Download This PDF File
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Thrombotic Thrombocytopenic Purpura and Systemic Lupus Erythematosus: Successful Management of a Rare Presentation
Indian J Crit Care Med July-September 2008 Vol 12 Issue 3 Case Report Thrombotic thrombocytopenic purpura and systemic lupus erythematosus: Successful management of a rare presentation Pratish George, Jasmine Das, Basant Pawar1, Naveen Kakkar2 Thrombotic thrombocytopenic purpura (TTP) and systemic lupus erythematosus (SLE) very rarely present simultaneously and pose a diagnostic and therapeutic dilemma to the critical care team. Prompt diagnosis and management with plasma exchange and immunosuppression is life-saving. A patient critically ill with TTP and SLE, successfully managed in the acute period of illness with plasma exchange, steroids and Abstract mycophenolate mofetil is described. Key words: Plasma exchange, systemic lupus erythematosus, thrombotic thrombocytopenic purpura Introduction Case Report Systemic lupus erythematosis (SLE) is diagnosed by A 30-year-old lady was admitted with fever and the presence of four or more of the following criteria, jaundice. A week earlier she had undergone an serially or simultaneously: malar rash, discoid rash, uncomplicated medical termination of pregnancy at photosensitivity, oral ulcers, non erosive arthritis, serositis, another hospital, at 13 weeks of gestation. She had an renal abnormalities including proteinuria or active urinary uneventful pregnancy with twins two years earlier and sediments, neuropsychiatric features, hematological the twins were diagnosed to have thalassemia major. abnormalities including hemolytic anemia, leucopenia, She was subsequently diagnosed to have thalassemia lymphopenia and thrombocytopenia, immunological minor and her husband had thalassemia minor trait. No markers like anti-ds DNA or anti-Smith antibody and high earlier history of spontaneous Þ rst trimester abortions Antinuclear antibody titres. Thrombotic thrombocytopenic was present. purpura (TTP) in patients with SLE is extremely rare. -

Interstitial Granuloma Annulare Triggered by Lyme Disease
Volume 27 Number 5| May 2021 Dermatology Online Journal || Case Presentation 27(5):11 Interstitial granuloma annulare triggered by Lyme disease Jordan Hyde1 MD, Jose A Plaza1,2 MD, Jessica Kaffenberger1 MD Affiliations: 1Division of Dermatology, The Ohio State University Wexner Medical Center, Columbus, Ohio, USA, 2Department of Pathology, The Ohio State University Wexner Medical Center, Columbus, Ohio, USA Corresponding Author: Jessica Kaffenberger MD, Division of Dermatology, The Ohio State University Medical Wexner Medical Center, Suite 240, 540 Officenter Place, Columbus, OH 43230, Tel: 614-293-1707, Email: [email protected] been associated with a variety of systemic diseases Abstract including diabetes mellitus, malignancy, thyroid Granuloma annulare is a non-infectious disease, dyslipidemia, and infection [3,4]. granulomatous skin condition with multiple different associations. We present a case of a man in his 60s There are multiple histological variants of GA, with a three-week history of progressive targetoid including interstitial GA. The histopathology of plaques on his arms, legs, and trunk. Skin biopsy classic GA demonstrates a focal degeneration of demonstrated interstitial granuloma annulare. collagen surrounded by an inflammatory infiltrate Additional testing revealed IgM antibodies to Borrelia composed of lymphocytes and histiocytes. In a less burgdorferi on western blot suggesting interstitial common variant, interstitial GA, scattered histiocytes granuloma annulare was precipitated by the recent are seen -

