residual disease monitoring in non-Hodgkin’s lymphomas: a critical reappraisal of molecular strategies P Corradini1, M Ladetto2, A Pileri2 and C Tarella2 1Bone Marrow Transplantation Unit, Istituto Scientifico HS Raffaele, Milan; and 2Divisione Universitaria di Ematologia–Azienda Ospedaliera S Giovanni Battista, Turin, Italy Although current treatments can induce clinical complete neoplasms. In the NHL setting, several studies have been pub- remissions in the vast majority of patients with indolent lym- lished on the prognostic significance of minimal residual dis- phoma, most of them actually relapse, because of the persist- ence of residual tumor cells which are undetectable using con- ease (MRD) detection. Most of these studies focus on indolent ventional diagnostic procedures. Polymerase chain reaction lymphomas: small lymphocytic lymphoma/chronic lympho- (PCR)-based methods are increasingly used for minimal cytic leukemia (SLL/CLL),17,18 follicular (FCL)19–21 and mantle residual disease detection (MRD), and provide useful prognos- cell lymphomas (MCL).20,22 This is mostly because these tic information. In this review, current approaches for MRD tumors, unlike more aggressive NHL histotypes, are dissemi- detection in indolent lymphomas are summarized. In addition, nated disorders with frequent microscopic or submicroscopic the prognostic aspects of molecular monitoring after transplan- tation procedures are discussed. The experience accumulated bone marrow (BM) and peripheral blood (PB) involvement, over the past decade shows that PCR analysis has a prognostic and thus they represent ideal targets for MRD evaluation with impact in several therapeutic programs including conventional PCR-based assays.23,24 and high-dose regimens. -
Supplementary Data
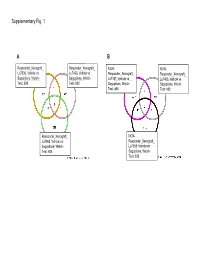
Supplementary Fig. 1 A B Responder_Xenograft_ Responder_Xenograft_ NON- NON- Lu7336, Vehicle vs Lu7466, Vehicle vs Responder_Xenograft_ Responder_Xenograft_ Sagopilone, Welch- Sagopilone, Welch- Lu7187, Vehicle vs Lu7406, Vehicle vs Test: 638 Test: 600 Sagopilone, Welch- Sagopilone, Welch- Test: 468 Test: 482 Responder_Xenograft_ NON- Lu7860, Vehicle vs Responder_Xenograft_ Sagopilone, Welch - Lu7558, Vehicle vs Test: 605 Sagopilone, Welch- Test: 333 Supplementary Fig. 2 Supplementary Fig. 3 Supplementary Figure S1. Venn diagrams comparing probe sets regulated by Sagopilone treatment (10mg/kg for 24h) between individual models (Welsh Test ellipse p-value<0.001 or 5-fold change). A Sagopilone responder models, B Sagopilone non-responder models. Supplementary Figure S2. Pathway analysis of genes regulated by Sagopilone treatment in responder xenograft models 24h after Sagopilone treatment by GeneGo Metacore; the most significant pathway map representing cell cycle/spindle assembly and chromosome separation is shown, genes upregulated by Sagopilone treatment are marked with red thermometers. Supplementary Figure S3. GeneGo Metacore pathway analysis of genes differentially expressed between Sagopilone Responder and Non-Responder models displaying –log(p-Values) of most significant pathway maps. Supplementary Tables Supplementary Table 1. Response and activity in 22 non-small-cell lung cancer (NSCLC) xenograft models after treatment with Sagopilone and other cytotoxic agents commonly used in the management of NSCLC Tumor Model Response type -

