Sexual Orientation and Trans Sexuality 101
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Black Boi, Boss Bitch
Black Boi, Boss Bitch Lauryn Hill 18 Jan 1995 - 26 Sep 1998 BLACK QUEER LOOKS Y todo comenzo bailando.... 27 Oct 1998 “Y todo comenzo bailando”...The earliest memories I can recall of my existence are festive. 20 Pound Pots of pernil & pigfeet. Pasteles, Gandulez, Guinea, Pollo Guisado. Habichuelas. 5 different types of beans & 5 different dishes on one plate. Even if only 4 niggas pulled up to the crib, abuela was always cooking for 40. The image of her red lipstick stain on hefty glasses of Budweiser that once contained Goya olives is forever etched in my mind. This was that poor boricua family that stored rice & beans in “I Can’t Believe it’s Not Butter” containers.The kind of family that blasted Jerry Rivera’s & Frankie Ruiz voices over dollar-store speakers. The kind that prized Marc Anthony, Hector LaVoe, El Gran Combo, La India, Tito Rojas. Victor Manuelle. Salsa Legends that put abuela's feet to work. My cousin Nina & her wife Iris who sparked their Ls in the bathroom, waving around floor length box braids, and bomb ass butch-queen aesthetics. “Pero nino, you hoppin on the cyph?. Uncle Negro or “Black”as we called him for his rich dark-skin, stay trying to wife my mom’s friends. 7:11 pm. 7 pounds 8 oz. October 27th. Maybe it was the lucky 7. Maybe it was fated for them to welcome another, intensely-loving Scorpio into their home. Or maybe it was just another blissful evening in the barrio. Where Bottles of Henny would be popped, and cousins & aunts & uncles you didn’t even know you had would reappear. -

The Oxford Democrat : Vol. 70. No.52
The Oxford Democrat. 1903. NUMBER 52. VOLUME 70. SOUTH PARIS, MAINE, TUESDAY, DECEMBER 29, KH tiMh'.l lo; ili l 'y. oners, but Beverley soon suspected tl tt rutiler item, who was coining out 01 never fails. But he'll tell Clark to eta.v JUNKS, Fruit Marketing and Storage. *«W>4^3*4HfcHêHîMlHWHfr^ Furii «worth was on his guard in a C. THE a "tralllc In hah," ae the terrible bu-tl- u cabin nut far away, beard and knew where he is, and Vigo can do no more." ^ AMONG FARMERS. Some of the most and twin!;iing. lie set his jaw and uttered preening impor- ness had been named, was going on. the voice. What effect Helm's hold and appar- & Machinist, in- a< I!· htnh.· Smith tant relating to the fri\it f nil ugly oath: then qiii-k MA1NK. questions miH"î Savages came In from far away with Ho. lio. little cried artless talk h:id upon Hamilton's SOUTH PARIS, are those that out of the y4"i«P my lady!" ently at the with "SFLKD THIS PLOW." dustry grow he struck siucwlse pistol of general machinery, steam en in horticulture to scalps yet scarcely dry dangling at Adrien ne's captor in a breezy, jocund mind Is not recorded, hut the meager Manufacturer anil tools., .present tendency pro- his blade. It was a move which might mill work, spool machinery their belis. It made the Vir- "You wouldn't run over u facts at command show that ,'lties, drille made and duce each fruit in that section where it #| young tone. -
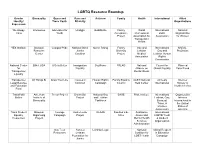
Lgbt Resource Roundup
LGBTQ Resource Roundup Gender Bisexuality Queer and Race and Activism Family Health International Allied Identity/ Trans Youth Ethnicity Organizations Expression We Happy Interweave Advocates for Unid@s GetEQUAL Family World International National Trans Youth Acceptance Professional LGBT Organization Project Association for Association for Women Transgender Health YES Institute Bisexual Campus Pride National Black Queer Rising Family Gay and International NARAL- Resource Justice Diversity Lesbian Gay and ProChoice Center Coalition Project Medical Lesbian Human Association Rights Commission National Center BiNet USA It Gets Better Immigration SoulForce PFLAG National Council for Planned for Equality Alliance on Global Equality Parenthood Transgender Mental Illness Equality Transgender All Things Bi Draw Your Line Causes in Human Rights Family Equality GLBT National Amnesty Intersex Legal Defense Common Campaign Council Help Center International Society of and Education North America Fund TransFaith American Trevor Project Brown Boi National Gay SAGE Pride Institute International Organization Online Institute of Project and Lesbian Lesbian, Gay, Intersex Bisexuality Taskforce Bisexual, International in Trans, & the United Intersex States of Association America Trans Student Bisexual Courage Audre Lorde GLAAD Families Like Substance International Equality Organizing Campaign Project Mine Abuse and LGBTQ Youth Resources Project Mental Health & Student Services Organization Administration Gay Teen Astraea Lambda Legal National Global Respect -

