Epidemiological Trends of Malaria in Eastern Shan State, Myanmar 2000-2016
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Weekly Security Review (27 August – 2 September 2020)
Commercial-In-Confidence Weekly Security Review (27 August – 2 September 2020) Weekly Security Review Safety and Security Highlights for Clients Operating in Myanmar 27 August – 2 September 2020 Page 1 of 27 Commercial-In-Confidence Weekly Security Review (27 August – 2 September 2020) EXECUTIVE SUMMARY ............................................................................................................................. 3 Internal Conflict ....................................................................................................................................... 4 Nationwide .......................................................................................................................................... 4 Rakhine State ....................................................................................................................................... 4 Shan State ............................................................................................................................................ 5 Myanmar and the World ......................................................................................................................... 8 Election Watch ........................................................................................................................................ 8 Social and Political Stability ................................................................................................................... 11 Transportation ...................................................................................................................................... -

National Transport Master Plan
Ministry of Transport The Republic of the Union of Myanmar The Survey Program for the National Transport Development Plan in the Republic of the Union of Myanmar Final Report September 2014 JAPAN INTERNATIONAL COOPERATION AGENCY Oriental Consultants Co., Ltd. International Development Center of Japan EI ALMEC Corporation JR 14-192 Ministry of Transport The Republic of the Union of Myanmar The Survey Program for the National Transport Development Plan in the Republic of the Union of Myanmar Final Report September 2014 JAPAN INTERNATIONAL COOPERATION AGENCY Oriental Consultants Co., Ltd. International Development Center of Japan ALMEC Corporation Exchange rate used in this Report USD 1.00 = JPY 99.2 USD 1.00 = MMK 970.9 MMK 1.00 = JPY 0.102 (As of October, 2013) Project Location Map The Survey Program for the National Transport Development Plan in the Republic of the Union of Myanmar A grand design for the transport sector at the dawn of new and modern era of transport development in Myanmar Final Report TABLE OF CONTENTS Page Chapter 1. Introduction 1.1 MYT-Plan Goals and Objective ..................................................................................... 1 - 1 1.2 Structure of the Master Plan ....................................................................................... 1 - 2 1.3 Structure of the Report ................................................................................................ 1 - 3 Chapter 2. Socio-economic and Financial Frameworks 2.1 Demographic Framework ........................................................................................... -
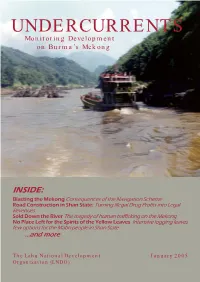
UNDERCURRENTS Monitoring Development on Burma’S Mekong
UNDERCURRENTS Monitoring Development on Burma’s Mekong INSIDE: Blasting the Mekong Consequences of the Navigation Scheme Road Construction in Shan State: Turning Illegal Drug Profits into Legal Revenues Sold Down the River The tragedy of human trafficking on the Mekong No Place Left for the Spirits of the Yellow Leaves Intensive logging leaves few options for the Mabri people in Shan State ...and more The Lahu National Development January 2005 Organization (LNDO) The Mekong/ Lancang The Mekong River is Southeast Asia’s longest, stretching from its source in Tibet to the delta of Vietnam. Millions of people depend on it for agriculture and fishing, and accordingly it holds a special cultural significance. For 234 kilometers, the Mekong forms the border between Burma’s Shan State and Luang Nam Tha and Bokeo provinces of Laos. This stretch includes the infamous “Golden Triangle”, or where Burma, Laos and Thailand meet, which has been known for illicit drug production. Over 22,000 primarily indigenous peoples live in the mountainous region of this isolated stretch of the river in Burma. The main ethnic groups are Akha, Shan, Lahu, Sam Tao (Loi La), Chinese, and En. The Mekong River has a special significance for the Lahu people. Like the Chinese, we call it the Lancang, and according to legends, the first Lahu people came from the river’s source. Traditional songs and sayings are filled with references to the river. True love is described as stretching form the source of the Mekong to the sea. The beauty of a woman is likened to the glittering scales of a fish in the Mekong. -