How Close Are We to Incorporating Measurable Residual Disease Into
REVIEW ARTICLE How close are we to incorporating Ferrata Storti Foundation measurable residual disease into clinical practice for acute myeloid leukemia? Nicholas J. Short and Farhad Ravandi Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, TX, USA Haematologica 2019 ABSTRACT Volume 104(8):1532-1541 ssessment of measurable residual disease, also called “minimal resid - ual disease,” in patients with acute myeloid leukemia in morpholog - Aical remission provides powerful prognostic information and comple - ments pretreatment factors such as cytogenetics and genomic alterations. Based on data that low levels of persistent or recurrent residual leukemia are consistently associated with an increased risk of relapse and worse long- term outcomes, its routine assessment has been recommended by some experts and consensus guidelines. In addition to providing important prog - nostic information, the detection of measurable residual disease may also theoretically help to determine the optimal post-remission strategy for an individual patient. However, the full therapeutic implications of measurable residual disease are uncertain and thus controversy exists as to whether it should be routinely incorporated into clinical practice. While some evidence supports the use of allogeneic stem cell transplantation or hypomethylating agents for some subgroups of patients in morphological remission but with detectable residual leukemia, the appropriate use of this information in mak - ing clinical decisions remains largely speculative at present. To resolve this pressing clinical issue, several ongoing studies are evaluating measurable Correspondence: residual disease-directed treatments in acute myeloid leukemia and may FARHAD RAVANDI lead to new, effective strategies for patients in these circumstances. This [email protected] review examines the common technologies used in clinical practice and in the research setting to detect residual leukemia, the major clinical studies Received: February 8, 2019. -

Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva
UCSF UC San Francisco Previously Published Works Title Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva. Permalink https://escholarship.org/uc/item/95h5g8mq Journal Cell reports, 33(7) ISSN 2211-1247 Authors Saitou, Marie Gaylord, Eliza A Xu, Erica et al. Publication Date 2020-11-01 DOI 10.1016/j.celrep.2020.108402 Peer reviewed eScholarship.org Powered by the California Digital Library University of California HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Cell Rep Manuscript Author . Author manuscript; Manuscript Author available in PMC 2020 November 30. Published in final edited form as: Cell Rep. 2020 November 17; 33(7): 108402. doi:10.1016/j.celrep.2020.108402. Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva Marie Saitou1,2,3, Eliza A. Gaylord4, Erica Xu1,7, Alison J. May4, Lubov Neznanova5, Sara Nathan4, Anissa Grawe4, Jolie Chang6, William Ryan6, Stefan Ruhl5,*, Sarah M. Knox4,*, Omer Gokcumen1,8,* 1Department of Biological Sciences, University at Buffalo, The State University of New York, Buffalo, NY, U.S.A 2Section of Genetic Medicine, Department of Medicine, University of Chicago, Chicago, IL, U.S.A 3Faculty of Biosciences, Norwegian University of Life Sciences, Ås, Viken, Norway 4Program in Craniofacial Biology, Department of Cell and Tissue Biology, School of Dentistry, University of California, San Francisco, CA, U.S.A 5Department of Oral Biology, School of Dental Medicine, University at Buffalo, The State University of New York, Buffalo, NY, U.S.A 6Department of Otolaryngology, School of Medicine, University of California, San Francisco, CA, U.S.A 7Present address: Weill-Cornell Medical College, Physiology and Biophysics Department 8Lead Contact SUMMARY Salivary proteins are essential for maintaining health in the oral cavity and proximal digestive tract, and they serve as potential diagnostic markers for monitoring human health and disease. -

Cancer and the Immune System an Overview of Recent Publications Featuring Illumina® Technology 2 Cancer and the Immune System TABLE of CONTENTS
Cancer and the Immune System An Overview of Recent Publications Featuring Illumina® Technology 2 Cancer and the Immune System TABLE OF CONTENTS 04 Introduction 05 Dendritic cells 07 T-Cell Repertoire 09 Intratumoral T-Cells 11 Single Cells and TCR Sequencing 14 Cancer antigens 18 Cancer Immunoediting 20 Tumor Microenvironment 22 Cancer Immunotherapy 25 Hematological Malignancies 28 Tracking Malignant Lymphocytes 30 Bibliography Cancer and the Immune System 3 INTRODUCTION Advances in high-throughput sequencing have dramatically improved our knowledge of the cancer genome and the intracellular mechanisms involved in tumor progression and response to treatment. While the primary focus to date has been on the cancer cell, this technology can also be used to understand the interaction of the tumor cells and the cells in the surrounding tumor microenvironment. The tumor microenvironment is defined as the cellular environment in which the tumor exists. This includes surrounding blood vessels, immune cells, fibroblasts, other cells, signaling molecules, and the extracellular matrix. Expression analysis of the RNA levels can be used to determine the activation of pathways in the tumor microenvironment. Since common signaling pathways are involved in manifestation of several hallmarks of cancer, including cancer cell proliferation, survival, invasion, metastasis, and immunosuppression, targeting these shared signaling pathways in combination with immunotherapy may be a promising strategy for cancer treatment1. It is important to note that RNA-seq has the potential to track the activation of individual clones, which could ultimately lead to personalized treatment2,3. The human adaptive immune system provides protection against an enormous variety of pathogens and well as tumors. -