Genders & Sexualities Terms
GENDERS & SEXUALITIES TERMS All terms should be evaluated by your local community to determine what best fits. As with all language, the communities that utilize these and other words may have different meanings and reasons for using different terminology within different groups. Agender: a person who does not identify with a gender identity or gender expression; some agender-identifying people consider themselves gender neutral, genderless, and/or non- binary, while some consider “agender” to be their gender identity. Ally/Accomplice: a person who recognizes their privilege and is actively engaged in a community of resistance to dismantle the systems of oppression. They do not show up to “help” or participate as a way to make themselves feel less guilty about privilege but are able to lean into discomfort and have hard conversations about being held accountable and the ways they must use their privilege and/or social capital for the true liberation of oppressed communities. Androgynous: a person who expresses or presents merged socially-defined masculine and feminine characteristics, or mainly neutral characteristics. Asexual: having a lack of (or low level of) sexual attraction to others and/or a lack of interest or desire for sex or sexual partners. Asexuality exists on a spectrum from people who experience no sexual attraction nor have any desire for sex, to those who experience low levels of sexual attraction and only after significant amounts of time. Many of these different places on the spectrum have their own identity labels. Another term used within the asexual community is “ace,” meaning someone who is asexual. -

Beyond the Binary: Gender Identity and Mental Health Among Transgender and Gender Non-Conforming Adults
City University of New York (CUNY) CUNY Academic Works All Dissertations, Theses, and Capstone Projects Dissertations, Theses, and Capstone Projects 9-2018 Beyond the Binary: Gender Identity and Mental Health Among Transgender and Gender Non-Conforming Adults Chassitty N. Fiani The Graduate Center, City University of New York How does access to this work benefit ou?y Let us know! More information about this work at: https://academicworks.cuny.edu/gc_etds/2815 Discover additional works at: https://academicworks.cuny.edu This work is made publicly available by the City University of New York (CUNY). Contact: [email protected] BEYOND THE BINARY: GENDER IDENTITY AND MENTAL HEALTH AMONG TRANSGENDER AND GENDER NON-CONFORMING ADULTS by CHASSITTY N. FIANI A dissertation submitted to the Graduate Faculty in Psychology in partial fulfillment of the requirements for the degree of Doctor of Philosophy, The City University of New York 2018 © 2018 CHASSITTY N. FIANI All Rights Reserved ii Beyond the Binary: Gender Identity and Mental Health among Transgender and Gender Non- Conforming Adults by Chassitty N. Fiani This manuscript has been read and accepted for the Graduate Faculty in Psychology in satisfaction of the dissertation requirement for the degree of Doctor of Philosophy. __________________ __________________________________ Date Kevin L. Nadal Chair of Examining Committee __________________ __________________________________ Date Richard Bodnar Executive Officer Supervisory Committee: Dr. Chitra Raghavan Dr. Brett Stoudt Dr. Michelle Fine Dr. David Rivera THE CITY UNIVERSITY OF NEW YORK iii ABSTRACT Beyond the Binary: Gender Identity and Mental Health among Transgender and Gender Non- Conforming Adults by Chassitty N. Fiani Advisor: Kevin L. -