IDP 2011 Eng Cover Master
Map 7 : Southern and Central Shan State Hsipaw Mongmao INDIA Ta ng ya n CHINA Mongyai MYANMAR (BURMA) LAOS M Y A N M A R / B U R M A THAILAND Pangsang Kehsi Mong Hsu Matman Salween Mongyang S H A N S T A T E Mongket COAL MINE Mongla Mong Kung Pang Mong Ping Kunhing Kengtung Yatsauk Laikha Loilem Namzarng Monghpyak Mong Kok COAL MINE Taunggyi KENG TAWNG DAM COAL MINE Nam Pawn Mong Hsat Mongnai TASANG Tachilek Teng DAM Langkher Mongpan Mongton Mawkmai Hsihseng en Salwe Pekon T H A I L A N D Loikaw Kilometers Shadaw Demawso Wieng Hang Ban Mai 01020 K A Y A H S T A T E Nai Soi Tatmadaw Regional Command Refugee Camp Development Projects Associated with Human Rights Abuses Tatmadaw Military OPS Command International Boundary Logging Tatmadaw Battalion Headquarters State/Region Boundary Dam BGF/Militia HQ Rivers Mine Tatmadaw Outpost Roads Railroad Construction BGF/Militia Outpost Renewed Ceasefire Area (UWSA, NDAA) Road Construction Displaced Village, 2011 Resumed Armed Resistance (SSA-N) IDP Camp Protracted Armed Resistance (SSA-S, PNLO) THAILAND BURMA BORDER CONSORTIUM 43 Map 12 : Tenasserim / Tanintharyi Region INDIA T H A I L A N D CHINA MYANMAR Yeb yu (BURMA) LAOS Dawei Kanchanaburi Longlon THAILAND Thayetchaung Bangkok Ban Chaung Tham Hin T A N I N T H A R Y I R E G I O N Gulf Taninth of Palaw a Thailand ryi Mergui Andaman Sea Tanintharyi Mawtaung Bokpyin Kilometers 0 50 100 Kawthaung Development Projects Associated Tatmadaw Regional Command Refugee Camp with Human Rights Abuses Tatmadaw Military OPS Command International Boundary Gas -

THE POLITICAL ECONOMY of OPIUM REDUCTION in BURMA: LOCAL PERSPECTIVES from the WA REGION Mr. Sai Lone a Thesis Submitted in Part
THE POLITICAL ECONOMY OF OPIUM REDUCTION IN BURMA: LOCAL PERSPECTIVES FROM THE WA REGION Mr. Sai Lone A Thesis Submitted in Partial Fulfillment of the Requirements for the Degree of Master of Arts Program in International Development Studies Faculty of Political Science Chulalongkorn University Academic Year 2008 Copyright of Chulalongkorn University เศรษฐศาสตรการเมืองของการปราบฝนในประเทศพมา: มุมมองระดับทองถิ่นในเขตวา นายไซ โลน วิทยานิพนธน ี้เปนสวนหนึ่งของการศึกษาตามหลกสั ูตรปริญญาศิลปศาสตรมหาบัณฑิต สาขาวิชาการพัฒนาระหวางประเทศ คณะรัฐศาสตร จุฬาลงกรณมหาวิทยาลัย ปการศึกษา 2551 ลิขสิทธิ์ของจุฬาลงกรณมหาวิทยาลัย Thesis title: THE POLITICAL ECONOMY OF OPIUM REDUCTION IN BURMA: LOCAL PERSPECTIVES FROM THE WA REGION By: Mr. Sai Lone Field of Study: International Development Studies Thesis Principal advisor: Niti Pawakapan, Ph. D. Accepted by the Faculty of Political Science, Chulalongkorn University in Partial Fulfillment of the Requirements for the Master’s Degree ___________________________ Dean of the Faculty of Political Science (Professor Charas Suwanmala, Ph.D.) THESIS COMMITTEE ___________________________ Chairperson (Professor Supang Chantavanich, Ph.D.) ___________________________ Thesis Principal Advisor (Niti Pawakapan, Ph.D.) ___________________________ External Examiner (Decha Tangseefa, Ph.D.) นายไซ โลน: เศรษฐศาสตรการเมืองของการปราบฝนในประเทศพมา: มุมมองระดับ ทองถิ่นในเขตวา (THE POLITICAL ECONOMY OF OPIUM REDUCTION IN BURMA: LOCAL PERSPECTIVES FROM THE WA REGION) อ. ทปรี่ ึกษา: ดร.นิติ ภวัครพันธุ. 133 หนา. งานวิจัยชิ้นนี้เนนศึกษาผลกระทบดานเศรษฐกิจสังคมของโครงการพัฒนาชนบทที่ดําเนินงานโดยองคกร -

