Neurology History and Physical Guidelines
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
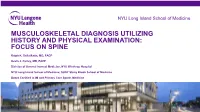
Musculoskeletal Diagnosis Utilizing History and Physical Examination: Focus on Spine
NYU Long Island School of Medicine MUSCULOSKELETAL DIAGNOSIS UTILIZING HISTORY AND PHYSICAL EXAMINATION: FOCUS ON SPINE Ralph K. Della Ratta, MD, FACP Kevin J. Curley, MD, FACP Division of General Internal Medicine, NYU Winthrop Hospital NYU Long Island School of Medicine, SUNY Stony Brook School of Medicine Board Certified in IM and Primary Care Sports Medicine Learning Objectives 1. Identify components of the focused history and physical examination that will guide musculoskeletal diagnosis 2. Utilize musculoskeletal examination provocative maneuvers to aide differential diagnosis 3. Review the evidence base (likelihood ratios etc.) that is known about musculoskeletal physical examination 2 NYU Long Island School of Medicine * ¾ of medical diagnoses are still made on history and exam despite technological Musculoskeletal Physical Exam advances of modern medicine • Physical examination is key to musculoskeletal diagnosis • Unlike many other organ systems, the diagnostic standard for many musculoskeletal disorders is the exam finding (e.g. diagnosis of epicondylitis, see below) • “You may think you have not seen it, but it has seen you!” Lateral Epicondylitis confirmed on exam by reproducing pain at lateral epicondyle with resisted dorsiflexion at wrist **not diagnosed with imaging** 3 NYU Long Island School of Medicine Musculoskeletal Physical Exam 1. Inspection – symmetry, swelling, redness, deformity 2. Palpation – warmth, tenderness, crepitus, swelling 3. Range of motion *most sensitive for joint disease Bates Pocket Guide to Physical -

EPA Quick Reference Guide
EPA Quick Reference Guide EPAs 1 & 2 – Professionalism Unacceptable • Unreliable • Dishonest • Avoids responsibility • Commitment uncertain • Dresses inappropriately • Unexplained absences • Verbal and non-verbal disrespect towards preceptor • Does not recognize own limitations and the need to seek assistance • Unable to comprehend the point of view and emotional state of other people • Judgmental of others • Fails to recognize and respect cross-cultural and gender differences Minimally Competent • Sometimes late • Not consistently able to complete assignments or tasks • Not consistently considerate of the feelings and emotional needs of others • Sometimes judgmental Competent • Punctual • Dependable • Accepts responsibilities • Demonstrates a willingness to accept feedback regarding necessary change(s) • Appropriately shows concern for others’ feelings and interacts accordingly • Recognizes and respects cross-cultural and gender differences Office of Medical Education 306 Liberty View Lane, Lynchburg, Va. 24502 [email protected] EPAs 3 & 4 – Data Gathering / Interviewing & Physical Examination Skills Unacceptable • Inefficient, disorganized • Weak prioritization skills • Misses major findings • Fails to appreciate physical findings and pertinent information • History and/or physical exam incomplete or inaccurate • Insufficient attention to psychosocial issues • Needs to work on establishing rapport with patients • Needs to work on awareness of appropriate boundaries with patients • Needs to improve demonstration of compassion • -
Clinical Reasoning - the Process of Thinking and Decision Making, Consciously & Unconsciously Guide Practice Actions
Diagnostic Reasoning “DR” Toolbox for Hospitalist Faculty Heather Hofmann, MD Department of Medicine 2017-18 2 Goal Increase faculty familiarity with diagnostic reasoning principles and tools so as to improve its teaching. Three Parts: I: Introduction to Diagnostic Reasoning II: DR Toolbox III: Structured Reflection Exercise (SRE) 4 Part I: Introduction to Diagnostic Reasoning Learning Objectives - Understand the “what” and “why” of Diagnostic Reasoning - Recognize dual-process theory’s role in “how” we reason 6 What is Diagnostic Reasoning? - Clinical reasoning - The process of thinking and decision making, consciously & unconsciously guide practice actions 25yo female G1P0, 2m gestation returns from Rio. - Diagnostic reasoning: - The process of collecting & analyzing information establish a diagnosis chest pain STEMI in proximal LAD abdominal pain acute appendicitis 7 Why teach diagnostic reasoning? - Incorrect diagnoses are often at the root of medical errors - DR is a means to apply basic science to clinical problems - Central to being a physician 8 Patient’s perspective What’s wrong with me? Is it bad? What can we do about it? 9 Why now? Never too early for practice 10 From Novice to Expert 11 How do we reason? Information processing theory 12 How do we reason? Information processing theory: Dual process theory. Analytical Non-analytical Conscious Unconscious Type/System 2 Type/System 1 Slow Fast Effortful Automatic Deliberative Involuntary Logical Emotional Requires attention, Executes skilled self-control, time. response and -