2017 Oregon Dental Conference® Course Handout
2017 Oregon Dental Conference® Course Handout Nasser Said-Al-Naief, DDS, MS Course 8125: “The Mouth as The Body’s Mirror: Oral, Maxillofacial, and Head and Neck Manifestations of Systemic Disease” Thursday, April 6 2 pm - 3:30 pm 2/28/2017 The Mouth as The Body’s Mirror Oral Maxillofacial and Head and Neck Manifestation of Ulcerative Conditions of Allergic & Immunological Systemic Disease the Oro-Maxillofacial Diseases Region Nasser Said-Al-Naief, DDS, MS Professor & Chair, Oral Pathology and Radiology Director, OMFP Laboratory Oral manifestations of Office 503-494-8904// Direct: 503-494-0041 systemic diseases Oral Manifestations of Fax: 503-494-8905 Dermatological Diseases Cell: 1-205-215-5699 Common Oral [email protected] Conditions [email protected] OHSU School of Dentistry OHSU School of Medicine 2730 SW Moody Ave, CLSB 5N008 Portland, Oregon 97201 Recurrent aphthous stomatitis (RAS) Recurrent aphthous stomatitis (RAS) • Aphthous" comes from the Greek word "aphtha”- • Recurrence of one or more painful oral ulcers, in periods of days months. = ulcer • Usually begins in childhood or adolescence, • The most common oral mucosal disease in North • May decrease in frequency and severity by age America. (30+). • Affect 5% to 66% of the North American • Ulcers are confined to the lining (non-keratinized) population. mucosa: • * 60% of those affected are members of the • Buccal/labial mucosa, lateral/ventral tongue/floor of professional class. the mouth, soft palate/oropharyngeal mucosa • Etiopathogenesis: 1 2/28/2017 Etiology of RAU Recurrent Aphthous Stomatitis (RAS): Types: Minor; small size, shallow, regular, preceeded by prodrome, heal in 7-10 days Bacteria ( S. -

Immune-Pathophysiology and -Therapy of Childhood Purpura
Egypt J Pediatr Allergy Immunol 2009;7(1):3-13. Review article Immune-pathophysiology and -therapy of childhood purpura Safinaz A Elhabashy Professor of Pediatrics, Ain Shams University, Cairo Childhood purpura - Overview vasculitic disorders present with palpable Purpura (from the Latin, purpura, meaning purpura2. Purpura may be secondary to "purple") is the appearance of red or purple thrombocytopenia, platelet dysfunction, discolorations on the skin that do not blanch on coagulation factor deficiency or vascular defect as applying pressure. They are caused by bleeding shown in table 1. underneath the skin. Purpura measure 0.3-1cm, A thorough history (Table 2) and a careful while petechiae measure less than 3mm and physical examination (Table 3) are critical first ecchymoses greater than 1cm1. The integrity of steps in the evaluation of children with purpura3. the vascular system depends on three interacting When the history and physical examination elements: platelets, plasma coagulation factors suggest the presence of a bleeding disorder, and blood vessels. All three elements are required laboratory screening studies may include a for proper hemostasis, but the pattern of bleeding complete blood count, peripheral blood smear, depends to some extent on the specific defect. In prothrombin time (PT) and activated partial general, platelet disorders manifest petechiae, thromboplastin time (aPTT). With few exceptions, mucosal bleeding (wet purpura) or, rarely, central these studies should identify most hemostatic nervous system bleeding; -