Displacement and Poverty in South East Burma/Myanmar
It remains to be seen how quickly and effectively the new DISPLACEMENT government will be able to tackle poverty, but there has not yet been any relaxation of restrictions on humanitarian AND POVERTY access into conflict-affected areas. In this context, the vast majority of foreign aid continues to be channelled into areas IN SOUTH EAST not affected by armed conflict such as the Irrawaddy/ Ayeyarwady Delta, the Dry Zone and Rakhine State. While responding to demonstrated needs, such engagement is BURMA/MYANMAR building trust with authorities and supporting advocacy for increased humanitarian space throughout the country. Until this confidence building process translates into access, 2011 cross-border aid will continue to be vital to ensure that the needs of civilians who are affected by conflict in the South East and cannot be reached from Yangon are not further marginalised. overty alleviation has been recognised by the new A new government in Burma/Myanmar offers the possibility The opportunity for conflict transformation will similarly government as a strategic priority for human of national reconciliation and reform after decades of conflict. require greater coherence between humanitarian, political, Thailand Burma Border Consortium (TBBC) development. While official figures estimate that a Every opportunity to resolve grievances, alleviate chronic development and human rights actors. Diplomatic www.tbbc.org quarter of the nation live in poverty, this survey poverty and restore justice must be seized, as there remain engagement with the Government in Naypidaw and the non Download the full report from Psuggests that almost two thirds of households in rural areas many obstacles to breaking the cycle of violence and abuse. -

SSA-S Government 11-Point Peace Agreement
SSA-S Government 11-point peace agreement 16 January 2012 RCSS/SSA and Union-Level Peace-making group signed an eleven-point peace agreement in Taunggyi, the capital of Shan State, on 16 Jan 2012. Unofficial Translation ........................................................................................................................................ 1. To allow RCSS/SSA headquarters in Homain sub-township and Mong Hta sub- township. 2. The government troops to negotiate and arrange in order that RCSS/SSA troops and their families be resettled in the locations mentioned in No. 1 3. RCSS/SSA will appoint village heads in the region; for township level administration the village heads will cooperate with government officials 4. Government soldiers in Homain sub-township and Mong Hta sub-township to give help to RCSS/SSA; Both sides will discuss and negotiate to arrange for the security of RCSS/SSA leaders 5. Government troops and RCSS/SSA to negotiate to designate areas where they can enter in border areas 6. Each side agreed to inform the other side in advance if one side wants to enter the other’s control area with weapons 7. To open liaison offices between the government and SSA-S in Taunggyi, Kholam, Kengtung, Mong Hsat and Tachileik and trading offices in Muse and Nanhkan 8. Government ministers to arrange for SSA-S members to run businesses and companies in accord with existing policies, by providing helps and supporting required technology 9. To cooperate with the union government for regional development 10. To cooperate with the government in making plan for battling drug trafficking 11. The government and RCSS/SSA agreed in principle to the points discussed on January 16, 2012. -
Geology & Mineral Resources of Myanmar
Geology & Mineral Resources of Myanmar KYAW KYAW OHN Assistant Director (Geologist) DEPARTMENT OF GEOLOGICAL SURVEY AND MINERAL EXPLORATION MINISTRY OF MINES 1 Introduction Organization Morpho-Tectonic Geology Mineral Occurrence Investment Cooperation Conclusion Belts of Setting of & Mining Activities Opportunities with Myanmar Myanmar in Myanmar International Myanmar is endowed with resources of arable land, natural gas, mineral deposits, fisheries, forestry and manpower. 2 Introduction Organization Morpho-Tectonic Geology Mineral Occurrence Investment Cooperation Conclusion Belts of Setting of & Mining Activities Opportunities with Myanmar Myanmar in Myanmar International Area : 678528 sq.km Coast Line : 2100 km Border : 4000 km NS Extend : 2200 km EW Extend : 950 km Population : >51millions(est:) Region : 7 State: : 7 Location : 10º N to 28º 30' 92º 30' E to 101º30' 3 Introduction Organization Morpho-Tectonic Geology Mineral Occurrence Investment Cooperation Conclusion Belts of Setting of & Mining Activities Opportunities with Myanmar Myanmar in Myanmar International Union Minister Deputy Minister No.(1) No.(2) Myanmar Myanmar Department of Geological Department Mining Mining Gems Pearl Survey &Mineral of Enterprise Enterprise Enterprise Enterprise Exploration Mines Lead Coal Gold Gems, Pearl Geological Mineral Zinc Lime stone Tin Jade Breeding Survey Policy Silver Industrial Tungsten & Cultivating Mineral formulation, Copper Minerals Rare Earth Jewelry Exploration Regulation Iron Manganese Titanium Laboratory measures Nickel Decorative -