Minimal Residual Disease Detection in Mantle Cell Lymphoma
Original Article Minimal residual disease detection in mantle cell lymphoma: methods and significance of four-color flow cytometry compared to consensus IGH-polymerase chain reaction at initial staging and for follow-up examinations Sebastian Böttcher,1 Matthias Ritgen,1 Sebastian Buske,1 Stefan Gesk,2 Wolfram Klapper,3 Eva Hoster,4 Wolfgang Hiddemann,4 Michael Unterhalt,4 Martin Dreyling,4 Reiner Siebert,2 Michael Kneba,1 and Christiane Pott1 on behalf of the EU MCL MRD Group 1University of Schleswig-Holstein, Campus Kiel, 2nd Department of Medicine, Kiel, Germany; 2University of Schleswig-Holstein, Campus Kiel, Institute of Human Genetics, Kiel, Germany; 3Department of Haematopathology and Lymph Node Registry Kiel, University of Schleswig-Holstein, Campus Kiel, Germany and 4Department of Internal Medicine III, University of Munich, Hospital Grosshadern, Munich, Germany Citation: Böttcher S, Ritgen M, Buske S, Gesk S, Klapper W, Hoster E, Hiddemann W, Unterhalt M, Dreyling M, Siebert R, Kneba M and Pott C on behalf of the EU MCL MRD Group. Minimal residual disease detection in mantle cell lymphoma: methods and significance of four-color flow cytometry compared to consensus IGH-polymerase chain reaction at initial staging and for follow-up examinations. Haematologica 2008 Apr; 93(4):XXX-XXX. doi: 10.3324/haematol.11267 Treatment protocols as published by the BIOMED-2 Concerted Action.3 FAM- labeled PCR products were size separated on a high-resolu- Untreated patients with Ann Arbor stage II to IV MCL tion polyacrylamide gel and laser-induced fluorescence ana- were eligible for inclusion in the trials. Computed tomogra- lyzed using an ABI 310 genetic analyzer (Applied phy (CT) examinations of neck, chest, abdomen, and pelvis Biosystems, ABI, Darmstadt, Germany) as described previ- as well as bone marrow biopsies for cytology and histology ously (GeneScanning).4 In case of a polyclonal signal after (in general assessed by local pathologists) were mandatory FR1-IGH PCR, FR2- and FR3-IGH primer sets were used in for initial staging. -

HDAC3: Taking the SMRT-N-Correct Road to Repression
Oncogene (2007) 26, 5439–5449 & 2007 Nature Publishing Group All rights reserved 0950-9232/07 $30.00 www.nature.com/onc REVIEW HDAC3: taking the SMRT-N-CoRrect road to repression P Karagianni and J Wong1 Department of Molecular and Cellular Biology, Baylor College of Medicine, One Baylor Plaza, Houston, TX, USA Known histone deacetylases (HDACs) are divided into repression when targeted to promoters, as well as different classes, and HDAC3 belongs to Class I. Through physical association with the DNA-binding factor forming multiprotein complexes with the corepressors YY1 (Yang et al., 1997; Dangond et al., 1998; Emiliani SMRT and N-CoR, HDAC3 regulates the transcription et al., 1998). Together, these findings suggested that this of a plethora of genes. A growing list of nonhistone ubiquitously expressed protein could be involved in the substrates extends the role of HDAC3 beyond transcrip- regulation of mammalian gene expression. On the other tional repression. Here, we review data on the composi- hand, HDAC3 contains an intriguingly variable C tion, regulation and mechanism of action of the SMRT/ terminus, with no apparent similarity with other N-CoR-HDAC3 complexes and provide several examples HDACs. This observation led to the hypothesis that of nontranscriptional functions, to illustrate the wide HDAC3 may have some unique properties and may variety of physiological processes affected by this deacety- not be completely redundant with the other HDACs lase. Furthermore, we discuss the implication of HDAC3 (Yang et al., 1997). This is also suggested by the in cancer, focusing on leukemia. We conclude with some differential localization of HDAC3, which, unlike the thoughts about the potential therapeutic efficacies of predominantly nuclear HDACs 1 and 2, can be found in HDAC3 activity modulation.