Efficacy of Central Nervous System Prophylaxis with Stand-Alone
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Primary Effusion Lymphoma Without an Effusion: a Rare Case of Solid Extracavitary Variant of Primary Effusion Lymphoma in an HIV-Positive Patient
Hindawi Case Reports in Hematology Volume 2018, Article ID 9368451, 5 pages https://doi.org/10.1155/2018/9368451 Case Report Primary Effusion Lymphoma without an Effusion: A Rare Case of Solid Extracavitary Variant of Primary Effusion Lymphoma in an HIV-Positive Patient Hamza Hashmi ,1 Drew Murray,1 Samer Al-Quran ,2 and William Tse3 1Division of Hematology and Oncology, University of Louisville, Louisville, KY, USA 2Department of Pathology and Laboratory Medicine, University of Louisville, Louisville, KY, USA 3Division of Blood and Marrow Transplant, University of Louisville, Louisville, KY, USA Correspondence should be addressed to Hamza Hashmi; [email protected] Received 26 August 2017; Revised 5 December 2017; Accepted 27 December 2017; Published 28 January 2018 Academic Editor: Tatsuharu Ohno Copyright © 2018 Hamza Hashmi et al. )is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Primary effusion lymphoma (PEL) is a unique form of non-Hodgkin lymphoma, usually seen in severely immunocompromised, HIV-positive patients. PEL is related to human herpesvirus-8 (HHV-8) infection, and it usually presents as a lymphomatous body cavity effusion in the absence of a solid tumor mass. )ere have been very few case reports of HIV-positive patients with HHV-8- positive solid tissue lymphomas not associated with an effusion (a solid variant of PEL). In the absence of effusion, establishing an accurate diagnosis can be challenging, and a careful review of morphology, immunophenotype, and presence of HHV-8 is necessary to differentiate from other subtypes of non-Hodgkin lymphoma. -

And Cisplatin-Resistant Ovarian Cancer
Vol. 2, 607–610, July 2003 Molecular Cancer Therapeutics 607 Alchemix: A Novel Alkylating Anthraquinone with Potent Activity against Anthracycline- and Cisplatin-resistant Ovarian Cancer Klaus Pors, Zennia Paniwnyk, mediated stabilization of the topo II-DNA-cleavable complex Paul Teesdale-Spittle,1 Jane A. Plumb, and resulting in inhibition of poststrand passage DNA religa- Elaine Willmore, Caroline A. Austin, and tion (1). This event is not lethal per se but initiates a cascade 2 Laurence H. Patterson of events leading to cell death (2). Anthraquinones, as ex- Department of Pharmaceutical and Biological Chemistry, The School of emplified by mitoxantrone, are topo II inhibitors with proven Pharmacy, University of London, London WC1N 1AX, United Kingdom [K. P., L. H. P.]; Department of Pharmacy, De Montfort University, success for the treatment of advanced breast cancer, non- Leicester LE1 9BH, United Kingdom [Z. P., P. T. S.]; Cancer Research Hodgkin’s lymphoma, and acute leukemia (3). Intercalation is UK Department of Medical Oncology, University of Glasgow, Glasgow a crucial part of topo II inhibition by cytotoxic anthraquinones G61 1BD, United Kingdom [J. A. P.]; and School of Cell and Molecular Biosciences, The Medical School, University of Newcastle upon Tyne, with high affinity for DNA (4). It is likely that the potent Newcastle upon Tyne NE2 4HH, United Kingdom [E. W., C. A. A.] cytotoxicity of anthraquinones is related to their slow rate of dissociation from DNA, the kinetics of which favors long- term trapping of the topo-DNA complexes (5). However, Abstract currently available DNA intercalators at best promote a tran- Chloroethylaminoanthraquinones are described with sient inhibition of topo II, because the topo-drug-DNA ter- intercalating and alkylating capacity that potentially nary complex is reversed by removal of the intracellular drug covalently cross-link topoisomerase II (topo II) to DNA. -