Queer Feminine Disidentificatory Orientations: Occupying Liminal Spaces of Queer Fem(Me)Inine (Un)Belonging
1 Queer Feminine Disidentificatory Orientations: Occupying Liminal Spaces of Queer Fem(me)inine (Un)Belonging Alexandra Athelstan-Price Submitted in accordance with the requirements for the degree of Doctor of Philosophy The University of Leeds School of Sociology and Social Policy September 2014 2 The candidate confirms that the work submitted is her own and that appropriate credit has been given where reference has been made to the work of others. This copy has been supplied on the understanding that it is copyright material and that no quotation from the thesis may be published without proper acknowledgement © 2014 The University of Leeds and Alexandra Athelstan-Price. The right of Alexandra Athelstan-Price to be identified as Author of this work has been asserted by her in accordance with the Copyright, Designs and Patents Act 1988. 3 'If I didn't define myself for myself, I would be crunched into other people's fantasies for me and eaten alive.' - Audre Lorde 4 Table of Contents Acknowledgements Abstract Chapter 1: Introduction i) Introduction ii) Theoretical Framework: Disidentificatory Orientations iii) Literature Review: Femme and Queer Femininities iv) Why Queer Femininities Matter! v) Conclusion Chapter 2: Methodology: Towards a Collaborative Femme Ethnography i) Introduction ii) Summary of Methods iii) Queer Fem(me)inist Methodologies & Ethnography iv) Reflexivity v) Recruiting Participants vi) Questionnaire vii) Sampling viii) Visual Methods ix) Qualitative Interviews x) Discourse Analysis xi) Ethics xii) Conclusion Chapter -

Butch, Femme, Dyke, Or Lipstick, Aren't All Lesbians the Same?: an Exploration of Labels and "Looks" Among Lesbians in the U.S
University of Mississippi eGrove Electronic Theses and Dissertations Graduate School 2013 Butch, Femme, Dyke, Or Lipstick, Aren't All Lesbians The Same?: An Exploration Of Labels And "Looks" Among Lesbians In The U.S. South Danielle Kerr University of Mississippi Follow this and additional works at: https://egrove.olemiss.edu/etd Part of the Sociology Commons Recommended Citation Kerr, Danielle, "Butch, Femme, Dyke, Or Lipstick, Aren't All Lesbians The Same?: An Exploration Of Labels And "Looks" Among Lesbians In The U.S. South" (2013). Electronic Theses and Dissertations. 1153. https://egrove.olemiss.edu/etd/1153 This Thesis is brought to you for free and open access by the Graduate School at eGrove. It has been accepted for inclusion in Electronic Theses and Dissertations by an authorized administrator of eGrove. For more information, please contact [email protected]. BUTCH, FEMME, DYKE, OR LIPSTICK, AREN'T ALL LESBIANS THE SAME? AN EXPLORATION OF LABELS AND "LOOKS" AMONG LESBIANS IN THE U.S. SOUTH A Thesis presented in partial fulfillment of requirements for the degree of Master of Arts in the Department of Sociology and Anthropology The University of Mississippi by DANIELLE E. KERR August 2013 Copyright Danielle E. Kerr 2013 ALL RIGHTS RESERVED ABSTRACT This thesis is an exploratory qualitative sociological analysis of gender, sexuality, and race among “out” lesbians in the U.S. South. In this thesis, I explore the following questions: (1) what labels are self-identified lesbians in the South using and/or applying to themselves, and how do they use them? (2) How do they talk about and experience their dress as a part of their identity? (3) How are lesbians doing gender and sexuality in both private and professional environments? (4) How does Southern location influence lesbians’ conceptualization of their gender and sexuality? This research expands current understandings in the literature regarding the complex intersections of gender, sexual identity, and race in a Southern lesbian group. -