Gazetteer of Upper Burma and the Shan States. in Five
GAZETTEER OF UPPER BURMA AND THE SHAN STATES. IN FIVE VOLUMES. COMPILED FROM OFFICIAL PAPERS BY J. GEORGE SCOTT. BARRISTER-AT-LAW, C.I.E., M.R.A.S., F.R.G.S., ASSISTED BY J. P. HARDIMAN, I.C.S. PART II.--VOL. III. RANGOON: PRINTED BY THE SUPERINTENDENT, GOVERNMENT PRINTING, BURMA. 1901. [PART II, VOLS. I, II & III,--PRICE: Rs. 12-0-0=18s.] CONTENTS. VOLUME III. Page. Page. Page. Ralang 1 Sagaing 36 Sa-le-ywe 83 Ralôn or Ralawn ib -- 64 Sa-li ib. Rapum ib -- ib. Sa-lim ib. Ratanapura ib -- 65 Sa-lin ib. Rawa ib. Saga Tingsa 76 -- 84 Rawkwa ib. Sagônwa or Sagong ib. Salin ib. Rawtu or Maika ib. Sa-gu ib. Sa-lin chaung 86 Rawva 2 -- ib. Sa-lin-daung 89 Rawvan ib. Sagun ib -- ib. Raw-ywa ib. Sa-gwe ib. Sa-lin-gan ib. Reshen ib. Sa-gyan ib. Sa-lin-ga-thu ib. Rimpi ib. Sa-gyet ib. Sa-lin-gôn ib. Rimpe ib. Sagyilain or Limkai 77 Sa-lin-gyi ib. Rosshi or Warrshi 3 Sa-gyin ib -- 90 Ruby Mines ib. Sa-gyin North ib. Sallavati ib. Ruibu 32 Sa-gyin South ib. Sa-lun ib. Rumklao ib. a-gyin San-baing ib. Salween ib. Rumshe ib. Sa-gyin-wa ib. Sama 103 Rutong ib. Sa-gyu ib. Sama or Suma ib. Sai Lein ib. Sa-me-gan-gôn ib. Sa-ba-dwin ib. Saileng 78 Sa-meik ib. Sa-ba-hmyaw 33 Saing-byin North ib. Sa-meik-kôn ib. Sa-ban ib. -

Myanmar Opium Survey 2019 Cultivation, Production and Implications
COVER MYANMAR OPIUM SURVEY 2019 CULTIVATION, PRODUCTION AND IMPLICATIONS DRAFT 2020-01-27 JANUARY 2020 In Southeast Asia, UNODC supports Member States to develop and implement evidence- based rule of law, drug control and related criminal justice responses through the Regional Programme 2014-2021 and aligned country programmes including the Myanmar Country Programme 2014-2021. This study is connected to the Mekong MOU on Drug Control which UNODC actively supports through the Regional Programme, including the commitment to develop data and evidence as the basis for countries of the Mekong region to respond to challenges of drug production, trafficking and use. UNODC’s Research and Trend Analysis Branch promotes and supports the development and implementation of surveys globally, including through its Illicit Crop Monitoring Programme (ICMP). The implementation of Myanmar opium survey was made possible thanks to the financial support of the Governments of Japan and the United States of America. UNODC Regional Office for Southeast Asia and the Pacific Telephone: +6622882100 Fax: +6622812129 Email: unodc‐[email protected] Website: www.unodc.org/southeastasiaandpacific Twitter: @UNODC_SEAP The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of UNODC concerning the legal status of any country, territory or city, or its authorities, or concerning the delimitation of its frontiers or boundaries. Contents Acknowledgements ........................................................................................................................... -