BC Cancer Protocol Summary for Treatment of Lymphoma with Dose- Adjusted Etoposide, Doxorubicin, Vincristine, Cyclophosphamide
BC Cancer Protocol Summary for Treatment of Lymphoma with Dose- Adjusted Etoposide, DOXOrubicin, vinCRIStine, Cyclophosphamide, predniSONE and riTUXimab with Intrathecal Methotrexate Protocol Code LYEPOCHR Tumour Group Lymphoma Contact Physician Dr. Laurie Sehn Dr. Kerry Savage ELIGIBILITY: One of the following lymphomas: . Patients with an aggressive B-cell lymphoma and the presence of a dual translocation of MYC and BCL2 (i.e., double-hit lymphoma). Histologies may include DLBCL, transformed lymphoma, unclassifiable lymphoma, and intermediate grade lymphoma, not otherwise specified (NOS). Patients with Burkitt lymphoma, who are not candidates for CODOXM/IVACR (such as those over the age of 65 years, or with significant co-morbidities) . Primary mediastinal B-cell lymphoma Ensure patient has central line EXCLUSIONS: . Cardiac dysfunction that would preclude the use of an anthracycline. TESTS: . Baseline (required before first treatment): CBC and diff, platelets, BUN, creatinine, bilirubin. ALT, LDH, uric acid . Baseline (required, but results do not have to be available to proceed with first treatment): results must be checked before proceeding with cycle 2): HBsAg, HBcoreAb, . Baseline (optional, results do not have to be available to proceed with first treatment): HCAb, HIV . Day 1 of each cycle: CBC and diff, platelets, (and serum bilirubin if elevated at baseline; serum bilirubin does not need to be requested before each treatment, after it has returned to normal), urinalysis for microscopic hematuria (optional) . Days 2 and 5 of each cycle (or days of intrathecal treatment): CBC and diff, platelets, PTT, INR . For patients on cyclophosphamide doses greater than 2000 mg: Daily urine dipstick for blood starting on day cyclophosphamide is given. -

HODGKIN LYMPHOMA TREATMENT REGIMENS (Part 1 of 2)
HODGKIN LYMPHOMA TREATMENT REGIMENS (Part 1 of 2) The selection, dosing, and administration of anticancer agents and the management of associated toxicities are complex. Drug dose modifications and schedule and initiation of supportive care interventions are often necessary because of expected toxicities and because of individual patient variability, prior treatment, and comorbidities. Thus, the optimal delivery of anticancer agents requires a healthcare delivery team experienced in the use of such agents and the management of associated toxicities in patients with cancer. The cancer treatment regimens below may include both FDA-approved and unapproved uses/regimens and are provided as references only to the latest treatment strategies. Clinicians must choose and verify treatment options based on the individual patient. NOTE: GREY SHADED BOXES CONTAIN UPDATED REGIMENS. REGIMEN DOSING Classical Hodgkin Lymphoma—First-Line Treatment General treatment note: Routine use of growth factors is not recommended. Leukopenia is not a factor for treatment delay or dose reduction (except for escalated BEACOPP).1 CR=complete response IPS=International Prognostic Score PD=progressive disease PFTs=pulmonary function tests PR=partial response RT=radiation therapy SD=stable disease Stage IA, IIA Favorable ABVD (doxorubicin [Adriamycin] Days 1 and 15: Doxorubicin 25mg/m2 IV + bleomycin 10mg/m2 IV + vinblastine + bleomycin + vinblastine + 6mg/m2 IV + dacarbazine 375mg/m2 IV. dacarbazine [DTIC-Dome]) + Repeat cycle every 4 weeks for 2–4 cycles. involved-field radiotherapy (IFRT)1–4 Follow with IFRT after completion of chemotherapy. Abbreviated Stanford V Weeks 1, 3, 5 and 7: Vinblastine 6mg/m2 IV + doxorubicin 25mg/m2 IV. (doxorubicin + vinblastine + Weeks 1 and 5: Mechlorethamine 6mg/m2. -