Toolkit to Support Child Welfare Agencies in Serving LGBTQ Children, Youth, and Families Table of Contents
Toolkit to Support Child Welfare Agencies in Serving LGBTQ Children, Youth, and Families TABLE OF COnTenTs Introduction ........................................................................................................... 3 Purpose and Structure ................................................................................................................. 3 Creating a Culturally Competent Environment ............................................. 4 Readiness Assessments ............................................................................................................... 4 LGBTQ Policies/Guidelines/Procedures ................................................................................. 5 Building Cultural Competence .................................................................................................. 6 Best Practices for Supporting LGBTQ Children, Youth, and Families ...... 7 Education......................................................................................................................................... 7 Normalcy ......................................................................................................................................... 8 LGBTQ Families ............................................................................................................................. 9 Health, Well-Being, and Development .................................................................................. 10 Training Curricula ...............................................................................................11 -

Authorized Abbreviations, Brevity Codes, and Acronyms
Army Regulation 310–50 Military Publications Authorized Abbreviations, Brevity Codes, and Acronyms Headquarters Department of the Army Washington, DC 15 November 1985 Unclassified USAPA EPS - * FORMAL * TF 2.45 05-21-98 07:23:12 PN 1 FILE: r130.fil SUMMARY of CHANGE AR 310–50 Authorized Abbreviations, Brevity Codes, and Acronyms This revision-- o Contains new and revised abbreviations, brevity codes , and acronyms. o Incorporates chapter 4, sections I and II of the previous regulation into chapters 2 and 3. o Redesignates chapter 5 of the previous regulation as chapter 4. USAPA EPS - * FORMAL * TF 2.45 05-21-98 07:23:13 PN 2 FILE: r130.fil Headquarters Army Regulation 310–50 Department of the Army Washington, DC 15 November 1985 Effective 15 November 1985 Military Publications Authorized Abbreviations, Brevity Codes, and Acronyms has been made to highlight changes from the a p p r o v a l f r o m H Q D A ( D A A G – A M S – P ) , earlier regulation dated 15February 1984. ALEX, VA 22331–0301. Summary. This regulation governs Depart- m e n t o f t h e A r m y a b b r e v i a t i o n s , b r e v i t y Interim changes. Interim changes to this codes, and acronyms. regulation are not official unless they are au- thenticated by The Adjutant General. Users Applicability. This regulation applies to el- will destroy interim changes on their expira- ements of the Active Army, Army National Guard, and U.S. -
Kentish Dialect
A Dictionary of the KENTISH DIALECT © 2008 KENT ARCHAEOLOGICAL SOCIETY 'A Dictionary of the Kentish Dialect and Provincialisms: in use in the county of Kent' by W.D.Parish and W.F.Shaw (Lewes: Farncombe,1888) 'The Dialect of Kent: being the fruits of many rambles' by F. W. T. Sanders (Private limited edition, 1950). Every attempt was made to contact the author to request permission to incorporate his work without success. His copyright is hereby acknowledged. 'A Dictionary of Kentish Dialect and Provincialisms' : in use in the county of Kent by W.D.Parish and W.F.Shaw (Lewes: Farncombe,1888) Annotated copy by L. R. Allen Grove and others (1977) 'The Dialect of Kent in the 14th Century by Richard Morris' (Reprinted from Archaeologia Cantiana Vol VI, 1863) With thanks to the Centre for Kentish Studies, County Hall, Maidstone, Kent Database by Camilla Harley Layout and design © 2008 Kent Archaeological Society '0D RABBIT IT od rab-it it interj. A profane expression, meaning, "May God subvert it." From French 'rabattre'. A Dictionary of the Kentish Dialect and Provincialisms (1888)Page 11 AAZES n.pl. Hawthorn berries - S B Fletcher, 1940-50's; Boys from Snodland, L.R A.G. 1949. (see also Haazes, Harves, Haulms and Figs) Notes on 'A Dictionary of Kentish Dialect & Provincialisms' (c1977)Page 1 ABED ubed adv. In bed. "You have not been abed, then?" Othello Act 1 Sc 3 A Dictionary of the Kentish Dialect and Provincialisms (1888)Page 1 ABIDE ubie-d vb. To bear; to endure; to tolerate; to put-up-with. -