(June 2000) I. INTRODUCTION WHAT IS DOCUMENTATION and WHY
DRAFT EVALUATION & MANAGEMENT DOCUMENTATION GUIDELINES (June 2000) I. INTRODUCTION WHAT IS DOCUMENTATION AND WHY IS IT IMPORTANT? Medical record documentation is required to record pertinent facts, findings, and observations about an individual's health history including past and present illnesses, examinations, tests, treatments, and outcomes. The medical record chronologically documents the care of the patient and is an important element contributing to high quality care. The medical record facilitates: · the ability of the physician and other health care professionals to evaluate and plan the patient's immediate treatment, and to monitor his/her health care over time. · communication and continuity of care among physicians and other health care professionals involved in the patient's care; · accurate and timely claims review and payment; · appropriate utilization review and quality of care evaluations; and · collection of data that may be useful for research and education. An appropriately documented medical record can reduce many of the "hassles" associated with claims processing and may serve as a legal document to verify the care provided, if necessary. WHAT DO PAYERS WANT AND WHY? Because payers have a contractual obligation to enrollees, they may require reasonable documentation that services are consistent with the insurance coverage provided. They may request information to validate: · the site of service; · the medical necessity and appropriateness of the diagnostic and/or therapeutic services provided; and/or · that services provided have been accurately reported. II. GENERAL PRINCIPLES OF MEDICAL RECORD DOCUMENTATION The principles of documentation listed below are applicable to all types of medical and surgical Pg. 1 services in all settings. For Evaluation and Management (E/M) services, the nature and amount of physician work and documentation varies by type of service, place of service and the patient's status. -

Outcome and Assessment Information Set OASIS-D Guidance Manual Effective January 1, 2019
Outcome and Assessment Information Set OASIS-D Guidance Manual Effective January 1, 2019 Centers for Medicare & Medicaid Services PRA Disclosure Statement According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is x. The time required to complete this information collection is estimated to average 0.3 minutes per response, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. This estimate does not include time for training. If you have comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850. *****CMS Disclaimer*****Please do not send applications, claims, payments, medical records or any documents containing sensitive information to the PRA Reports Clearance Office. Please note that any correspondence not pertaining to the information collection burden approved under the associated OMB control number listed on this form will not be reviewed, forwarded, or retained. If you have questions or concerns regarding where to submit your documents, please contact Joan Proctor National Coordinator, Home Health Quality Reporting Program Centers for Medicare & Medicaid. OASIS-D Guidance Manual Table of Contents Page -
Diagnosis and Management of Chlamydia: a Guide for Gps
■ PRESCRIBING IN PRACTICE Diagnosis and management of chlamydia: a guide for GPs ELEANOR DRAEGER SPL Chlamydia is a common sexually- transmitted infection caused by Chlamydia trachomatis bacteria. This article discusses its diagnosis and treatment, and considers the GP’s role in management. hlamydia is the most common sexually-transmitted infection C(STI) in the UK, with 203,116 new diagnoses in England in 2017, of which 126,828 (62%) were in young people aged 15–24 years.1 Chlamydia is transmitted primarily through penetrative sex and infects the urethra and endocervix. It can also infect the throat and the rectum, and in some cases the conjunctiva. It is very infectious, with a concordance of up to 75% between sexual partners. There are many risk factors for chlamydia infection, including being under the age of 25 years, having a new sexual partner and inconsistent use of condoms. If a woman contracts chlamydia during pregnancy it can be transmitted to the baby at delivery, causing conjunctivitis or pneumonia. Classification of chlamydia infections There are three species of chlamydia bacteria that can cause disease in humans: • Chlamydia psittaci – the natural host is birds, especially par- rots, but it can be transmitted to humans, causing psittacosis • Chlamydia pneumoniae – causes respiratory disease in humans • Chlamydia trachomatis – several different serovars can cause disease (including STIs) in humans, as detailed in Figure 1. Symptoms The majority of genital chlamydia infections are asymptomatic, but they can cause significant symptoms. In women, chlamydia can cause vaginal discharge, dysuria, abdominal and pelvic pain, post-coital and intermenstrual bleeding, and deep dys- pareunia. -