A Patient with Plaque Type Morphea Mimicking Systemic Lupus Erythematosus
CASE REPORT A Patient With Plaque Type Morphea Mimicking Systemic Lupus Erythematosus Wardhana1, EA Datau2 1 Department of Internal Medicine, Siloam International Hospitals. Karawaci, Indonesia. 2 Department of Internal Medicine, Prof. Dr. RD Kandou General Hospital & Sitti Maryam Islamic Hospital, Manado, North Sulawesi, Indonesia. Correspondence mail: Siloam Hospitals Group’s CEO Office, Siloam Hospital Lippo Village. 5th floor. Jl. Siloam No.6, Karawaci, Indonesia. email: [email protected] ABSTRAK Morfea merupakan penyakit jaringan penyambung yang jarang dengan gambaran utama berupa penebalan dermis tanpa disertai keterlibatan organ dalam. Penyakit ini juga dikenal sebagai bagian dari skleroderma terlokalisir. Berdasarkan gambaran klinis dan kedalaman jaringan yang terlibat, morfea dikelompokkan ke dalam beberapa bentuk dan sekitar dua pertiga orang dewasa dengan morfea mempunyai tipe plak. Produksi kolagen yang berlebihan oleh fibroblast merupakan penyebab kelainan pada morfea dan mekanisme terjadinya aktivitas fibroblast yang berlebihan ini masih belum diketahui, meskipun beberapa mekanisme pernah diajukan. Morfe tipe plak biasanya bersifat ringan dan dapat sembuh dengan sendirinya. Morfea tipe plak yang penampilan klinisnya menyerupai lupus eritematosus sistemik, misalnya meliputi alopesia dan ulkus mukosa di mulut, jarang dijumpai. Sebuah kasus morfea tipe plak pada wanita berusia 20 tahun dibahas. Pasien ini diobati dengan imunosupresan dan antioksidan local maupun sistemik. Kondisi paisen membaik tanpa disertai efek samping yang berarti. Kata kunci: morfea, tipe plak. ABSTRACT Morphea is an uncommon connective tissue disease with the most prominent feature being thickening or fibrosis of the dermal without internal organ involvement. It is also known as a part of localized scleroderma. Based on clinical presentation and depth of tissue involvement, morphea is classified into several forms, and about two thirds of adults with morphea have plaque type. -
Nodular Morphea
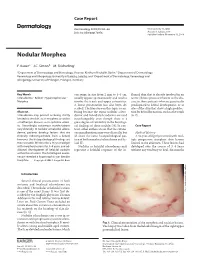
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable. -
Thrombocytopenia.Pdf
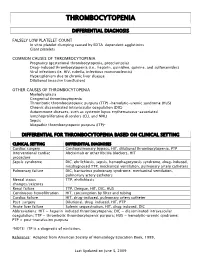
THROMBOCYTOPENIA DIFFERENTIAL DIAGNOSIS FALSELY LOW PLATELET COUNT In vitro platelet clumping caused by EDTA-dependent agglutinins Giant platelets COMMON CAUSES OF THROMBOCYTOPENIA Pregnancy (gestational thrombocytopenia, preeclampsia) Drug-induced thrombocytopenia (i.e., heparin, quinidine, quinine, and sulfonamides) Viral infections (ie. HIV, rubella, infectious mononucleosis) Hypersplenism due to chronic liver disease Dilutional (massive transfusion) OTHER CAUSES OF THROMBOCYTOPENIA Myelodysplasia Congenital thrombocytopenia Thrombotic thrombocytopenic purpura (TTP) -hemolytic-uremic syndrome (HUS) Chronic disseminated intravascular coagulation (DIC) Autoimmune diseases, such as systemic lupus erythematosus-associated lymphoproliferative disorders (CLL and NHL) Sepsis Idiopathic thrombocytopenic purpura (ITP)* DIFFERENTIAL FOR THROMBOCYTOPENIA BASED ON CLINICAL SETTING CLINICAL SETTING DIFFERENTIAL DIAGNOSES Cardiac surgery Cardiopulmonary bypass, HIT, dilutional thrombocytopenia, PTP Interventional cardiac Abciximab or other IIb/IIIa blockers, HIT procedure Sepsis syndrome DIC, ehrlichiosis, sepsis, hemophagocytosis syndrome, drug-induced, misdiagnosed TTP, mechanical ventilation, pulmonary artery catheters Pulmonary failure DIC, hantavirus pulmonary syndrome, mechanical ventilation, pulmonary artery catheters Mental status TTP, ehrlichiosis changes/seizures Renal failure TTP, Dengue, HIT, DIC, HUS Continuous hemofiltration HIT, consumption by filter and tubing Cardiac failure HIT, drug-induced, pulmonary artery catheter Post-surgery -

Pathobiology of Thrombocytopenia and Bleeding in Patients with Wiskott-Aldrich Syndrome
TITLE: Pathobiology of Thrombocytopenia and Bleeding in Patients with Wiskott-Aldrich Syndrome Principal Investigator: James B. Bussel, MD IRB Protocol Number: 0801009600 ClinicalTrials.gov ID: NCT00909363 Compound Number: SB-497115 Development Phase: Phase II Effective Date: August 26th 2010 Updated: September 18, 2015 Protocol Versions: August 15, 2013 October 28, 2014 December 31, 2014 July 7, 2015 1 TABLE OF CONTENTS List of Abbreviations 4 1 INTRODUCTION 5 1.1 Background 5 1.2 Rationale 5 2 OBJECTIVE(S) 6 2.1 Primary Objective 6 2.2 Secondary Objectives 6 3 INVESTIGATIONAL PLAN 6 3.1 Study Design 6 3.2 Laboratory Testing 7 4 SUBJECT SELECTION AND WITHDRAWAL CRITERIA 8 4.1 Number of Subjects 8 4.2 Inclusion Criteria 8 4.3 Exclusion Criteria 8 4.4 Withdrawal Criteria 9 4.4.1 Study Stopping Rules 10 4.4.2 Patient Stopping Rules 10 5 STUDY TREATMENTS 10 5.1 Treatment Assignment 10 5.2 Product Accountability 11 5.3 Treatment Compliance 11 5.4 Concomitant Medications and Non-Drug Therapies 11 5.4.1 Permitted Medications and Non-Drug Therapies 11 5.4.2 Prohibited Medications and Non-Drug Therapies 11 5.5 Treatment after the End of the Study 11 5.6 Treatment of Investigational Product Overdose 11 5.7 Treatment Plan 12 6 STUDY ASSESSMENTS AND PROCEDURES 13 6.1 Critical Baseline Assessments 13 6.2 Efficacy 13 6.3 Safety 13 6.3.1 Liver chemistry stopping and follow-up criteria 15 6.4 Adverse Events 16 6.4.1 Definition of an AE 16 6.4.2 Definition of a SAE 17 6.4.3 Disease-Related Events and/or Disease-Related Outcomes Not Qualifying as SAEs -