(Rituxan®), Rituximab-Abbs (Truxima®), Rituximab-Pvvr (Ruxience®) Prior Authorization Drug Coverage Policy
1 Rituximab Products: Rituximab (Rituxan®), Rituximab-abbs (Truxima®), Rituximab-pvvr (Ruxience®) Prior Authorization Drug Coverage Policy Effective Date: 2/1/2021 Revision Date: n/a Review Date: 7/2/20 Lines of Business: Commercial Policy type: Prior Authorization This Drug Coverage Policy provides parameters for the coverage of rituximab (Rituxan®), rituximab-abbs (Truxima®), and rituximab-pvvr (Ruxience®). Consideration of medically necessary indications are based upon U.S. Food and Drug Administration (FDA) indications, recommended uses within the Centers of Medicare & Medicaid Services (CMS) five recognized compendia, including the National Comprehensive Cancer Network (NCCN) Drugs & Biologics Compendium (Category 1 or 2A recommendations), and peer-reviewed scientific literature eligible for coverage according to the CMS, Medicare Benefit Policy Manual, Chapter 15, section 50.4.5 titled, “Off- Label Use of Anti-Cancer Drugs and Biologics.” This policy evaluates whether the drug therapy is proven to be effective based on published evidence-based medicine. Drug Description1-3 Rituximab (Rituxan®), rituximab-abbs (Truxima®), and rituximab-pvvr (Ruxience®) are monoclonal antibodies that target the CD20 antigen expressed on the surface of pre-B and mature B- lymphocytes. Upon binding to cluster of differentiation (CD) 20, rituximab mediates B-cell lysis. Possible mechanisms of cell lysis include complement dependent cytotoxicity (CDC) and antibody dependent cell mediated cytotoxicity (ADCC). B cells are believed to play a role in the pathogenesis of rheumatoid arthritis (RA) and associated chronic synovitis. In this setting, B cells may be acting at multiple sites in the autoimmune/inflammatory process, including through production of rheumatoid factor (RF) and other autoantibodies, antigen presentation, T-cell activation, and/or proinflammatory cytokine production. -
R-Chop-21 / Chop-21
Lymphoma group R-CHOP-21 / CHOP-21 INDICATION Lymphoma Omit rituximab if CD20-negative. TREATMENT INTENT Curative or disease modification depending on clinical circumstances PRE-ASSESSMENT 1. Ensure histology is confirmed prior to administration of chemotherapy and document in notes. 2. Record stage and IPI of disease - CT scan (neck, chest, abdomen and pelvis), and/or PET- CT, presence or absence of B symptoms, clinical extent of disease, consider bone marrow aspirate and trephine. 3. Blood tests – FBC, U&Es, LDH, ESR, urate, calcium, Vitamin D level,magnesium, creatinine, LFTs, glucose, Igs, β2 microglobulin, hepatitis B core antibody and hepatitis B surface Ag, hepatitis C antibody, EBV, CMV, VZV, HIV 1+2 after consent, group and save. 4. Urine pregnancy test • before cycle 1 of each new chemotherapy course for women of child- bearing age unless they are post-menopausal, have been sterilised or undergone a hysterectomy. 5. ECG +/- Echo and baseline BP in all patients with a cardiac history or at risk of cardiac complications (hypertension, smokers, diabetes). 6. Record performance status (WHO/ECOG). 7. Record height and weight. 8. Consent - ensure patient has received adequate verbal and written information regarding their disease, treatment and potential side effects. Document in medical notes all information that has been given. Obtain written consent on the day of treatment. 9. Fertility - it is very important the patient understands the potential risk of infertility. All patients should be offered fertility advice by referring to the Oxford Fertility Unit. 10. Hydration – in patients with bulky disease pre-hydrate with sodium chloride 0.9% 1 litre over 4- 6 hours. -

Anaplastic Large Cell Lymphoma (ALCL)
Helpline (freephone) 0808 808 5555 [email protected] www.lymphoma-action.org.uk Anaplastic large cell lymphoma (ALCL) This page is about anaplastic large-cell lymphoma (ALCL), a type of T-cell lymphoma. On this page What is ALCL? Who gets it? Symptoms Treatment Relapsed and refractory ALCL Research and targeted treatments We have separate information about the topics in bold font. Please get in touch if you’d like to request copies or if you would like further information about any aspect of lymphoma. Phone 0808 808 5555 or email [email protected]. What is ALCL? Anaplastic large cell lymphoma (ALCL) is a type of T-cell lymphoma – a non-Hodgkin lymphoma that develops from white blood cells called T cells. Under a microscope, the cancerous cells in ALCL look large, undeveloped and very abnormal (‘anaplastic’). There are four main types of ALCL. They have complicated names based on their features and the types of proteins they make: • ALK-positive ALCL (also known as ALK+ ALCL) is the most common type. In ALK-positive ALCL, the abnormal T cells have a genetic change (mutation) that means they make a protein called ‘anaplastic lymphoma kinase’ (ALK). In other words, they test positive for ALK. ALK-positive ALCL is a fast-growing (high-grade) lymphoma. Page 1 of 6 © Lymphoma Action • ALK-negative ALCL (also known as ALK- ALCL) is a high-grade lymphoma that accounts for around 3 in every 10 cases of ALCL. The abnormal T cells do not make the ALK protein – they test negative for ALK. -