Dubbing Culture: Indonesian Gay and Lesbi Subjectivities and Ethnography in an Already Globalized World
TOM BOELLSTORFF University of California, Irvine Dubbing culture: Indonesian Gay and Lesbi Subjectivities and Ethnography in an already globalized world ABSTRACT s the 20th century begins to recede into historical memory, “glo- balization” presents itself as a completed project: We appear to In this article I explore how Indonesians come to live in a world that is already globalized (Appadurai 1996; Gibson- see themselves as lesbi or gay through fragmentary Graham 1996; Hannerz 1989; Miller 1995). Even with this state of encounters with mainstream mass media (rather affairs, however, globalization is more than background noise. than lesbian and gay Westerners or Western lesbian AAlthough a certain academic fatigue has set in concerning globalization, and gay media). By placing this ethnographic mate- these processes are shifting and intensifying and so demand our continuing rial alongside a recent debate on the dubbing of attention. Ethnography has an important role to play in such a refocused foreign television programs into the Indonesian analysis, for it can show how even the most apparently “remote” communi- language, I develop a theoretical framework of ties are caught up in globalizing processes in ways that impact subjectivities “dubbing culture” to critically analyze globalizing as well as social circumstances (e.g., Tsing 1993). processes. [globalization, homosexuality, identity, Such are the foundational concerns of this article. In it, I bring an analy- Indonesia, mass media, nationalism, postcolonial] sis of how Indonesians come to think of themselves as lesbi or gay through encounters with mass media, together with a late 1990s controversy over the dubbing of foreign television shows and films into the Indonesian language, in order to develop a framework for rethinking ethnography in an already globalized world. -

Student Workbook for Oral Interpretation Bos Been Writ- Ten to Fulfill a Twofold Need at Kansas State College
WOHXBOOK FOR ORAL KJTKRI'RSTATIOH OLADSS &HA!iDT GOUM 3, S., flortiawetern UniTrereity, 1934 A THESIS submitted In pwtlal fulfillment of the rog J.p©a8:it8 for U» degree of uasteh op scnaras rjeporteient of Speech nASSAS STATE COLLH0E OP AQHICOLTORE AMD APPLIED SCISI3CE 1947 Oocu- menf li LD .71 TABLE OF COBTKBTS 'W IH7R0DUCTI0H 1 MATERIALS ASD SSETBODB 4 REVEST OP LITERATURE • « 7 BOUT 13 Articulation and Enunciation, .......... 15 Pronunciation ................. 4 85 Audibility. 73 Word Moaning and Sound. 77 Words In Halation to Ideas. ........... OS Ueaning and Interpretation. 109 Suggestions for the Listeners* Unjaynent. .... 145 WMMARY, 195 AaafCWIfiWEHKHTS 199 HEFEREHCES 200 APPfflror 201 IOTRQDUCTIOE Along with the raany aocial changes which have talton place In the African home during the twentieth century is the tend- ency toward decentralisation of the fanily group ao a unit of entertainment. Instead of the entire fatally gathering around the organ in the parlor to sing songs after dinner, a later has & "date" to see tiie musical cosaedy at the local oiisema; brother dashes off to bond practice? raothor turns on the radio to listen to Wayne King; and dad goes back to the office. In the past, the raenibers of the foaily hurried thren^ their after-dinner duties In order again to gather around tlie dining room table while the laap was placed near oothor or dad and "the book" was taken from the shelf wriore It had been plaoed tlie night before. Then, through the reading of nagio words by their parents, tlie faiaily heard the next exciting chapter of "A Tale of Two Cities," or another section of the "Illlad," Tlie lamp on tlie table faded away and tlir^ugh the oral inter- pretation of a story, they wore carried in their ijaaglnation to Paris, to anclont Greoce, to adventure and, most important of all, to an appreciation for tlie sound of good literature.