Acute Immune Thrombocytopenic Purpura in Children
Turk J Hematol 2007; 24:41-51 REVIEW ARTICLE © Turkish Society of Hematology Acute immune thrombocytopenic purpura in children Abdul Rehman Sadiq Public School, Bahawalpur, Pakistan [email protected] Received: Sep 12, 2006 • Accepted: Mar 21, 2007 ABSTRACT Immune thrombocytopenic purpura (ITP) in children is usually a benign and self-limiting disorder. It may follow a viral infection or immunization and is caused by an inappropriate response of the immune system. The diagnosis relies on the exclusion of other causes of thrombocytopenia. This paper discusses the differential diagnoses and investigations, especially the importance of bone marrow aspiration. The course of the disease and incidence of intracranial hemorrhage are also discussed. There is substantial discrepancy between published guidelines and between clinicians who like to over-treat. The treatment of the disease ranges from observation to drugs like intrave- nous immunoglobulin, steroids and anti-D to splenectomy. The different modes of treatment are evaluated. The best treatment seems to be observation except in severe cases. Key Words: Thrombocytopenic purpura, bone marrow aspiration, Intravenous immunoglobulin therapy, steroids, anti-D immunoglobulins 41 Rehman A INTRODUCTION There is evidence that enhanced T-helper cell/ Immune thrombocytopenic purpura (ITP) in APC interactions in patients with ITP may play an children is usually a self-limiting disorder. The integral role in IgG antiplatelet autoantibody pro- American Society of Hematology (ASH) in 1996 duction -

Immune Thrombocytopenic Purpura (ITP) — Adult Conditions for Which Ivig Has an Established Therapeutic Role
Immune thrombocytopenic purpura (ITP) — adult Conditions for which IVIg has an established therapeutic role. Specific Conditions Newly Diagnosed Immune thrombocytopenic purpura (ITP) Persistent Immune thrombocytopenic purpura (ITP) Chronic Immune thrombocytopenic purpura (ITP) Evans syndrome ‐ with significant Immune thrombocytopenic purpura (ITP) ‐ adult Indication for IVIg Use Newly diagnosed ITP — initial Ig therapy ITP in pregnancy — initial Ig therapy ITP with life‐threatening haemorrhage or the potential for life‐threatening haemorrhage Newly diagnosed or persistent ITP — subsequent therapy (diagnosis <12 months) Refractory persistent or chronic ITP — splenectomy failed or contraindicated and second‐line agent unsuccessful Subsequent or ongoing treatment for ITP responders during pregnancy and the postpartum period ITP and inadequate platelet count for planned surgery HIV‐associated ITP Level of Evidence Evidence of probable benefit – more research needed (Category 2a) Description and Diagnostic Immune thrombocytopenic purpura (ITP) is a reduction in platelet count Criteria (thrombocytopenia) resulting from shortened platelet survival due to anti‐platelet antibodies, reduced platelet production due to immune induced reduced megakaryopoeisis and/or immune mediated direct platelet lysis. When counts are very low (less than 30x109/L), bleeding into the skin (purpura) and mucous membranes can occur. Bone marrow platelet production (megakaryopoiesis) is morphologically normal. In some cases, there is additional impairment of platelet function related to antibody binding to glycoproteins on the platelet surface. It is a common finding in patients with human immunodeficiency virus (HIV) disease, and while it may be found at any stage of the infection, its prevalence increases as HIV disease advances. Around 80 percent of adults with ITP have the chronic form of disease. -

S2 Table. List of Syntax for 96 Diseases
S2 Table. List of syntax for 96 diseases 'autoimmune gastritis'/exp OR 'acantholysis'/exp OR 'acantholysis' OR 'acute disseminated encephalomyelitis'/exp OR 'adem (acute disseminated encephalomyelitis)' OR 'acute disseminated encephalitis' OR 'acute disseminated encephalomyelitis' OR 'encephalitis postvaccinalis' OR 'encephalitis, post-vaccinal' OR 'encephalomyelitis, acute disseminated' OR 'post vaccinal encephalitis' OR 'post vaccination encephalitis' OR 'post-infectious encephalitis' OR 'post-infectious encephalomyelitis' OR 'postinfection encephalitis' OR 'postinfectious encephalitis' OR 'postinfectious encephalomyelitis' OR 'postvaccinal encephalitis' OR 'postvaccinal encephalopathy' OR 'postvaccination encephalitis' OR 'postvaccine encephalitis' OR 'postvaccinial encephalitis' OR 'postvaccinial encephalomyelitis' OR 'smallpox vaccination encephalitis' OR 'vaccinal encephalitis' OR 'vaccination encephalopathy' OR 'vaccination post vaccinial encephalitis' OR 'vaccinia encephalitis' OR 'addison disease'/exp OR 'addison disease' OR 'addison`s disease' OR 'addisons disease' OR 'addison biermer disease' OR 'adult onset still disease'/exp OR 'adult onset still disease' OR 'still`s disease, adult- onset' OR 'allergic glomerulonephritis'/exp OR 'allergic glomerulonephritis' OR 'glomerulonephritis, allergic' OR 'glomerulonephritis, poststreptococcal' OR 'post streptococcal glomerulonephritis' OR 'poststreptococcal glomerulonephritis' OR 'anca associated vasculitis'/exp OR 'anca associated vasculitis' OR 'anca vasculitis' OR 'anca-associated -

Thrombotic Thrombocytopenic Purpura: Pathophysiology, Diagnosis, and Management
Journal of Clinical Medicine Review Thrombotic Thrombocytopenic Purpura: Pathophysiology, Diagnosis, and Management Senthil Sukumar 1 , Bernhard Lämmle 2,3,4 and Spero R. Cataland 1,* 1 Division of Hematology, Department of Medicine, The Ohio State University, Columbus, OH 43210, USA; [email protected] 2 Department of Hematology and Central Hematology Laboratory, Inselspital, Bern University Hospital, University of Bern, CH 3010 Bern, Switzerland; [email protected] 3 Center for Thrombosis and Hemostasis, University Medical Center, Johannes Gutenberg University, 55131 Mainz, Germany 4 Haemostasis Research Unit, University College London, London WC1E 6BT, UK * Correspondence: [email protected] Abstract: Thrombotic thrombocytopenic purpura (TTP) is a rare thrombotic microangiopathy charac- terized by microangiopathic hemolytic anemia, severe thrombocytopenia, and ischemic end organ injury due to microvascular platelet-rich thrombi. TTP results from a severe deficiency of the specific von Willebrand factor (VWF)-cleaving protease, ADAMTS13 (a disintegrin and metalloprotease with thrombospondin type 1 repeats, member 13). ADAMTS13 deficiency is most commonly acquired due to anti-ADAMTS13 autoantibodies. It can also be inherited in the congenital form as a result of biallelic mutations in the ADAMTS13 gene. In adults, the condition is most often immune-mediated (iTTP) whereas congenital TTP (cTTP) is often detected in childhood or during pregnancy. iTTP occurs more often in women and is potentially lethal without prompt recognition and treatment. Front-line therapy includes daily plasma exchange with fresh frozen plasma replacement and im- munosuppression with corticosteroids. Immunosuppression targeting ADAMTS13 autoantibodies Citation: Sukumar, S.; Lämmle, B.; with the humanized anti-CD20 monoclonal antibody rituximab is frequently added to the initial ther- Cataland, S.R.