5-Fluorouracil + Adriamycin + Cyclophosphamide) Combination in Differentiated H9c2 Cells
Article Doxorubicin Is Key for the Cardiotoxicity of FAC (5-Fluorouracil + Adriamycin + Cyclophosphamide) Combination in Differentiated H9c2 Cells Maria Pereira-Oliveira, Ana Reis-Mendes, Félix Carvalho, Fernando Remião, Maria de Lourdes Bastos and Vera Marisa Costa * UCIBIO, REQUIMTE, Laboratory of Toxicology, Faculty of Pharmacy, University of Porto, Rua de Jorge Viterbo Ferreira, 228, 4050-313 Porto, Portugal; [email protected] (M.P.-O.); [email protected] (A.R.-M.); [email protected] (F.C.); [email protected] (F.R.); [email protected] (M.L.B.) * Correspondence: [email protected] Received: 4 October 2018; Accepted: 3 January 2019; Published: 10 January 2019 Abstract: Currently, a common therapeutic approach in cancer treatment encompasses a drug combination to attain an overall better efficacy. Unfortunately, it leads to a higher incidence of severe side effects, namely cardiotoxicity. This work aimed to assess the cytotoxicity of doxorubicin (DOX, also known as Adriamycin), 5-fluorouracil (5-FU), cyclophosphamide (CYA), and their combination (5-Fluorouracil + Adriamycin + Cyclophosphamide, FAC) in H9c2 cardiac cells, for a better understanding of the contribution of each drug to FAC-induced cardiotoxicity. Differentiated H9c2 cells were exposed to pharmacological relevant concentrations of DOX (0.13–5 μM), 5-FU (0.13–5 μM), CYA (0.13–5 μM) for 24 or 48 h. Cells were also exposed to FAC mixtures (0.2, 1 or 5 μM of each drug and 50 μM 5-FU + 1 μM DOX + 50 μM CYA). DOX was the most cytotoxic drug, followed by 5-FU and lastly CYA in both cytotoxicity assays (reduction of 3-(4,5-dimethylthiazol-2- yl)-2,5-diphenyl tetrazolium bromide (MTT) and neutral red (NR) uptake). -
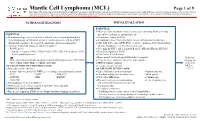
Mantle Cell Lymphoma (MCL)
Mantle Cell Lymphoma (MCL) Page 1 of 9 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. PATHOLOGIC DIAGNOSIS INITIAL EVALUATION ESSENTIAL: ● Physical exam: attention to node-bearing areas, including Waldeyer's ring, ESSENTIAL: size of liver and spleen, and patient’s age ● Hematopathology review of all slides with at least one tumor paraffin block. ● Performance status (ECOG) Hematopathology confirmation of classic versus aggressive variant of MCL ● B symptoms (fever, drenching night sweats, unintentional weight loss) (blastoid/pleomorphic). Re-biopsy if consult material is non-diagnostic. ● CBC with differential, LDH, BUN, creatinine, albumin, AST, total bilirubin, 1 ● Adequate immunophenotype to confirm diagnosis alkaline phosphatase, serum calcium, uric acid ○ Paraffin panel: ● Screening for HIV 1 and 2, hepatitis B and C (HBcAb, HBaAg, HCVAb) - Pan B-cell marker (CD19, CD20, PAX5), CD3, CD5, CD10, and cyclin D1 ● Beta-2 microglobulin (B2M) - Ki-67 (proliferation rate) ● Chest x-ray, PA and lateral or ● Bone marrow bilateral biopsy with unilateral aspirate Induction ○ Flow cytometry immunophenotyping: -

NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines® ) Non-Hodgkin’S Lymphomas Version 2.2015
NCCN Guidelines Index NHL Table of Contents Discussion NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines® ) Non-Hodgkin’s Lymphomas Version 2.2015 NCCN.org Continue Version 2.2015, 03/03/15 © National Comprehensive Cancer Network, Inc. 2015, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN® . Peripheral T-Cell Lymphomas NCCN Guidelines Version 2.2015 NCCN Guidelines Index NHL Table of Contents Peripheral T-Cell Lymphomas Discussion DIAGNOSIS SUBTYPES ESSENTIAL: · Review of all slides with at least one paraffin block representative of the tumor should be done by a hematopathologist with expertise in the diagnosis of PTCL. Rebiopsy if consult material is nondiagnostic. · An FNA alone is not sufficient for the initial diagnosis of peripheral T-cell lymphoma. Subtypes included: · Adequate immunophenotyping to establish diagnosisa,b · Peripheral T-cell lymphoma (PTCL), NOS > IHC panel: CD20, CD3, CD10, BCL6, Ki-67, CD5, CD30, CD2, · Angioimmunoblastic T-cell lymphoma (AITL)d See Workup CD4, CD8, CD7, CD56, CD57 CD21, CD23, EBER-ISH, ALK · Anaplastic large cell lymphoma (ALCL), ALK positive (TCEL-2) or · ALCL, ALK negative > Cell surface marker analysis by flow cytometry: · Enteropathy-associated T-cell lymphoma (EATL) kappa/lambda, CD45, CD3, CD5, CD19, CD10, CD20, CD30, CD4, CD8, CD7, CD2; TCRαβ; TCRγ Subtypesnot included: · Primary cutaneous ALCL USEFUL UNDER CERTAIN CIRCUMSTANCES: · All other T-cell lymphomas · Molecular analysis to detect: antigen receptor gene rearrangements; t(2;5) and variants · Additional immunohistochemical studies to establish Extranodal NK/T-cell lymphoma, nasal type (See NKTL-1) lymphoma subtype:βγ F1, TCR-C M1, CD279/PD1, CXCL-13 · Cytogenetics to establish clonality · Assessment of HTLV-1c serology in at-risk populations. -