The Contribution of the Medical History for the Diagnosis of Simulated Cases by Medical Students
International Journal of Medical Education. 2012;3:78-82 ISSN: 2042-6372 DOI: 10.5116/ijme.4f8a.e48c The contribution of the medical history for the diagnosis of simulated cases by medical students Tomoko Tsukamoto, Yoshiyuki Ohira, Kazutaka Noda, Toshihiko Takada, Masatomi Ikusaka Department of General Medicine, Chiba University Hospital, Japan Correspondence: Tomoko Tsukamoto, Department of General Medicine, Chiba University Hospital, 1-8-1 Inohana, Chuo-ku, Chiba city, Chiba, 260-8677 Japan. Email: [email protected] Accepted: April 15, 2012 Abstract Objectives: The case history is an important part of diag- rates were compared using analysis of the χ2-test. nostic reasoning. The patient management problem method Results: Sixty students (63.8%) made a correct diagnosis, has been used in various studies, but may not reflect the which was based on the history in 43 students (71.7%), actual reasoning process because a list of choices is given to physical findings in 11 students (18.3%), and laboratory the subjects in advance. This study investigated the contri- data in 6 students (10.0%). Compared with students who bution of the history to making the correct diagnosis by considered the correct diagnosis in their differential diagno- using clinical case simulation, in which students obtained sis after taking a history, students who failed to do so were clinical information by themselves. 5.0 times (95%CI = 2.5-9.8) more likely to make a final Methods: A prospective study was conducted. Ninety-four misdiagnosis (χ2(1) = 30.73; p<0.001). fifth-year medical students from Chiba University who Conclusions: History taking is especially important for underwent supervised clinical clerkships in 2009 were making a correct diagnosis when students perform clinical surveyed. -

Peripheral Arterial Disease | Piedmont Healthcare
Peripheral Arterial Disease CLAUDICATION TO LIMB THREATENING ISCHEMIA THE HOW AND WHEN TO EVALUATE AND TREAT Brian M Freeman MD FACS Nothing to Disclose PAD: Peripheral Arterial Disease Obstruction of any “peripheral artery” Causes – Atherosclerosis – Emboli – Extrinsic compression – Vasculitis PAD Effects more than 15 million Americans Majority of patients are asymptomatic African Americans and Hispanics are at risk Diabetics with PAD are at significant risk for amputations (Neuropathy + PAD) PAD Risk Factors PAD: PREVALENCE vs AGE PAD: More Prevalent and More Deadly Than Many Leading Diseases Disease Prevalence (Millions) Five-Year Mortality Rate 5 50% 17.0 4 40% 39% 30% 3 30% 28% 12.6 12.0 8.9 21% 2 4.8 20% 5.0 14% 4.0 1 10% 0 0% Diabetes Coronary PAD Cancer CHF Stroke Alzheimers Colorectal PAD Stroke CAD Breast Heart Cancer Cancer Disease Source: American Cancer Society, American Heart Association, Alzheimers Disease Education/Referral Center, American Diabetes Association, SAGE Group PAD: LONG-TERM MORTALITY Atherosclerosis is a Systemic Disease Lesion Location Consequence Carotid, cerebral Stroke Aorta, arch Aneurysm Coronary artery MI Renal artery HTN, CRF Mesenteric Bowel infarct Iliac artery Impotence Femoral artery Claudication Tibial artery Limb loss PAD There is a 5 fold increase in the relative risk of a Cardiovascular ischemic event Total Mortality is increased 2-3 X Visual Cues to PAD and Arterial Insufficiency Cool, dry, atrophic skin on legs Thickened or deformed nails-dystrophic Hair loss or uneven distribution on legs -

The Oral Presentation Nersi Nikakhtar, M.D
Guidelines for the Oral Presentation Nersi Nikakhtar, M.D. University of Minnesota Medical School !1 Table of Contents The Oral Presentation: An Introduction ..................................3 Why Worry About the Oral Presentation? ...............................4 Presenting the New Patient .....................................................5 The Opening Statement ......................................................5 History of Present Illness ....................................................5 Past Medical History ...........................................................6 Medications/Allergies ..........................................................7 Social and Family History ...................................................7 Review of Systems ..............................................................7 Vitals .....................................................................................8 Physical Exam .....................................................................8 Labs and Studies .................................................................8 Summary Statement ............................................................8 Assessment and Plan ..........................................................9 The Follow Up (or Daily) Presentation: What's Different? ...................................................................11 The Outpatient (Known Patient) Presentation: What's Different? ...................................................................12 !2 The Oral Presentation: An Introduction The -