Myanmar Languages | Ethnologue
7/24/2016 Myanmar Languages | Ethnologue Myanmar LANGUAGES Akeu [aeu] Shan State, Kengtung and Mongla townships. 1,000 in Myanmar (2004 E. Johnson). Status: 5 (Developing). Alternate Names: Akheu, Aki, Akui. Classi囕cation: Sino-Tibetan, Tibeto-Burman, Ngwi-Burmese, Ngwi, Southern. Comments: Non-indigenous. More Information Akha [ahk] Shan State, east Kengtung district. 200,000 in Myanmar (Bradley 2007a). Total users in all countries: 563,960. Status: 3 (Wider communication). Alternate Names: Ahka, Aini, Aka, Ak’a, Ekaw, Ikaw, Ikor, Kaw, Kha Ko, Khako, Khao Kha Ko, Ko, Yani. Dialects: Much dialectal variation; some do not understand each other. Classi囕cation: Sino-Tibetan, Tibeto-Burman, Ngwi-Burmese, Ngwi, Southern. More Information Anal [anm] Sagaing: Tamu town, 10 households. 50 in Myanmar (2010). Status: 6b (Threatened). Alternate Names: Namfau. Classi囕cation: Sino-Tibetan, Tibeto-Burman, Sal, Kuki-Chin-Naga, Kuki-Chin, Northern. Comments: Non- indigenous. Christian. More Information Anong [nun] Northern Kachin State, mainly Kawnglangphu township. 400 in Myanmar (2000 D. Bradley), decreasing. Ethnic population: 10,000 (Bradley 2007b). Total users in all countries: 450. Status: 7 (Shifting). Alternate Names: Anoong, Anu, Anung, Fuchve, Fuch’ye, Khingpang, Kwingsang, Kwinp’ang, Naw, Nawpha, Nu. Dialects: Slightly di㨽erent dialects of Anong spoken in China and Myanmar, although no reported diഡculty communicating with each other. Low inherent intelligibility with the Matwang variety of Rawang [raw]. Lexical similarity: 87%–89% with Anong in Myanmar and Anong in China, 73%–76% with T’rung [duu], 77%–83% with Matwang variety of Rawang [raw]. Classi囕cation: Sino-Tibetan, Tibeto-Burman, Central Tibeto-Burman, Nungish. Comments: Di㨽erent from Nung (Tai family) of Viet Nam, Laos, and China, and from Chinese Nung (Cantonese) of Viet Nam. -

BURMA/ K-N 2 5-7 March 2021 MYANMAR Chiang Mai University STUDIES Thailand Myanmar/Burma in the Changing Southeast Asian Context
3rd International Conference on VOLUME BURMA/ K-N 2 5-7 March 2021 MYANMAR Chiang Mai University STUDIES Thailand Myanmar/Burma in the Changing Southeast Asian Context PROCEEDINGS 3RD INTERNATIONAL CONFERENCE ON BURMA/MYANMAR STUDIES: MYANMAR/BURMA IN THE CHANGING SOUTHEAST ASIAN CONTEXT 5-7 MARCH 2021, CHIANG MAI UNIVERSITY, THAILAND 3RD INTERNATIONAL CONFERENCE ON BURMA/MYANMAR STUDIES: MYANMAR/BURMA IN THE CHANGING SOUTHEAST ASIAN CONTEXT PROCEEDINGS Volume K-N 05 -07 March 2021, Chiang Mai University, Thailand 3RD INTERNATIONAL CONFERENCE ON BURMA/MYANMAR STUDIES: MYANMAR/BURMA IN THE CHANGING SOUTHEAST ASIAN CONTEXT 5-7 MARCH 2021, CHIANG MAI UNIVERSITY, THAILAND March 2021 ICBMS III Conference Secretariat Regional Center for Social Science and Sustainable Development (RCSD) Faculty of Social Sciences, Chiang Mai University, Chiang Mai, Thailand Email: [email protected], [email protected]; Website: http://burmaconference.com 3RD INTERNATIONAL CONFERENCE ON BURMA/MYANMAR STUDIES: MYANMAR/BURMA IN THE CHANGING SOUTHEAST ASIAN CONTEXT 5-7 MARCH 2021, CHIANG MAI UNIVERSITY, THAILAND Table of Contents LOCAL KNOWLEDGE ABOUT WATER AND SANITATION PATTERNS IN SHAN KALAY KYAUNG VILLAGE Khin Khin Nyein & Myint Myint Khaing ........................................................................................................... 259 MIGRATION ISSUE ON THE URBAN RESILIENCE OF YANGON AREA (CASE STUDY ON THE MOBILE/MIGRANT SETTLEMENT) Khin Mar Yee, Mu Mu Than, Wah Wah Soe, Min Min Aye Than & Hnin Khaine Aye .......................................