Cardioprotective Effects of Exercise Training on Doxorubicin-Induced
www.nature.com/scientificreports OPEN Cardioprotective efects of exercise training on doxorubicin‑induced cardiomyopathy: a systematic review with meta‑analysis of preclinical studies Paola Victória da Costa Ghignatti, Laura Jesuíno Nogueira, Alexandre Machado Lehnen & Natalia Motta Leguisamo* Doxorubicin (DOX)‑induced cardiotoxicity in chemotherapy is a major treatment drawback. Clinical trials on the cardioprotective efects of exercise in cancer patients have not yet been published. Thus, we conducted a systematic review and meta‑analysis of preclinical studies for to assess the efcacy of exercise training on DOX‑induced cardiomyopathy. We included studies with animal models of DOX‑induced cardiomyopathy and exercise training from PubMed, Web of Sciences and Scopus databases. The outcome was the mean diference (MD) in fractional shortening (FS, %) assessed by echocardiography between sedentary and trained DOX‑treated animals. Trained DOX‑treated animals improved 7.40% (95% CI 5.75–9.05, p < 0.001) in FS vs. sedentary animals. Subgroup analyses revealed a superior efect of exercise training execution prior to DOX exposure (MD = 8.20, 95% CI 6.27–10.13, p = 0.010). The assessment of cardiac function up to 10 days after DOX exposure and completion of exercise protocol was also associated with superior efect size in FS (MD = 7.89, 95% CI 6.11–9.67, p = 0.020) vs. an echocardiography after over 4 weeks. Modality and duration of exercise, gender and cumulative DOX dose did were not individually associated with changes on FS. Exercise training is a cardioprotective approach in rodent models of DOX‑induced cardiomyopathy. Exercise prior to DOX exposure exerts greater efect sizes on FS preservation. -

Advances in Llm
LLM ADVANCES IN LLM Current Developments in the Management of Leukemia, Lymphoma, and Myeloma Section Editor: Susan O’Brien, MD Prophylaxis of Central Nervous System Relapse in Patients With Lymphoma Avyakta Kallam, MD Assistant Professor, Internal Medicine Division of Oncology & Hematology University of Nebraska Medical Center Omaha, Nebraska H&O How common is central nervous system AK Patients can be asymptomatic at the time of diag- relapse in lymphoma? nosis. When symptoms do occur, they can be subtle, and include nonspecific headaches, blurred vision, and AK The incidence of central nervous system (CNS) mild confusion. Overt symptoms include cranial nerve relapse in lymphoma depends on the type of disease. In palsies and focal neurologic deficits, such as weakness more-aggressive, high-grade lymphomas, such as Burkitt and imbalance. lymphoma and lymphoblastic lymphoma, the rate of Imaging studies, such as magnetic resonance imaging CNS relapse can reach 30% to 50%. In diffuse large of the brain, can help detect the presence of CNS involve- B-cell lymphoma, CNS involvement occurs in approxi- ment. The diagnostic test of choice, however, is lumbar mately 2% to 5% of patients. puncture with flow cytometry of the cerebral spinal fluid. H&O What are the risk factors? H&O Does CNS relapse impact prognosis? AK The validated Central Nervous System–International AK CNS relapse confers a poor prognosis in patients with Prognostic Index (CNS-IPI) scoring system is used to lymphoma, particularly diffuse large B-cell lymphoma. identify patients who are at high risk for CNS relapse. The median overall survival in a patient who develops The scoring system takes into account 6 characteristics: CNS relapse is approximately 3 to 4 months.