The Patient Interview
CHAPTER 1 The Patient Interview Sneha Baxi Srivastava, PharmD, BCACP LEARNING OBJECTIVES • Explain the basic communication skills needed when performing a patient interview. • Describe the components of the patient interview. • Conduct a thorough medication history. • Compare and contrast the different patient interview approaches in various clinical settings. • Adapt the interview technique based on the needs of the patient. KEY TERMS • Active Listening • Pertinent Positive • Rapport • Pertinent Negative • Empathy • Past History • Open-Ended Questions • Medication History • Leading Questions • Family History • Probing Questions • Personal and Social History • Nonverbal Communication • Review of Systems • Chief Complaint • Physical Exam • History of Present Illness • QuEST/SCHOLAR-MAC INTRODUCTION The patient interview is the primary way of obtaining comprehensive information about the patient in order to provide effective patient-centered care, and the medica- tion history component is the pharmacist’s expertise. A methodological approach is used to obtain information from the patient, usually starting with determining the patient’s chief complaint, also known as the reason for the healthcare visit, and then 2 CHAPTER 1 / The Patient Interview delving further into an exploration of the patient’s specific complaint and problem. A comprehensive patient interview includes inquiring about the patient’s medical, medication, social, personal, and family history, as well as a thorough review of systems and possibly a physical examination. The medication history is the part of the patient interview that provides the pharmacist the opportunity to utilize his or her expertise by precisely collecting each component of the medication history (however, a medication history may also be collected independent of a comprehensive patient interview). -
The AOA Guide
The AOA Guide: How to Succeed in the Third-Year Clerkships Example Notes for the MSIII 2017 Preface This guide was created as a way of assisting you as you start your clinical training. For the rest of your professional life, you will write various notes. Although they will eventually become second nature to you, it is often challenging at first to figure out what information is pertinent to a particular specialty/rotation.This book is designed to help you through that process. In this book you will find samples of SOAP notes for each specialty and a complete History and Physical. Each of these notes represents very typical patients you will see on the rotation. Look at the way the notes are phrased and the information they contain. We have included an abbre- viations page at the end of this book so that you can refer to it for the short-forms with which you are not yet familiar. Pretty soon you will be using these abbrevia- tions without a problem! These notes can be used as a template from which you can adjust the information to apply to your patient. It is important to remember that these notes are not all inclusive, of course, and other physicians will give sugges- tions that you should heed. If you are ever having trouble, us fourth year medical students are always willing to help! ***NOTE: Many note-writing practices at Jefferson may change as the hospital transitions from paper notes to EMR.*** Table of Contents Internal Medicine Progress Note (SOAP) ............................................................3 Neurology Progress Note (SOAP) ...................................................................... -

Assessment of an Adult Living with HIV
The fundamentals of the clinical assessment of an adult living with HIV Note: Pictures have been removed from the slides for copyright purposes Talitha Crowley (Stellenbosch University) Helen Woolgar (Stellenbosch University) Stacie Stender (Jhpiego) 2 Overview 1. Reasons for performing a clinical assessment 2. Approach to a clinical assessment 3. Subjective history taking 4. Objective examination 5. Assessment and plan 6. Summary 1. Discuss why a clinical assessment should be performed on a HIV infected patient. 2. Recognise possible abnormal findings from a subjective history as well as a physical examination. 3. Make an accurate patient assessment and develop an appropriate care plan. 4 Reasons for performing an assessment A study in Pretoria about • Establish baseline data about the the quality of services in ART clinics found that a patient’s health when diagnosed physical assessment was with HIV and before starting ART. performed in only 41.1% of patients (Kinkel et al. 2012) • Identify opportunistic infections that needs treatment. • Identify any other chronic conditions that may develop while a patient is on ART. 5 Approach to a clinical assessment • Subjective - history taking • Objective - physical examination • Assessment of subjective and objective findings and differential diagnosis • Plan 6 Comprehensive assessment • Subjective: History Taking e.g. previous illness, symptoms • Objective: General assessment, JACCOL, basic data, systems examination, diagnostic tests / investigations • Assessment: Diagnosis & WHO stage • Plan: